Clinical features and management of corneal graft rejection in detail and easy to und6laguage
Reading File
Finding Sources
Finding Sources
Searching PubMed
corneal graft rejection management
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the information needed for a thorough, easy-to-understand response. Let me compile it.
Corneal Graft Rejection - Clinical Features & Management
Sources: Kanski's Clinical Ophthalmology (10th ed.), Wills Eye Manual, Tintinalli's Emergency Medicine
What Is Corneal Graft Rejection?
A corneal graft (transplant) is normally tolerated well because the cornea has no blood vessels and very few immune cells - this is called "immune privilege." However, if the host's immune system recognizes the donor cornea as foreign, it launches an attack - this is graft rejection.
Think of it like this: the body's security system (immune system) finds an intruder (donor cornea) and tries to destroy it.
Rejection is the most common cause of corneal graft failure, accounting for about 31% of all graft losses.
Why Does Rejection Happen? (Pathogenesis)
Normally, the cornea is protected from rejection by:
- No blood vessels (antigens can't be "seen" by immune cells)
- No lymphatics
- Very few antigen-presenting cells
This privilege is LOST when:
- Blood vessels grow into the cornea (neovascularization)
- Inflammation occurs
- The host gets sensitized to HLA antigens on the donor cornea
Once sensitized, T-lymphocytes attack the graft - usually starting at the graft margin (nearest blood vessels) and moving toward the center.
Risk Factors for Rejection
| Risk Factor | Explanation |
|---|---|
| Host stromal vascularization | Blood vessels = immune cells can reach the graft |
| Large or eccentric grafts (>8 mm) | More host-graft interface |
| Previous failed graft | Already sensitized immune system |
| Herpetic infection | Triggers inflammation |
| Glaucoma | Chronic inflammation |
| Gender mismatch | Male donor → female recipient is HIGH RISK |
| HLA mismatch | Minor benefit from matching |
Key pearl: A male donor cornea should NOT be given to a female recipient - this is a newer recognized risk factor.
When Does It Occur?
Rejection can happen any time from 10 days to years after transplant. The timing is very variable. Many cases are asymptomatic until rejection is already established - which is why regular follow-up is so important.
Clinical Features (Symptoms + Signs)
Symptoms (What the Patient Feels)
The classic "RSVP" mnemonic:
- R - Redness
- S - Sensitivity to light (photophobia)
- V - Vision decrease (blurred vision)
- P - Pain (mild)
Many patients have NO symptoms early on and are only caught on routine exam!
Signs (What the Doctor Sees)
Rejection can affect each layer of the cornea separately or together:
1. Epithelial Rejection (mildest)
- An elevated line of abnormal epithelium moves across the cornea
- Occurs around 3 months after surgery
- Eye may look relatively quiet (mild or no inflammation)
- Easiest to treat
2. Subepithelial Rejection
- Krachmer spots - small gray-white subepithelial infiltrates on the donor cornea
- Look like the spots seen in adenoviral eye infection
- Deeper edema and hazy opacification
3. Stromal Rejection
- Deeper stromal haze
- Can be chronic (slowly progressive) or hyperacute (rapid, usually with endothelial rejection)
- Stromal edema = sign of endothelial failure
4. Endothelial Rejection (most serious)
- The MOST DANGEROUS type - endothelial cells don't regenerate!
