TKR SURGICAL STEPS AND CUTS
Reading File
Finding Sources
Searching the Web
total knee replacement surgical steps bone cuts technique
Finding Sources
Reading Web Page
https://www.ncbi.nlm.nih.gov/books/NBK499896
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
I now have comprehensive information from Campbell's Operative Orthopaedics (15th Ed 2026) and supplementary sources. Here is the full detailed answer:
Total Knee Replacement (TKR/TKA) - Surgical Steps and Bone Cuts
PATIENT POSITIONING & SETUP
- Supine with thigh support/tourniquet applied
- Knee flexed to ~90° for incision; leg hangs freely
- Tourniquet inflated after limb exsanguination (optional)
STEP 1 - SURGICAL APPROACH
Skin Incision
- Anterior midline longitudinal incision - the standard
- Made with the knee in flexion so subcutaneous tissue falls medially and laterally, improving exposure
- Incision must be long enough to avoid excessive skin tension (risk of skin necrosis)
- If prior scars exist, use the most lateral usable scar (blood supply comes predominantly from medial side)
Deep Approach (Retinacular Incision)
The medial parapatellar approach is most commonly used:
- Incise through a medial cuff of the quadriceps tendon (leave 3-4 mm cuff on vastus medialis for closure)
- Continue around the medial border of the patella
- Extend 3-4 cm onto the anteromedial tibial surface along the medial patellar tendon border
- Subperiosteally elevate anteromedial capsule and deep MCL off the tibia to the posteromedial corner
- Extend and evert the patella (or sublux laterally if obese/stiff)
Alternatives: midvastus approach (splits vastus medialis obliquus muscle), subvastus approach (preserves quadriceps entirely - better patellar tracking, harder exposure).
STEP 2 - JOINT EXPOSURE AND SOFT TISSUE PREPARATION
- Flex knee to ~90°
- Remove the ACL and anterior horns of medial and lateral menisci
- Remove any osteophytes (especially posterior condylar osteophytes - they block flexion and tent posterior capsule causing flexion contracture)
- Posterior meniscal horns are removed after bone cuts
STEP 3 - BONE CUTS (MEASURED RESECTION TECHNIQUE)
The goal: appropriate component sizing, mechanical axis restoration, balanced flexion/extension gaps, optimal patellar tracking.
CUT 1: DISTAL FEMORAL CUT (Extension Gap Cut)
- Made using an intramedullary (IM) guide (entry point: ~1 cm anterior and medial to intercondylar notch)
- Cut angle: 5-7° of valgus relative to the femoral anatomic axis (= perpendicular to the mechanical axis)
- This angle is measured off a long-standing radiograph (angle between mechanical and anatomic femoral axes)
- Amount of resection = thickness of distal femoral component (typically ~9-10 mm)
- Establishes the extension gap
- Key rules:
- Avoid elevating the joint line >4 mm
- For PS (posterior-stabilized) implants: add 2 mm extra distally to compensate for PCL sacrifice
- If a flexion contracture exists: additional resection can help, but avoid over-resection
CUT 2: PROXIMAL TIBIAL CUT (Foundation Cut - Affects Both Gaps)
- The most important cut in TKA - it affects both the flexion and extension gap
- Made using intramedullary or extramedullary guide, cut perpendicular to the tibial mechanical axis (0° in the coronal plane)
- Posterior slope: most systems incorporate 3° into the polyethylene insert; cutting guide set accordingly
- Rotation: referenced to the medial 1/3 of the tibial tubercle proximally and slightly medial to the center of the ankle distally (cross-referenced with 2nd ray of the foot and tibial crest)
- Resection amount:
- Referenced off the less arthritic side: ~8-10 mm (equals implant thickness)
- Referenced off the more arthritic side: typically 2 mm or less
- Protect patellar tendon and collateral ligaments with retractors during this cut
Note: Tibial cut can be performed before or after distal femoral cuts (surgeon preference).
