Blood tests for infertility
Reading File
Finding Sources
Finding Sources
Searching PubMed
"infertility" AND "laboratory evaluation"
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive overview of blood tests used in the workup of infertility, organized by sex. The evaluation begins with history and physical examination of both partners, then proceeds to targeted laboratory investigations.
Definition
Infertility is the inability to conceive after 12 months of regular unprotected intercourse (or 6 months in women ≥35 years). A specific cause is found in ~80% of couples: one-third due to female factors alone, one-third male factors alone, and one-third a combination. — Tietz Textbook of Laboratory Medicine, 7th Ed.
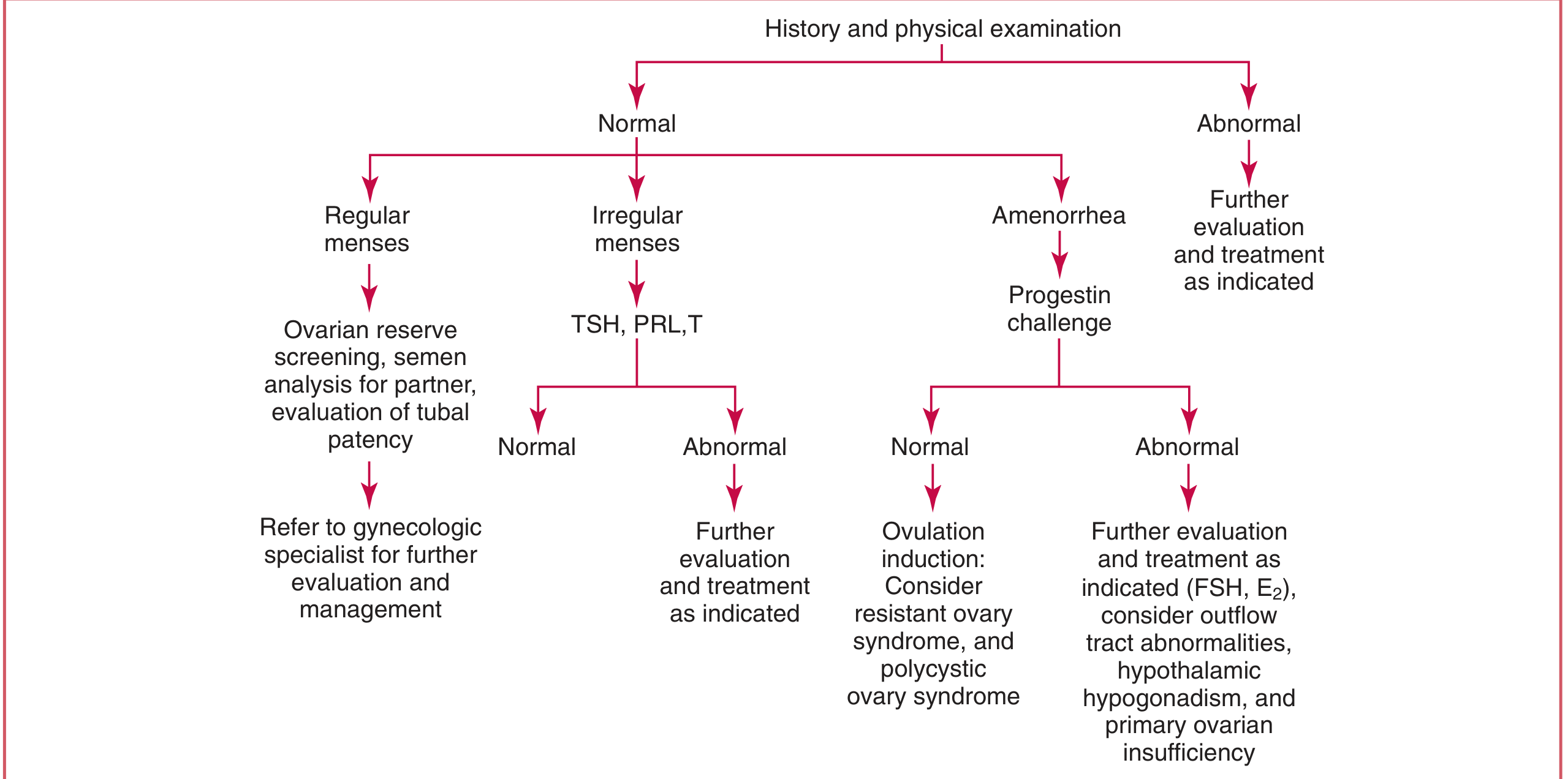
Female Infertility — Blood Tests
Algorithm for evaluation:
1. Ovulation Assessment
| Test | Timing | Interpretation |
|---|---|---|
| Serum Progesterone | Midluteal (day 21–23) | >300 ng/dL (9.5 nmol/L) confirms corpus luteum formation (indirect evidence of ovulation) |
| LH surge (urine/serum) | Periovulatory | LH peaks 24–36 hours before ovulation; used to time intercourse |
2. Ovarian Reserve Testing
Used when diminished ovarian reserve is suspected (advanced age, prior ovarian surgery, poor response to stimulation):
| Test | Interpretation |
|---|---|
| FSH (day 2–3 of cycle) | Elevated FSH indicates reduced reserve; FSH >10–15 IU/L is concerning |