- Khodadoust line - a characteristic linear row of keratic precipitates (inflammatory deposits) on the endothelium, advancing from the graft margin toward the center
- Corneal edema (graft swells and goes cloudy)
- Anterior chamber reaction (cells and flare)
Clinical image - Corneal graft rejection with keratic precipitates and rejection line:
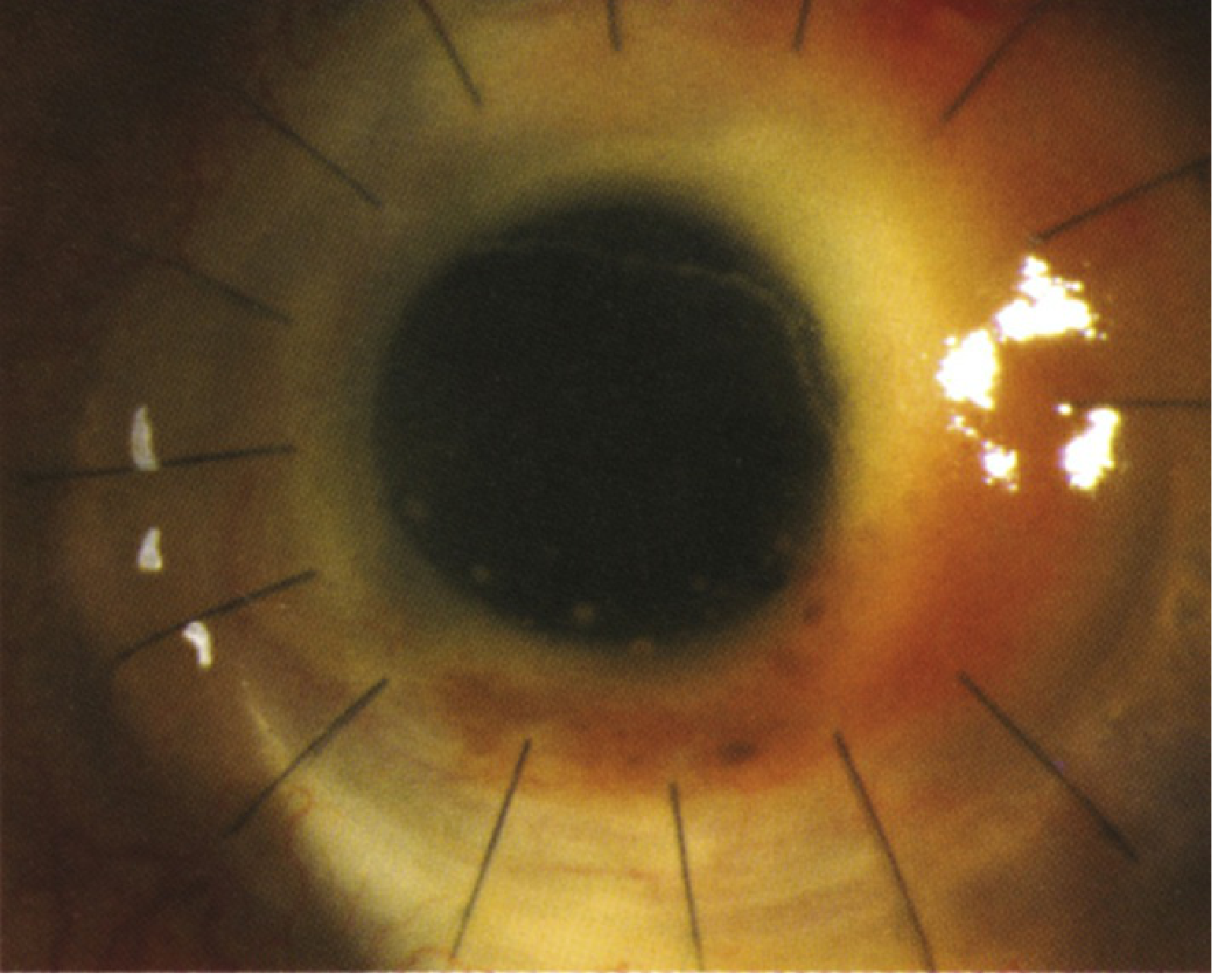
The bright white cluster at the graft margin represents keratic precipitates - inflammatory cells deposited on the endothelium. Note the sutured graft.