CUT 3: FEMORAL SIZING AND ROTATION ASSESSMENT
Before the 4-in-1 femoral cuts, the surgeon determines:
- Component size (AP measurement of femur)
- Rotation of femoral component - this defines the shape of the flexion gap
Rotation Reference Options:
| Reference | Method |
|---|---|
| Transepicondylar axis (TEA) | Posterior femoral cut parallel to a line between medial and lateral epicondyles |
| Anteroposterior (Whiteside's) axis | Posterior cut perpendicular to line from sulcus to top of intercondylar notch |
| Posterior condylar axis | Cut in 3° external rotation off a line between posterior condyles |
| Cut tibial surface (gap balancing) | Rectangular gap with ligaments tensioned - femoral rotation follows the tibia |
- Internal rotation of femoral component causes lateral patellar tilt or patellofemoral instability
- Excessive external rotation widens the medial flexion gap causing flexion instability
CUT 4: 4-IN-1 FEMORAL CUTS (Flexion Gap + Finishing Cuts)
These cuts are made with a single cutting guide (the 4-in-1 jig) pinned to the distal femur:
| Cut | Purpose |
|---|---|
| Anterior femoral cut | Removes anterior cortex; avoids notching (use anterior referencing for safety) |
| Posterior femoral cuts (x2) | Remove posterior condyles ~9 mm; defines flexion gap size |
| Anterior chamfer cut | Bevels the anterior-to-distal femur junction |
| Posterior chamfer cut | Bevels the posterior-to-distal femur junction |
- Posterior referencing: jig feet sit flush on posterior condyles; removes fixed 9 mm posteriorly regardless of component size; smaller jigs remove more anteriorly
- Anterior referencing: boom sits on anterior cortex; consistent anterior cut depth; prevents notching/overstuffing
After these cuts, assess the flexion gap - it should equal the extension gap (symmetric rectangle). A rectangular flexion gap = correct rotation.
CUT 5: INTERCONDYLAR NOTCH CUT (PS implants only)
- Performed perpendicular to the transepicondylar axis
- Removes bone from the intercondylar box to accommodate the post-and-cam mechanism of a posterior-stabilized implant
- CR (cruciate-retaining) implants skip this cut
CUT 6: PATELLAR CUT
- Standard patellar button thickness = 9 mm
- Measure native patella thickness; resect to leave enough bone
- Example: 20 mm patella → set guide to 11-12 mm resection (some surgeons use 14 mm to protect against thin patella)
- Maintain symmetric thickness to avoid patellar tilt
- Not universally performed - patellar resurfacing is standard in the USA but not in many other countries
STEP 4 - GAP BALANCING AND SOFT TISSUE RELEASES
After bone cuts are made:
- Insert spacer blocks or a tensioning device in both flexion (90°) and extension (0°) gaps
- Gaps should be:
- Symmetric (equal medially and laterally)
- Equal in flexion and extension
- If extension gap tight medially: release posterior oblique ligament, semimembranosus, posteromedial capsule
- If flexion gap tight medially: release anterior superficial MCL, pes anserinus insertion
- If PCL is too tight (flexion gap tight): recess or release PCL; if PCL no longer functions - convert to PS implant
STEP 5 - TRIAL REDUCTION
- Impact femoral and tibial trial implants
- Insert provisional polyethylene spacer trial
- Reduce the knee and assess:
- Stability in full extension
- Mid-flexion stability
- Patellar tracking ("no thumb" test)
- Range of motion
- Final sizing and rotational alignment confirmed
STEP 6 - COMPONENT IMPLANTATION
- Thorough irrigation and debridement
- Cement tibial baseplate (and/or femoral component) - depending on system (cemented vs cementless)
- Impact femoral component
- Insert final polyethylene insert
- Cement or press-fit patella button
- Confirm final ROM, stability, patellar tracking
STEP 7 - CLOSURE
- Thorough irrigation
- Close retinacular layer (medial parapatellar cuff) with interrupted sutures
- Subcutaneous layer closed
- Skin closure (staples or suture)
- Drain placement (optional)
SUMMARY: ORDER OF BONE CUTS
1. Distal Femoral Cut → sets extension gap (5-7° valgus IM guide)
2. Proximal Tibial Cut → foundation cut (perpendicular to mech. axis)
3. Size & Rotate Femur → determine AP size + rotation reference
4. Anterior Femoral Cut → 4-in-1 jig
5. Posterior Femoral Cuts → 4-in-1 jig (9 mm posteriorly)
