Pathogenesis and precepetating factors of dka and hss flowchart simple
A clean medical educational flowchart showing pathogenesis and precipitating factors of DKA (Diabetic Ketoacidosis) and HHS (Hyperosmolar Hyperglycemic State) side by side. Left column - DKA: Title: "DKA - Diabetic Ketoacidosis" Precipitating Factors box (red/orange): Infection, Insulin omission/nonadherence, New-onset T1DM, Acute illness (MI, stroke, pancreatitis), Drugs (steroids, SGLT2i, cocaine), Endocrinopathies (Cushing's, thyrotoxicosis), Surgery/trauma Arrow down to: "Absolute Insulin Deficiency + Counter-regulatory hormone excess (glucagon, cortisol, catecholamines)" Two arrows splitting: Left arrow to: "LIVER: Glycogenolysis + Gluconeogenesis → Hyperglycemia" Right arrow to: "ADIPOSE: Lipolysis → Free Fatty Acids → Liver → Ketogenesis (β-hydroxybutyrate, acetoacetate)" Both arrows converge to: "Osmotic Diuresis → Dehydration + Electrolyte loss" Then: "Metabolic Acidosis (pH <7.3) + Ketonemia/Ketonuria" Final box: "DKA Triad: Hyperglycemia + Ketosis + Acidosis" Right column - HHS: Title: "HHS - Hyperosmolar Hyperglycemic State" Precipitating Factors box (blue): Infection/Sepsis, Serious illness (MI, stroke), Inadequate fluid intake (elderly, debilitated), New-onset T2DM, Medications (diuretics, steroids), Impaired thirst mechanism Arrow down to: "Relative Insulin Deficiency (enough insulin to suppress ketogenesis, not enough to control glucose)" Arrow to: "Hepatic glucose production + Impaired peripheral glucose utilization → Severe Hyperglycemia (>600 mg/dL)" Arrow to: "Osmotic Diuresis → Severe Dehydration (fluid deficit 8-10L) + Electrolyte loss" Arrow to: "Inability to compensate (elderly/debilitated) → Progressive Hemoconcentration + Prerenal azotemia" Final box: "HHS: Severe Hyperglycemia (>600) + Hyperosmolality (>320) + NO significant Ketosis/Acidosis" At the bottom center: Comparison table: Feature | DKA | HHS Glucose | >250 mg/dL | >600 mg/dL pH | <7.3 | Normal/near normal Ketones | +++ | Absent/trace Osmolality | Mildly elevated | >320 mOsm/L Onset | Hours-days | Days-weeks Common in | T1DM | T2DM/elderly Use color coding: orange/red for DKA, blue for HHS. Clean white background, professional medical style, clear arrows and boxes with rounded corners, bold headings.
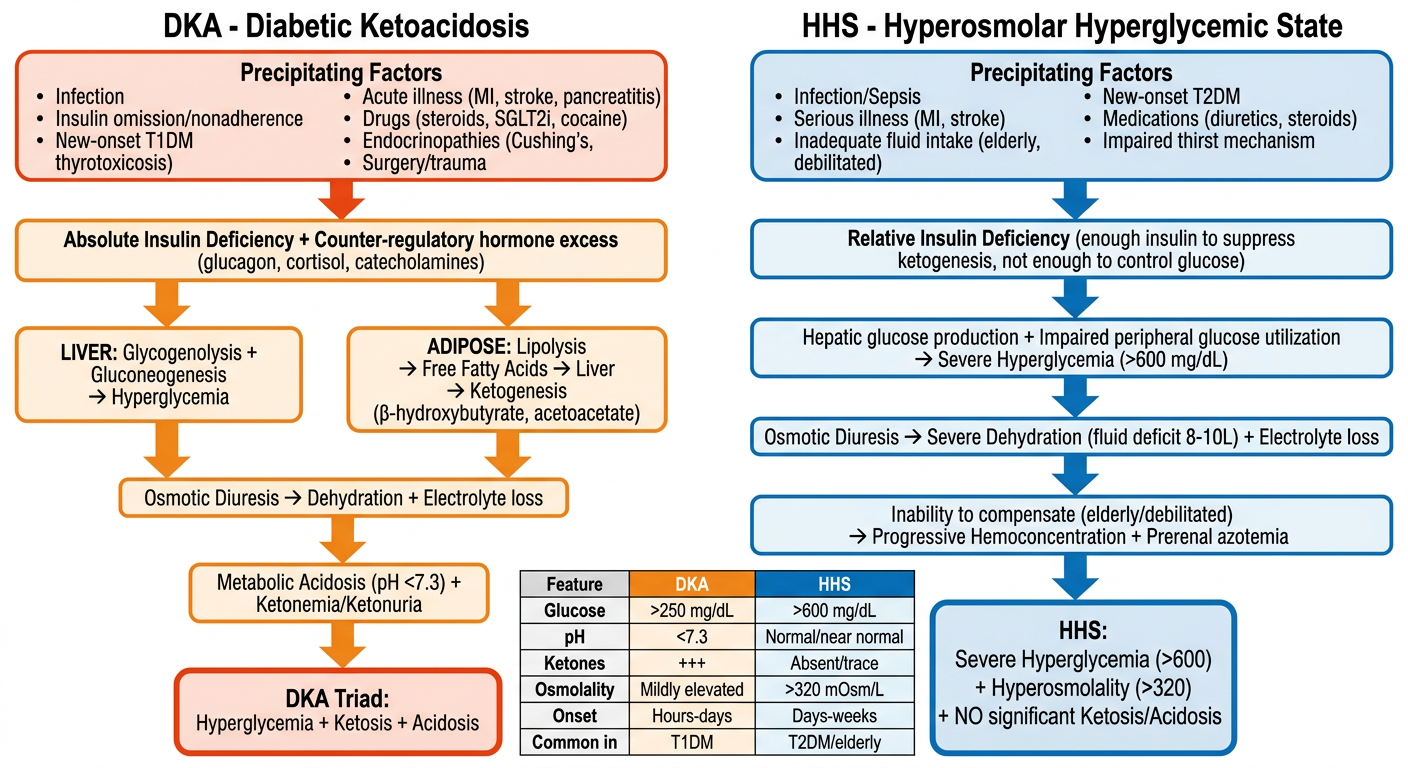
DKA - Pathogenesis
-
Glucose axis - Liver undergoes glycogenolysis and gluconeogenesis (using substrates: amino acids, lactate, pyruvate from muscle; glycerol from fat). Peripheral glucose utilization also falls. Result: hyperglycemia.
-
Ketone axis - Adipose lipolysis releases free fatty acids and glycerol. FFAs reach the liver where beta-oxidation produces ketone bodies: beta-hydroxybutyrate, acetoacetate, and acetone. Without insulin, ketone production far exceeds utilization.
HHS - Pathogenesis
- Severe hyperglycemia (>600 mg/dL, often >1000 mg/dL) develops due to hepatic glucose overproduction + impaired peripheral utilization.
- Osmotic diuresis causes massive fluid loss - deficit typically 8-10L (larger than DKA).
- The elderly/debilitated patient cannot compensate by drinking enough fluid.
- Progressive hemoconcentration + reduced renal glucose excretion → vicious cycle of worsening hyperglycemia and hyperosmolality (>320 mOsm/L).
- No significant ketosis because portal insulin is sufficient to suppress lipolysis.