Endothelial rejection with Khodadoust line (Kanski's Fig. 8.7D):
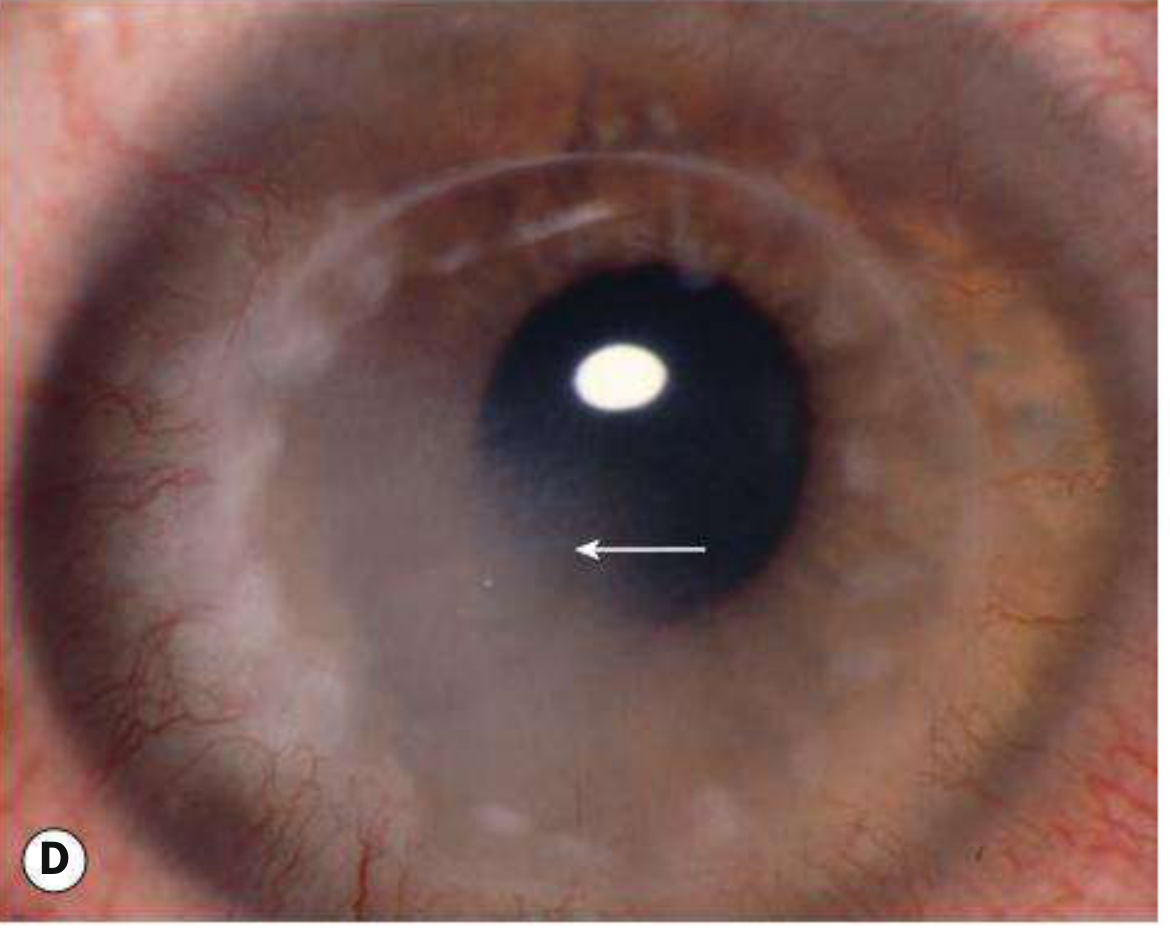
Arrow points to the Khodadoust line - a sweep of keratic precipitates crossing the endothelium. Peripheral white haziness = graft edema. Note the blood vessels around the graft margin.
5. General Signs (Any Type)
- Ciliary injection (redness around the cornea = limbal flush) - often the first visible sign
- Anterior chamber inflammation (cells + flare on slit lamp)
- Neovascularization growing onto the graft
- Broken suture
Summary Table of Rejection Types
| Type | Key Sign | Timing | Severity |
|---|---|---|---|
| Epithelial | Elevated epithelial line | ~3 months | Mild |
| Subepithelial | Krachmer spots | Variable | Mild-moderate |
| Stromal | Stromal haze | Variable | Moderate |
| Endothelial | Khodadoust line + edema | Variable | SEVERE |
Differential Diagnosis
Before treating as rejection, rule out:
- Infective keratitis (bacterial, fungal, herpetic) - look for corneal infiltrate, hypopyon, discharge
- Uveitis - keratic precipitates NOT limited to graft endothelium; history of uveitis
- Suture abscess - focal infiltrate near suture
- Raised IOP - corneal edema without inflammation; clears when IOP controlled
- Epithelial downgrowth - advancing smooth/scalloped line; does NOT respond to steroids
- Non-immune graft failure - no inflammation, just slow clouding
Workup
- Full history - when was the transplant? what eye drops is the patient using? any recent steroid taper? reason for original transplant (HSV history?)