6. Anterior Chamfer Cut → 4-in-1 jig
7. Posterior Chamfer Cut → 4-in-1 jig
8. Box Cut (PS only) → intercondylar notch
9. Patellar Cut → 9 mm button resurfacing
ALIGNMENT GOALS
| Parameter | Target |
|---|---|
| Mechanical axis | 0° (neutral) ± 3° |
| Tibial cut angle | 0° (perpendicular to mech. axis) |
| Distal femoral cut | 5-7° valgus (anatomic axis) |
| Femoral component rotation | 0-3° external rotation |
| Posterior tibial slope | 0-3° (implant-dependent) |
| Tibial resection | 8-10 mm (less arthritic side) |
| Distal femoral resection | = component thickness (~9-10 mm) |
| Joint line elevation (max) | ≤ 4 mm (primary); ≤ 8 mm total |
Sources: Campbell's Operative Orthopaedics 15th Ed 2026, Miller's Review of Orthopaedics 9th Ed, StatPearls TKA Techniques (NCBI)
Pain shock
Reading File
Finding Sources
Finding Sources
Searching the Web
pain shock neurogenic vasovagal pathophysiology mechanism clinical features management
Reading File
Reading File
Reading File
Reading File
Reading File
Now I have comprehensive textbook content. Here is the full answer:
Pain Shock (Primary / Neurogenic Shock)
Definition
Pain shock (also called primary shock, neurogenic shock, or vagal inhibition) is a sudden circulatory collapse triggered by an overwhelming neural stimulus - most commonly pain, fear, emotional stress, or stimulation of a sensitive reflex area - that causes acute peripheral vasodilatation and/or cardiac inhibition, resulting in inadequate tissue perfusion.
It is classified as a form of distributive (neurogenic) shock - the underlying problem is not a loss of blood volume but a loss of vasomotor tone, leading to pathological pooling of blood in the periphery.
- P.C. Dikshit Textbook of Forensic Medicine and Toxicology
- Parikh's Textbook of Medical Jurisprudence, Forensic Medicine and Toxicology
Two Overlapping Mechanisms
1. Sympathetico-adrenal stimulation pathway (Classic "Pain Shock")
Severe pain triggers massive sympathetic discharge:
- Sudden pooling of blood in splanchnic and peripheral vascular beds (neurogenic vasodilation)
- Reduced venous return to the heart
- Fall in cardiac output and blood pressure
- In extreme cases: sudden rise in BP can rupture a Berry aneurysm or dissecting aortic aneurysm
2. Vagal inhibition pathway (Vasovagal / Reflex)
Stimulation of trigger areas (epigastrium, throat, genitals, etc.) activates the inhibitory vagus nerve:
- Sudden reflex cardiac slowing or arrest
- Paralysis of cardiac and respiratory centres
- Instantaneous collapse - can cause sudden death
"Holding the throat in an excited person may result in his collapse and instantaneous death. Other examples are: a blow on the epigastrium, sudden joy, fear, pain." - Parikh's
Pathophysiology
Pain / Emotional Stimulus / Blow on Receptor Area
↓
Afferent nerve impulse to CNS
↓
┌───────────────────────────────────────────┐
│ Sympathetic pathway Vagal pathway │
│ (adrenal stimulation) (inhibitory vagus)│
└───────────────────────────────────────────┘
↓ ↓
Peripheral vasodilation Bradycardia / Cardiac arrest
(splanchnic pooling)
↓
Decreased venous return → ↓ Cardiac Output → ↓ BP
↓
Tissue Hypoperfusion (SHOCK)
Key physiological changes (Guyton & Hall Medical Physiology):
- Loss of vasomotor tone - vasomotor center depressed or overridden
- Increased vascular capacitance → decreased venous return
- Decreased cardiac output
- Brain ischemia from hypoperfusion → further vasomotor center depression (vicious cycle)
Trigger Zones / Receptor Areas
These are areas with dense afferent nerve endings capable of triggering reflex vagal inhibition:
| Area | Example Trigger |
|---|---|
| Epigastrium | Blow to the solar plexus |
| Throat / neck | Pressure on carotid sinus or larynx |
| Genitals / perineum | Trauma, instrumentation |
| Testicles | Squeeze injury |
| Eye | Ocular manipulation (oculocardiac reflex) |
| Chest | Blunt trauma |
| Any body surface | Sudden intense pain from any cause |
Clinical Features
| Feature | Description |
|---|---|
| Tremors and anxiety | Early stage |
| Pallor | Cutaneous vasoconstriction (or paradoxical flushing in pure neurogenic/spinal type) |
| Cold clammy extremities | Splanchnic pooling, reduced skin perfusion |
| Sighing respiration | Irregular, shallow breaths |
| Repeated yawning | Cerebral hypoxia |