Precipitating Factors (Common to Both)
| Factor | DKA | HHS |
|---|---|---|
| Infections | Most common | Most common |
| Insulin omission/nonadherence | Very common | Less relevant |
| New-onset diabetes | T1DM | T2DM |
| Acute MI / Stroke | Yes | Yes (major trigger) |
| Acute pancreatitis | Yes | Yes |
| Drugs | Steroids, SGLT2i, cocaine, clozapine, olanzapine, thiazides, lithium | Steroids, thiazides, diuretics |
| Endocrinopathies | Cushing's, thyrotoxicosis, acromegaly | Cushing's |
| Impaired fluid intake | Less common | Key factor (elderly/bedridden) |
| Severe burns / hyperthermia | Yes | Less common |
Key Difference at a Glance
| Feature | DKA | HHS |
|---|---|---|
| Glucose | >250 mg/dL | >600 mg/dL |
| pH | <7.3 | Normal / near-normal |
| Ketones | +++ | Absent or trace |
| Serum osmolality | Mildly elevated | >320 mOsm/L |
| Onset speed | Hours to days | Days to weeks |
| Typical patient | T1DM, younger | T2DM, elderly |
| Mortality | ~1-5% | Up to 15% |
Pathogenesis of dka and hss flow chart simple
A clean, simple medical flowchart showing pathogenesis of DKA and HHS side by side on white background. Simple boxes and arrows, minimal text, professional medical style. LEFT SIDE - DKA (use warm orange/red color scheme): Header box: "DKA — Diabetic Ketoacidosis" ↓ Box: "ABSOLUTE Insulin Deficiency + ↑ Counter-regulatory hormones (glucagon, cortisol, catecholamines)" ↓ splits into TWO arrows: Left path: Box: "↑ Glycogenolysis & Gluconeogenesis (liver)" ↓ Box: "HYPERGLYCEMIA" Right path: Box: "↑ Lipolysis → Free Fatty Acids → Liver" ↓ Box: "KETOGENESIS (β-hydroxybutyrate, acetoacetate)" ↓ Box: "KETONEMIA + ACIDOSIS (pH < 7.3)" Both paths merge down to: Box: "Osmotic Diuresis → Dehydration + Electrolyte Loss" ↓ Final box (bold red border): "DKA TRIAD: Hyperglycemia + Ketosis + Metabolic Acidosis" RIGHT SIDE - HHS (use blue color scheme): Header box: "HHS — Hyperosmolar Hyperglycemic State" ↓ Box: "RELATIVE Insulin Deficiency (enough insulin to suppress ketogenesis)" ↓ Box: "↑ Hepatic glucose output + ↓ Peripheral glucose utilization" ↓ Box: "SEVERE HYPERGLYCEMIA (>600 mg/dL)" ↓ Box: "Massive Osmotic Diuresis" ↓ Box: "Severe Dehydration (8–10 L deficit) — Patient CANNOT drink enough (elderly/debilitated)" ↓ Box: "Hemoconcentration + ↓ Renal glucose excretion → Worsening hyperglycemia" ↓ Final box (bold blue border): "HHS: Severe Hyperglycemia + Hyperosmolality (>320 mOsm/L) + NO Ketoacidosis" At the very bottom center, a simple 2-column comparison box: "KEY DIFFERENCE DKA → Absolute insulin lack → Ketosis + Acidosis HHS → Relative insulin lack → No ketosis, profound dehydration" White background, rounded corners on boxes, clear bold arrows, color coded orange-red for DKA and blue for HHS, clean minimal medical infographic style.
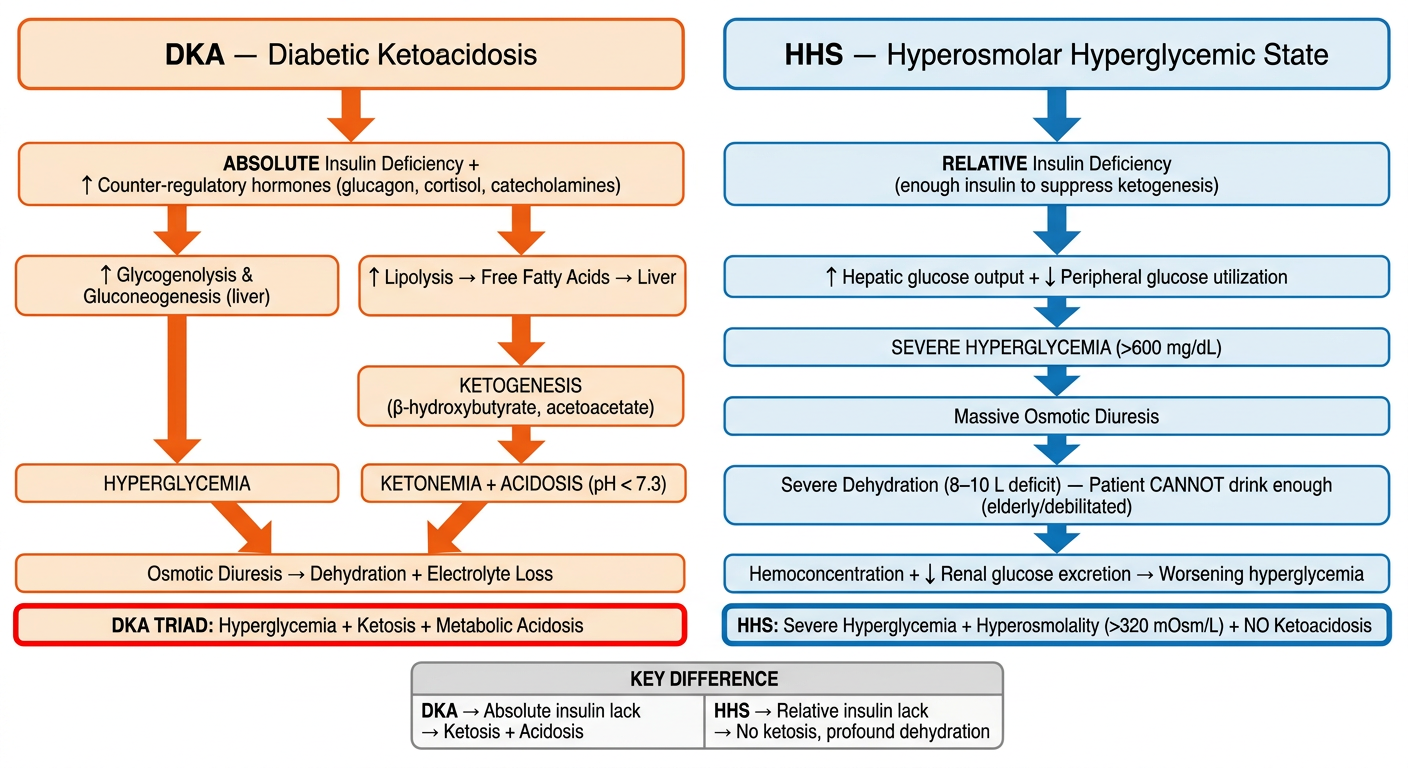
- Glucose axis: liver overproduces glucose → hyperglycemia
- Ketone axis: lipolysis → FFAs → liver ketogenesis → ketonemia → acidosis
- Both cause osmotic diuresis → dehydration
| DKA | HHS | |
|---|---|---|
| Insulin deficiency | Absolute | Relative |
| Ketosis | Yes (+++)" | No/trace |
| Acidosis | Yes (pH <7.3) | No |
| Glucose | >250 mg/dL | >600 mg/dL |
| Osmolality | Mildly ↑ | >320 mOsm/L |
Precipitating factors of dka and hss
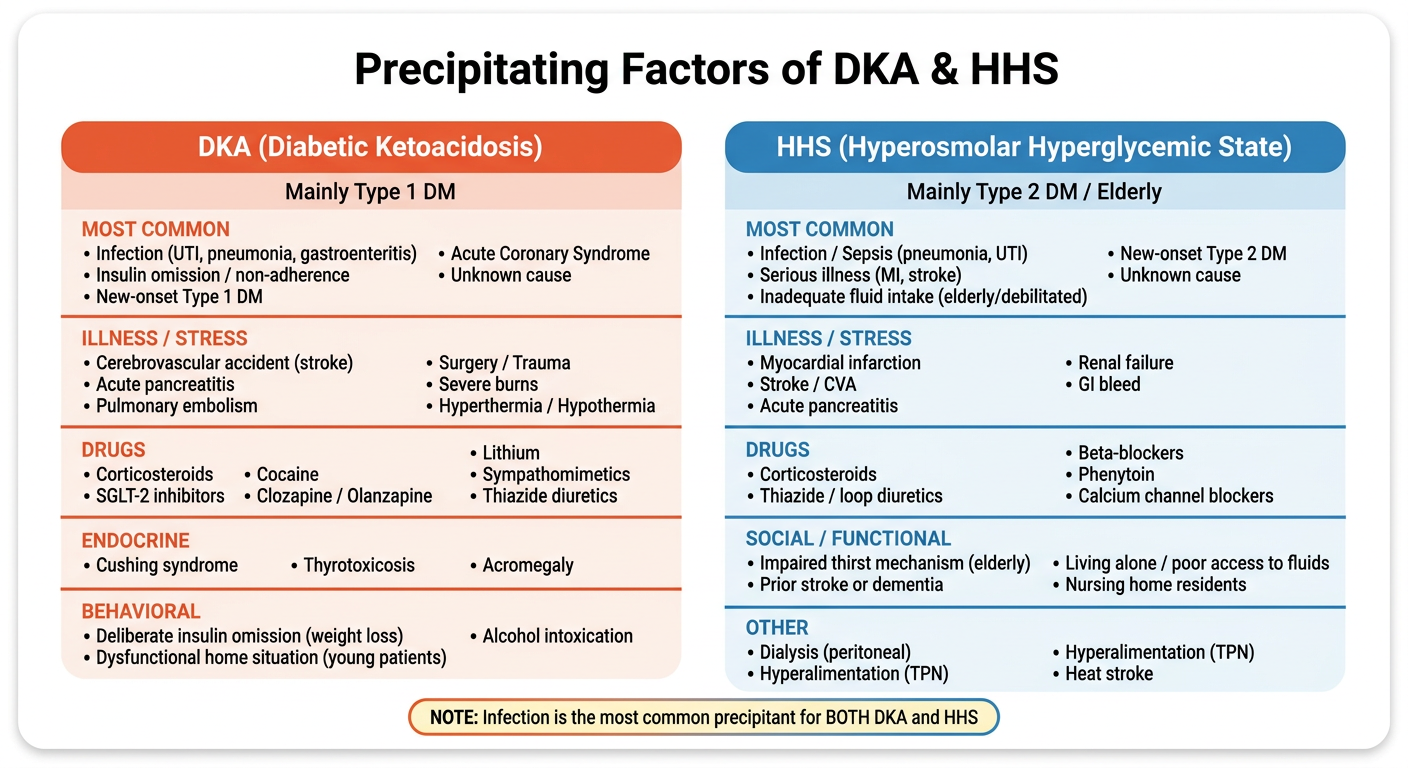
A clean, simple medical educational infographic/table showing precipitating factors of DKA and HHS side by side. White background, professional style, color coded. Title at top (bold, large): "Precipitating Factors of DKA & HHS" Two columns side by side: LEFT COLUMN - orange/red theme: Header: "DKA (Diabetic