- Slit lamp examination - look for Khodadoust line, Krachmer spots, epithelial line, keratic precipitates
- IOP measurement - always check, steroids can raise it
- Specular microscopy - assess endothelial cell density if available
Management
Golden rule: START TREATMENT IMMEDIATELY. Earlier treatment = better chance of saving the graft.
Treatment is stepped up based on the TYPE and SEVERITY:
For Endothelial Rejection (most aggressive treatment needed)
Step 1 - Topical steroids (first-line, mainstay)
- Prednisolone acetate 1% every hour while awake (for first 24 hours)
- Can also use difluprednate 0.05% every 2 hours
- Add dexamethasone 0.1% ointment at bedtime
- Gradually taper over several weeks as the eye improves
Step 2 - Systemic steroids (for severe/recurrent cases)
- Oral prednisolone 1 mg/kg/day for 1-2 weeks, then taper
- If started within 8 days of onset: IV methylprednisolone 500 mg/day for up to 3 days - this is especially effective and reduces risk of further episodes
Step 3 - Cycloplegia
- Homatropine 2% or atropine 1%, once or twice daily
- Dilates pupil, reduces pain from ciliary spasm, prevents synechiae
Step 4 - Other options for recalcitrant/high-risk cases
- Topical cyclosporine 0.05%-2% (onset is delayed; useful for prevention too)
- Subconjunctival dexamethasone injection (4 mg/mL, 0.5 mL)
- Systemic cyclosporine, tacrolimus, or azathioprine
For Epithelial and Stromal Rejection (less aggressive)
- Double the current topical steroid dose or use prednisolone acetate 1% four times daily (whichever is higher)
- Add cycloplegic and topical cyclosporine as above
IOP Monitoring (critical throughout)
- Steroids raise IOP - must monitor regularly
- If IOP elevated, add topical IOP-lowering drops
- Uncontrolled high IOP can itself cause corneal edema that mimics rejection
Follow-up Schedule
| Phase | Frequency |
|---|---|
| Active rejection | Every 3-7 days |
| Improving | Every 1-2 weeks |
| Stable | Monthly, then every few months |
| Maintenance steroids | Regular IOP checks lifelong |
Once improvement is noted, steroids must be tapered very slowly - sometimes continued at low doses for months to years to prevent recurrence.
Prevention of Rejection
- Maintain long-term low-dose topical steroids in high-risk patients (e.g., prednisolone acetate 1% QID indefinitely)
- Topical cyclosporine as prophylaxis in high-risk cases
- Avoid triggers: treat infections early, manage IOP, prevent suture-related inflammation
- Patient education: know the symptoms of rejection (RSVP) and seek help immediately - hours matter!
Key Take-Home Points
- Rejection can affect epithelium, stroma, or endothelium - endothelial rejection is most serious
- The pathognomonic sign is the Khodadoust line (linear keratic precipitates on the endothelium)
- Symptoms = RSVP (Redness, Sensitivity, Vision loss, Pain) - but many cases are asymptomatic
- Treat immediately and aggressively - delay = irreversible endothelial damage = permanent graft failure
- IV methylprednisolone within 8 days of onset can be particularly effective
- Monitor IOP regularly in all patients on steroid therapy
- Kanski's Clinical Ophthalmology 10th ed., pp. 294-295
- Wills Eye Manual, Ch. 4.28
- Tintinalli's Emergency Medicine, Ch. 241
This is a shared conversation. Sign in to Orris to start your own chat.