| Dilated pupils | Sympathetic stimulation |
| Rapid pulse / bradycardia | Depends on dominant mechanism - vagal type gives bradycardia |
| Hypotension | Core feature |
| Loss of consciousness/syncope | If severe |
| Sudden death | In cases of pure vagal inhibition or in those with pre-existing cardiac disease |
Classic neurogenic shock (spinal-type): hypotension + bradycardia + warm flushed extremities (no reflex tachycardia due to disrupted sympathetic tone) - Schwartz's Principles of Surgery
Key Distinction: Primary vs Secondary Shock
| Feature | Primary (Neurogenic/Pain) Shock | Secondary (Haematogenic) Shock |
|---|---|---|
| Onset | Immediate - within seconds/minutes | Delayed - hours after injury |
| Mechanism | Neurogenic vasodilation / vagal inhibition | True volume depletion (blood/fluid loss) |
| Trigger | Pain, fear, emotion, receptor area stimulation | Haemorrhage, burns, crush injury |
| Extremities | Initially cold/clammy (sympathetic) or warm (spinal) | Cold, clammy |
| Prognosis | Often self-limiting; can cause sudden death | More serious, progressive |
Forensic / Medicolegal Significance
Pain shock has major medicolegal importance because:
- A minor blow to a receptor area (e.g., epigastrium, throat) can cause sudden death with minimal or no external marks
- Autopsy findings may be negative - diagnosis by exclusion
- Must exclude: fatal wounds, poisoning, natural disease
- At-risk populations: emotionally labile individuals, elderly, those with existing cardiac disease, severely ill patients
Autopsy diagnosis criteria:
- History of sudden death from blow/injury over a receptor area
- Person of emotional temperament, elderly, or debilitated
- Exclusion of fatal injuries, poisoning, and natural disease
Management
Immediate Measures
- Remove the painful stimulus if possible
- Lay patient flat / supine - elevate legs (Trendelenburg position) to improve venous return
- Secure airway and ensure ventilation
- IV fluid resuscitation - first-line treatment; restores intravascular volume and preload
Pharmacological (if fluids insufficient)
| Drug | Role |
|---|---|
| Dopamine | First-line vasopressor if fluids fail |
| Phenylephrine (pure α-agonist) | For refractory hypotension; increases peripheral vascular tone |
| Atropine | If bradycardia is predominant (vagal inhibition) |
| Epinephrine | For severe anaphylaxis-component or cardiac arrest |
Monitoring
- ICU-level monitoring for haemodynamics and cardiac function
- Vasopressor support typically lasts only 24-48 hours as neurogenic shock tends to resolve
- In spinal cord injury cases: monitor for pulmonary oedema (loss of vasomotor capacity in pulmonary circulation)
- Must exclude haemorrhage in all trauma patients before attributing hypotension to neurogenic causes
Classification of Shock (Summary Table)
| Type | Example | Mechanism |
|---|---|---|
| Cardiogenic | MI, tamponade, arrhythmia | Pump failure |
| Hypovolaemic/Haemorrhagic | Massive blood loss, burns | Inadequate circulating volume |
| Septic | Gram-negative bacteraemia | Peripheral vasodilation + cell injury |
| Primary/Neurogenic (Pain Shock) | Pain, fear, spinal cord injury, anaesthesia | Peripheral vasodilation (sympathetic/parasympathetic) |
| Anaphylactic | Antigen-antibody reaction | Histamine-mediated vasodilation + increased capillary permeability |
Sources: P.C. Dikshit Textbook of Forensic Medicine & Toxicology; Parikh's Textbook of Medical Jurisprudence; Schwartz's Principles of Surgery 11e; Mulholland & Greenfield's Surgery 7e; Guyton & Hall Medical Physiology; Tintinalli's Emergency Medicine
Trigger finger
Reading File
Finding Sources
Finding Sources
Searching the Web
trigger finger stenosing tenosynovitis grading classification treatment surgery
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
I now have comprehensive information from multiple authoritative textbooks. Here is the complete answer:
Trigger Finger (Stenosing Tenosynovitis)
Definition
Trigger finger is a stenosing tenosynovitis of the flexor tendon at the level of the A1 pulley (first annular pulley), causing painful catching, snapping, or locking of the digit during flexion and extension. It is one of the most common hand conditions encountered in orthopedic and rheumatology practice.