Ketoacidosis)" Subheader: "Mainly Type 1 DM" Section: "MOST COMMON" • Infection (UTI, pneumonia, gastroenteritis) • Insulin omission / non-adherence • New-onset Type 1 DM • Acute Coronary Syndrome • Unknown cause Section: "ILLNESS / STRESS" • Cerebrovascular accident (stroke) • Acute pancreatitis • Pulmonary embolism • Mesenteric thrombosis • Surgery / Trauma • Severe burns • Hyperthermia / Hypothermia Section: "DRUGS" • Corticosteroids • SGLT-2 inhibitors • Cocaine • Clozapine / Olanzapine • Lithium • Sympathomimetics • Thiazide diuretics Section: "ENDOCRINE" • Cushing syndrome • Thyrotoxicosis • Acromegaly Section: "BEHAVIORAL" • Deliberate insulin omission (weight loss) • Dysfunctional home situation (young patients) • Alcohol intoxication RIGHT COLUMN - blue theme: Header: "HHS (Hyperosmolar Hyperglycemic State)" Subheader: "Mainly Type 2 DM / Elderly" Section: "MOST COMMON" • Infection / Sepsis (pneumonia, UTI) • Serious illness (MI, stroke) • Inadequate fluid intake (elderly/debilitated) • New-onset Type 2 DM • Unknown cause Section: "ILLNESS / STRESS" • Myocardial infarction • Stroke / CVA • Acute pancreatitis • Renal failure • GI bleed Section: "DRUGS" • Corticosteroids • Thiazide / loop diuretics • Beta-blockers • Phenytoin • Calcium channel blockers Section: "SOCIAL / FUNCTIONAL" • Impaired thirst mechanism (elderly) • Prior stroke or dementia • Living alone / poor access to fluids • Nursing home residents Section: "OTHER" • Dialysis (peritoneal) • Hyperalimentation (TPN) • Heat stroke At the bottom center, a small highlighted note box: "NOTE: Infection is the most common precipitant for BOTH DKA and HHS" Use clear section dividers, bullet points, color-coded headers (orange-red for DKA, blue for HHS), clean white background, rounded corners, easy to read font.