| Estradiol (E₂) (day 2–3) | Elevated early-cycle E₂ (>60–80 pg/mL) suggests poor reserve even if FSH is normal |
| Anti-Müllerian hormone (AMH) | Low AMH indicates diminished ovarian reserve; relatively cycle-independent |
3. Tests for Irregular or Absent Cycles
When menses are irregular or absent, measure:
| Test | Why |
|---|---|
| TSH | Hypothyroidism/hyperthyroidism impairs ovulation |
| Prolactin (PRL) | Hyperprolactinemia suppresses GnRH → anovulation |
| Testosterone (T) | Elevated in PCOS, adrenal disorders, androgen-secreting tumors |
| FSH + LH | Low FSH/LH = hypothalamic/pituitary failure; High FSH = primary ovarian insufficiency |
| Estradiol | Low in hypothalamic amenorrhea or primary ovarian insufficiency |
4. Additional Hormonal Tests (When Indicated)
| Test | Indication |
|---|---|
| hCG (β-hCG) | Rule out pregnancy before evaluation |
| DHEA-S / 17-OH Progesterone | Suspected congenital adrenal hyperplasia or adrenal androgen excess |
| Fasting glucose / insulin / HOMA-IR | PCOS-related insulin resistance |
| Karyotype / genetic testing | Suspected Turner syndrome or premature ovarian insufficiency |
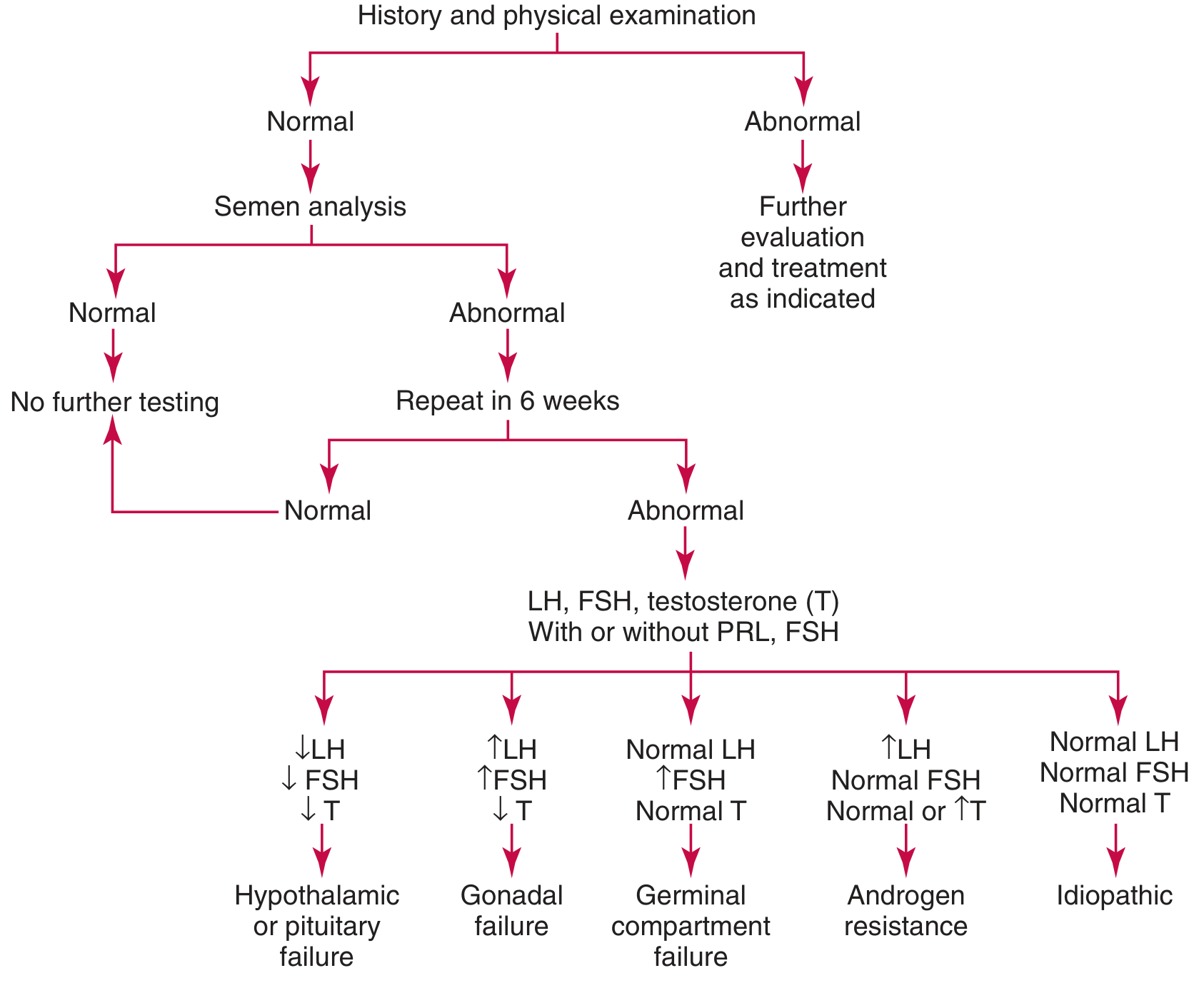
Male Infertility — Blood Tests
The primary test in male infertility is semen analysis (not a blood test), but if semen analysis is persistently abnormal, hormonal blood tests follow:
Algorithm:
Core Hormonal Panel
| Test | Interpretation |
|---|---|
| Total Testosterone | Measured first; low T (<200 ng/dL, 7 nmol/L) triggers further workup |
| Free Testosterone | Checked when total T is borderline (SHBG confounders) |
| FSH | ↑FSH + low sperm count = Sertoli cell/germinal epithelium failure (e.g., Klinefelter syndrome, radiation) |
| LH | Evaluated alongside FSH to localize the defect |
| Prolactin | Measured if T and FSH are abnormal; hyperprolactinemia suppresses GnRH |
Pattern Interpretation
| Hormone Pattern | Diagnosis |
|---|---|
| ↓LH, ↓FSH, ↓T | Hypothalamic or pituitary failure (e.g., Kallmann syndrome) |
| ↑LH, ↑FSH, ↓T | Gonadal (testicular) failure — primary hypogonadism |
| Normal LH, ↑FSH, Normal T | Germinal compartment failure (isolated spermatogenic defect) |
| ↑LH, Normal FSH, Normal or ↑T | Androgen resistance |
| All normal | Idiopathic or obstructive azoospermia |
Stimulation Tests (Specialized)
- hCG stimulation test: Testosterone measured before and 72 hours after 5,000 IU hCG IM. Doubling of testosterone = normal Leydig cell function; failure to rise >150 ng/dL = primary hypogonadism.
- GnRH stimulation test: Used to distinguish pituitary from hypothalamic failure. FSH/LH measured at 0, 30, 60, 120, 180 min after 100 µg IV GnRH. Rise ≥10 IU/L = normal pituitary; no rise = pituitary disease; delayed rise = hypothalamic disease.