Anatomy & Pathophysiology
The flexor tendons of each finger pass through a series of fibro-osseous tunnels formed by annular (A) and cruciate (C) pulleys:
A1 → A2 → C1 → A3 → C2 → A4 → C3 → A5
- The A1 pulley sits at the level of the metacarpophalangeal (MCP) joint in the distal palm
- In trigger finger, the A1 pulley undergoes fibrosis, thickening, and narrowing
- Histology shows fibrocartilaginous metaplasia of the pulley and/or flexor digitorum superficialis (FDS) tendon
- The flexor tendon (usually with a fusiform swelling or nodule) catches on the constricted pulley
- The tendon nodule is typically located just proximal to the annulus at the MCP level
- The nodule moves with the tendon and can be palpated by the examiner
- In rheumatoid arthritis, a nodule may be distal to this point
Epidemiology
| Feature | Detail |
|---|---|
| Lifetime prevalence | ~2-3% in adults |
| Most common digit | Thumb (most common), then ring and long fingers |
| Sex ratio | Triggering of thumb is 4x more frequent in women than men |
| Age | Most common in individuals >45 years (primary type); middle age |
| Peak | Women older than 50 years of age |
| Common associations | Diabetes mellitus, rheumatoid arthritis (RA), gout, de Quervain's disease, carpal tunnel syndrome (CTS coexists in 40-60% of patients) |
| Repetitive activity | Possibly associated with repetitive grasping |
Types
| Type | Features |
|---|---|
| Primary (Idiopathic) | Most common; middle-aged individuals; single digit |
| Secondary | Associated with RA, diabetes, gout; often multiple digits, may coexist with other stenosing tendinopathies |
| Pediatric / Developmental | Formerly called "congenital" - actually acquired; usually trigger thumb; presents with locked IP joint flexion in first few years of life |
Clinical Features
Early:
- Pain and tenderness over the A1 pulley in the distal palm
- Snapping or clicking during digital motion - typically worse on awakening
- Patient often reports the problem is in the PIP joint (referred pain)
Progressive:
- Frank catching or locking in flexion
- Digit locks and requires passive extension with the other hand
- Reduced range of motion
Late:
- Fixed flexion contracture of the PIP joint
- Cannot be actively or passively corrected
Green's Classification (Froimson Grading)
| Grade | Description |
|---|---|
| I | Pain and tenderness at the A1 pulley; history of catching but not demonstrable on exam (pre-triggering) |
| II | Catching of finger; demonstrable; patient can actively extend |
| III | Locking of finger; passively correctable (requires other hand to extend) |
| IV | Fixed, locked finger - flexion contracture of PIP joint; not passively correctable |
Surgical indication: Grade III-IV, or Grade II failing 3 months of conservative treatment.
Differential Diagnosis
- Intra-articular disorders (loose bodies, degenerative joint disease, fractures)
- Common extensor tendon subluxation at MCP
- Dupuytren's contracture
- De Quervain's tenosynovitis (coexisting)
- Ganglion/retinacular cyst over A1 pulley
Treatment
Conservative (Non-operative)
Indications: All grades initially; uncomplicated cases with short symptom duration
| Modality | Details |