Quick Reference
- I - Infection
- M - Medication (insulin missed / non-adherence)
- S - Stress (surgery, trauma, burns)
- I - Ischemia (MI, stroke)
- C - Cocaine / drugs (steroids, SGLT2i, clozapine)
- K - Ketosis-prone new-onset DM
| Factor | DKA | HHS |
|---|---|---|
| Infection | Most common | Most common |
| Insulin omission | Major cause | Less relevant |
| Impaired fluid intake | Less common | Key factor (elderly) |
| SGLT-2 inhibitors | Yes (euglycemic DKA) | No |
| Dementia / stroke hx | Rare | Common contributor |
| Deliberate behavior | Yes (young T1DM) | No |
Dka and hss clinical features
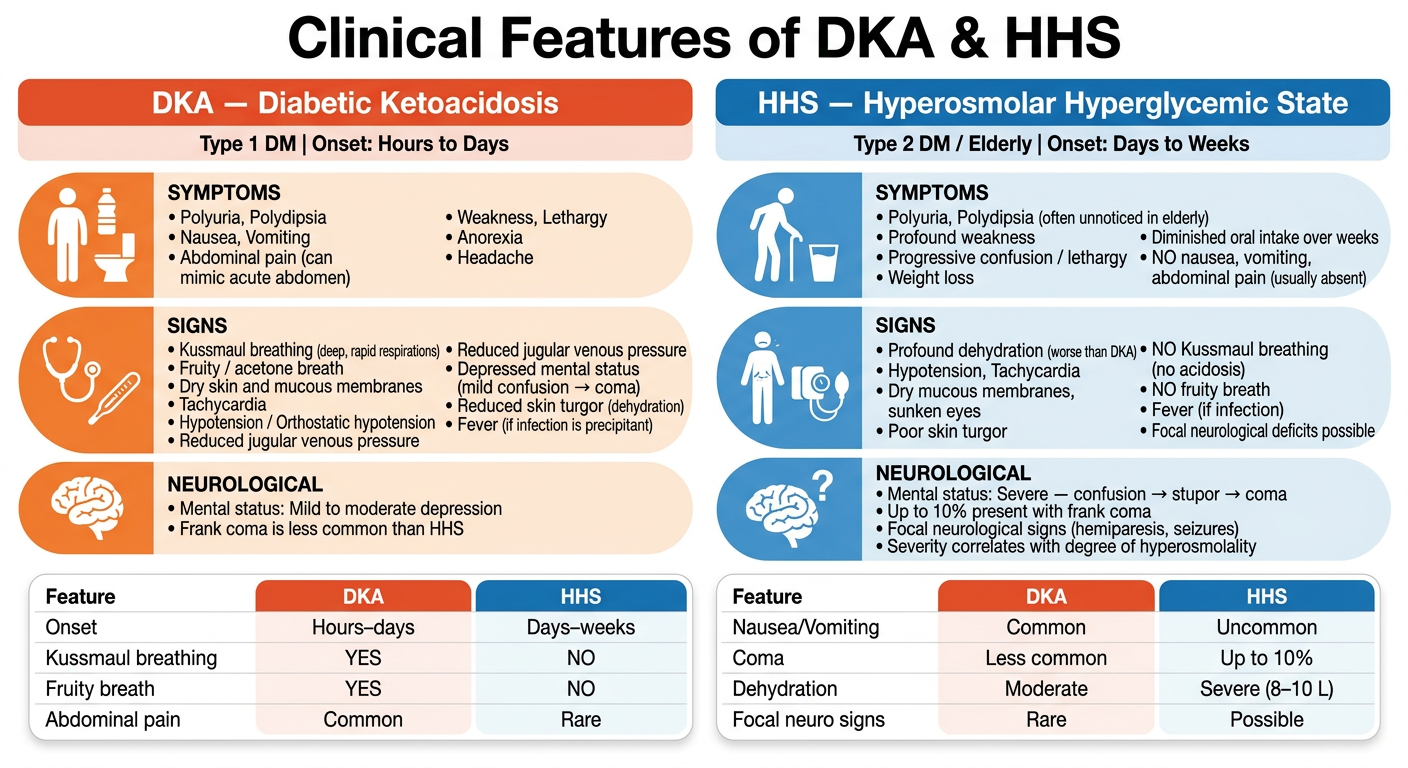
A clean, simple medical educational infographic showing clinical features of DKA and HHS side by side. White background, professional style, color coded, organized by system. Title at top (bold, large): "Clinical Features of DKA & HHS" Two main columns: LEFT COLUMN - orange/red theme: Header: "DKA — Diabetic Ketoacidosis" Subheader small text: "Type 1 DM | Onset: Hours to Days" SYMPTOMS section: • Polyuria, Polydipsia • Nausea, Vomiting • Abdominal pain (can mimic acute abdomen) • Weakness, Lethargy • Anorexia • Headache SIGNS section: • Kussmaul breathing (deep, rapid respirations) • Fruity / acetone breath • Dry skin and mucous membranes • Tachycardia • Hypotension / Orthostatic hypotension • Reduced jugular venous pressure • Depressed mental status (mild confusion → coma) • Reduced skin turgor (dehydration) • Fever (if infection is precipitant) NEUROLOGICAL section: • Mental status: Mild to moderate depression • Frank coma is less common than HHS RIGHT COLUMN - blue theme: Header: "HHS — Hyperosmolar Hyperglycemic State" Subheader small text: "Type 2 DM / Elderly | Onset: Days to Weeks" SYMPTOMS section: • Polyuria, Polydipsia (often unnoticed in elderly) • Profound weakness • Progressive confusion / lethargy • Weight loss • Diminished oral intake over weeks • NO nausea, vomiting, abdominal pain (usually absent) SIGNS section: • Profound dehydration (worse than DKA) • Hypotension, Tachycardia • Dry mucous membranes, sunken eyes • Poor skin turgor • NO Kussmaul breathing (no acidosis) • NO fruity breath • Fever (if infection) • Focal neurological deficits possible NEUROLOGICAL section: • Mental status: Severe — confusion → stupor → coma • Up to 10% present with frank coma • Focal neurological signs (hemiparesis, seizures) • Severity correlates with degree of hyperosmolality At the bottom: a comparison table with 2 columns: Feature | DKA | HHS Onset | Hours–days | Days–weeks Kussmaul breathing | YES | NO Fruity breath | YES | NO Abdominal pain | Common | Rare Nausea/Vomiting | Common | Uncommon Coma | Less common | Up to 10% Dehydration | Moderate | Severe (8–10 L) Focal neuro signs | Rare | Possible Use color-coded sections with icons if possible, orange-red for DKA, blue for HHS, clean readable font, rounded boxes, white background, bold section headings.
Key Clinical Distinguishers
- Kussmaul breathing - deep, rapid, sighing respirations (compensatory respiratory alkalosis for metabolic acidosis)
- Fruity/acetone breath - from exhaled acetone
- Abdominal pain + vomiting - common, can mimic surgical abdomen (caused by acidosis itself)
- Faster onset - hours to 1-2 days
- No Kussmaul, no fruity breath, no abdominal pain - absent because NO acidosis
- Profound dehydration - fluid deficit 8-10L vs 3-5L in DKA
- Worse CNS depression - up to 10% in frank coma, focal neuro deficits, seizures (because of severe hyperosmolality)
- Slower onset - days to weeks (often insidious in elderly)
Neurological Status Comparison
| CNS Finding | DKA | HHS |
|---|---|---|
| Mild confusion | Common | Common |
| Stupor | Less common | Common |
| Frank coma | Rare | Up to 10% |
| Focal deficits/seizures | Rare | Yes (hyperosmolality) |
The degree of CNS depression in HHS directly correlates with the severity of hyperosmolality - the higher the osmolality, the deeper the coma.