|---|---|
| Rest & activity modification | Avoid repetitive grasping |
| Stretching | Passive digital extension stretching |
| Night splinting | MCP held in extension; prevents locking; most effective at night |
| Heat/Ice | Symptom relief |
| NSAIDs | Analgesia and inflammation reduction |
| Corticosteroid injection | 60% success rate after a single injection; ~"curative" in 60%; effective for most patients |
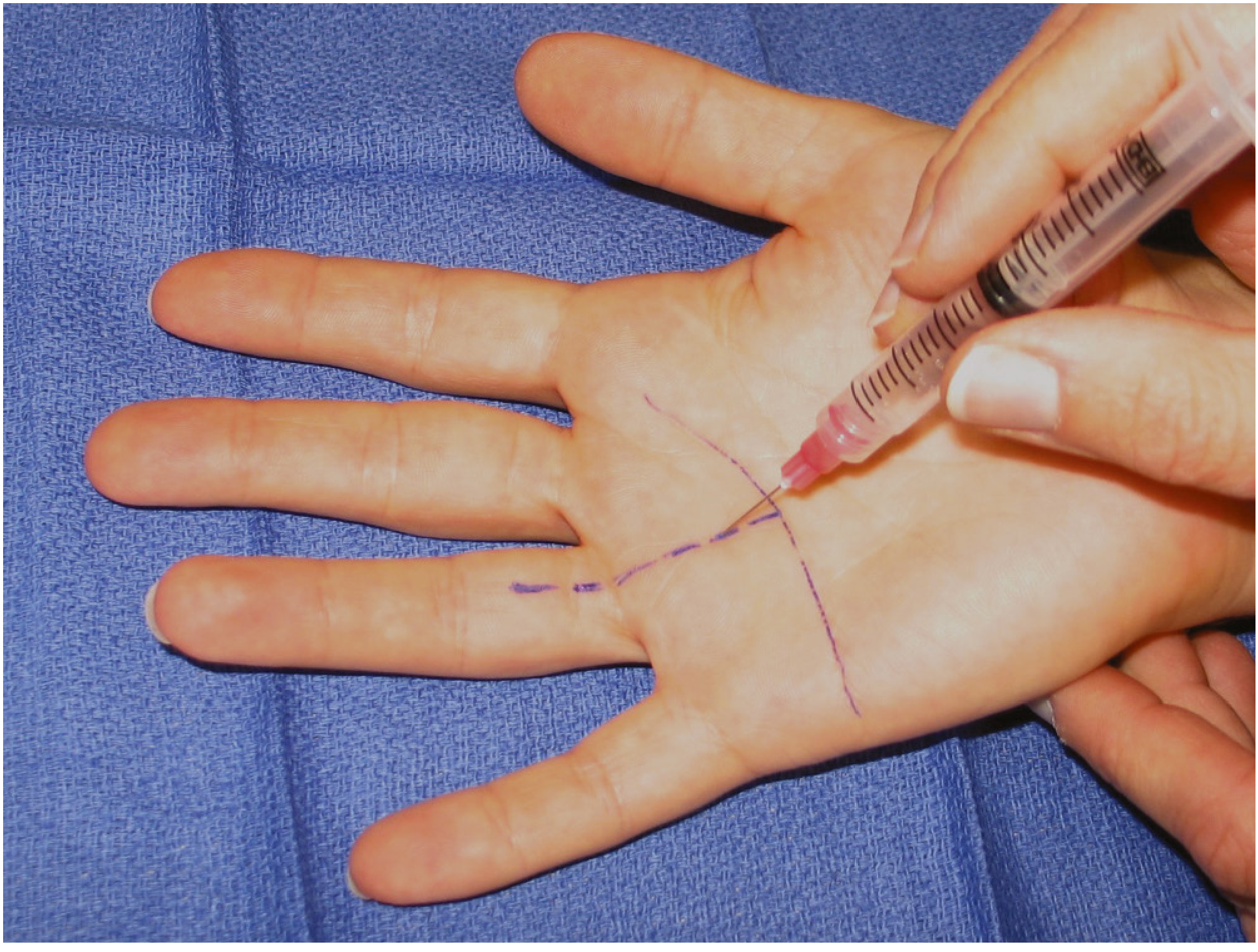
Corticosteroid Injection Technique
Injection into the flexor tendon sheath at the A1 pulley level:
- Needle enters at the distal palmar crease at 45-60° angle in the midline of the digit
- No difference between soluble and insoluble steroid preparations
- Repeat injections can be used, especially in patients preferring non-operative management
- Short course of splinting after injection may improve longevity
Special notes on diabetic patients:
- More refractory to non-operative management
- Corticosteroid injections may elevate serum glucose for ≥5 days
- Patients with unstable diabetes may be better treated without injection
- Cost-analysis shows immediate surgical release is the most cost-effective strategy in diabetic patients
Surgical Treatment
Indications:
- Failure of conservative management (including steroid injection)
- Grade III-IV disease
- Fixed contracture (Grade IV)
- Patient preference for definitive treatment
- Diabetic patients (cost-effective first-line)
- RA patients (specific modifications required)
Option 1: Open Surgical Release (Gold Standard - ~97% success rate)
Technique (Campbell's Operative Orthopaedics 15th Ed 2026):
- Anaesthesia: Local anaesthetic infiltration proximal to incision site; tourniquet (pneumatic or forearm Esmarch wrap) or epinephrine in local anaesthetic without tourniquet
- Incision:
- Transverse incision ~2 cm, placed:
- Middle, ring, small fingers: Several mm distal to the distal palmar crease
- Index finger: Several mm distal to the proximal palmar crease
- Thumb: Distal or proximal to the MCP joint flexion crease
- Alternative: oblique or longitudinal incision between MCP and distal palmar crease
- Transverse incision ~2 cm, placed:
- Nerve protection: Digital nerves are identified and protected. The thumb radial digital nerve is especially vulnerable (more palmar and closer to the flexor sheath than expected)
- Exposure: Spread subcutaneous tissues to expose the annular pulley system; confirm digital nerves are safe
- Pulley division:
- Open the pulley with a No. 15 blade and tenotomy scissors
- Fingers: Divide A1 and A0 (proximal palmar) pulley
- Thumb: Divide only the A1 pulley; avoid cutting too far distally (preserve oblique pulley)
- Incise from proximal to distal
- Confirm release: With a local block, ask the patient to flex and extend the finger and confirm cessation of triggering intraoperatively
- Closure and light dressing
Postoperative care: Active hand and finger use encouraged immediately; stretching exercises
Note: Triggering after release may occur due to catching on palmar aponeurosis transverse fibers - usually resolves with time. Occasionally a partially lacerated flexor tendon heals with a nodule causing triggering.
Option 2: Percutaneous Release
Technique:
- Inject local anaesthetic into palmar skin proximal to the release site
- Use an 18- or 19-gauge needle (ultrasound guidance optional)
- Position: palm up, hand on folded towel, MCP joint in slight hyperextension
- Insert needle onto A1 pulley; orient bevel longitudinally parallel to flexor tendons
- Move needle proximally and distally along the pulley, pressing firmly - feel for scraping/grating sensation as sheath is incised
- When grating is eliminated, remove needle and test finger flexion/extension
- Optional: inject corticosteroid at end
- Adhesive bandage; encourage immediate active use
Limitations of percutaneous release:
- Risk of incomplete pulley release
- Damage to flexor tendons and digital nerves
- Especially concerning for index finger and thumb (digital nerve anatomy)
Special Situations
Rheumatoid Arthritis patients:
- Preference is to excise a slip of the FDS tendon rather than release the A1 pulley
- RA patients are at risk for ulnar drift at the MCP joint - A1 pulley release can exacerbate this drift
Recurrent triggering after A1 release:
- If triggering persists: resection of the ulnar FDS slip when necessary
Pediatric Trigger Finger vs. Trigger Thumb
| Feature | Trigger Finger (Pediatric) | Trigger Thumb (Pediatric) |
|---|---|---|
| Frequency | Rare (2.3%) | 10x more common than trigger finger |
| Pathology | Abnormalities up to A3 pulley; FDS/FDP tendon nodularities; abnormal decussation | Notta's node - pathologic nodular FPL tendon thickening |
| Presentation | Snapping at PIP; fixed flexion deformity | Fixed IP joint flexion in first few years of life; no snapping as main complaint |
| Conservative | Observation + extension splinting (67% resolve with splinting vs 30% observation only) | Observation initially |
| Surgery | A1 release + consider FDS slip resection (Bruner incision); 91% success | A1 pulley release at 2-4 years; radial digital nerve at risk |
The condition is developmental, not truly congenital - not noted until the patient is several years old.
Complications of Surgical Release
| Complication | Notes |
|---|---|
| Wound dehiscence | Minor but relatively common |
| Scar tenderness | Common |
| Decreased ROM | Especially with stiffness |
| Digital nerve injury | Radial digital nerve of thumb especially vulnerable |
| Incomplete release / persistence | More common than true recurrence |
| Bowstringing | If too many pulleys released |
| Infection | Risk increased with preoperative hypoglycemia in diabetics |
Key Points Summary
- Trigger finger = A1 pulley stenosis causing flexor tendon catching/locking
- Most common in thumb > ring > long finger; women >45 years
- Histology: fibrocartilaginous metaplasia of pulley/tendon
- Graded I-IV by Green's (Froimson) classification
- 60% respond to a single corticosteroid injection
- 97% success with open A1 pulley release
- Diabetics: more refractory to injection; early surgery preferred
- RA: FDS slip resection preferred over A1 release (prevents ulnar drift)
- Always protect the radial digital nerve of the thumb during release
Sources: Campbell's Operative Orthopaedics 15th Ed 2026; Miller's Review of Orthopaedics 9th Ed; Firestein & Kelley's Textbook of Rheumatology; Gray's Anatomy for Students; Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.