Genetic Blood Tests
| Test | Indication |
|---|---|
| Karyotype | Suspected Klinefelter syndrome (47,XXY) in azoospermia with ↑FSH |
| Y-chromosome microdeletion (FISH/PCR) | Azoospermia or severe oligospermia |
| CFTR gene mutation | Congenital bilateral absence of vas deferens |
Summary Table — Key Blood Tests at a Glance
| Test | Female | Male |
|---|---|---|
| FSH | Ovarian reserve; ovulatory axis | Spermatogenic failure |
| LH | Ovulation timing; axis localization | Axis localization |
| Estradiol (E₂) | Ovarian reserve, follicular status | — |
| Progesterone | Confirms ovulation (midluteal) | — |
| Testosterone | PCOS, androgen excess | Hypogonadism, axis evaluation |
| Prolactin | Hyperprolactinemia → anovulation | Hyperprolactinemia → low T |
| TSH | Thyroid-related anovulation | Thyroid-related dysfunction |
| AMH | Ovarian reserve | — |
| β-hCG | Rule out pregnancy | — |
| Karyotype | Turner syndrome, POI | Klinefelter syndrome |
Sources: Tietz Textbook of Laboratory Medicine, 7th Ed., Ch. 58; Goldman-Cecil Medicine, Ch. 218; Henry's Clinical Diagnosis and Management by Laboratory Methods
Pre maraital blood test list
Finding Sources
Searching the Web
premarital blood tests complete list recommended screening
Finding Sources
Finding Sources
Here is a comprehensive premarital blood test list, organized by category:
Premarital Blood Test Panel
1. Blood Group & Compatibility
| Test | Purpose |
|---|---|
| ABO Blood Group | Identify blood type (A, B, AB, O) |
| Rh Factor (Rh typing) | Critical if female is Rh-negative — risk of hemolytic disease of the newborn in future pregnancies |
2. Genetic / Haematological Screening
| Test | Purpose |
|---|---|
| Haemoglobin Electrophoresis (Hb electrophoresis) | Detects sickle cell trait/disease (HbS), thalassaemia trait (α or β), and other haemoglobinopathies |
| Complete Blood Count (CBC) | Screens for anaemia, thrombocytopenia; low MCV raises suspicion of thalassaemia trait |
| Sickle Cell Genotype (HbAA, HbAS, HbSS, HbSC) | Especially critical — two carriers (AS × AS) have a 1-in-4 chance of an HbSS child |
| G6PD Screening | Enzyme deficiency common in certain populations; affects drug and food choices |
Two carriers of the same recessive disorder should receive genetic counselling before marriage. — Tietz Textbook of Laboratory Medicine, 7th Ed.
3. Infectious Disease Screening
| Test | Purpose |
|---|---|
| HIV 1 & 2 (ELISA / 4th-generation combo) | Prevent transmission to partner and future children |
| Hepatitis B Surface Antigen (HBsAg) | Identifies active/carrier HBV infection; vaccination can protect unvaccinated partner |
| Hepatitis B Surface Antibody (Anti-HBs) | Confirms immunity from vaccination or prior infection |
| Hepatitis C Antibody (Anti-HCV) | Chronic HCV can be silent for years |
| VDRL / RPR (Syphilis) | Syphilis can be asymptomatic and causes serious complications in pregnancy |
| Treponemal antibody (TPHA/FTA-ABS) | Confirmatory test for syphilis if VDRL is reactive |
4. Hormonal & Reproductive Health
| Test | Purpose |
|---|---|
| TSH (Thyroid Stimulating Hormone) | Undiagnosed thyroid disease affects fertility and fetal development |
| Fasting Blood Glucose / HbA1c | Screen for diabetes mellitus, which impacts pregnancy outcomes |
| Prolactin | Hyperprolactinemia can cause fertility issues in both sexes |
5. Rubella & Other Infections (Women)
| Test | Purpose |
|---|---|
| Rubella IgG (Rubella immunity) | If non-immune, vaccinate before pregnancy — rubella in first trimester causes congenital rubella syndrome |
| Toxoplasma IgG/IgM | Baseline serology; acute infection in pregnancy can harm the fetus |
| TORCH screen (optional, if indicated) | Toxoplasma, Rubella, CMV, Herpes — baseline status before pregnancy |
6. Additional Tests (Based on Region/Risk)
| Test | Purpose |
|---|---|
| Malaria (blood film or RDT) | Relevant in endemic regions |
| Urinalysis | Screen for renal disease, UTI, glucose |
| Karyotyping | If there is a family history of chromosomal disorders or recurrent miscarriages |
| Cystic Fibrosis carrier screen | Relevant in Caucasian and certain other populations |
| Spinal Muscular Atrophy (SMA) screen | Offered in some comprehensive premarital panels |
| Fragile X permutation screening | If family history of intellectual disability or premature ovarian insufficiency |
Quick Reference Summary
| Category | Key Tests |
|---|---|
| Blood group | ABO + Rh factor |
| Genetic | Hb electrophoresis, CBC, sickle cell genotype, G6PD |
| Infections | HIV, HBsAg, Anti-HCV, VDRL/RPR |
| Reproductive | TSH, fasting glucose, prolactin |
| Immunity (female) | Rubella IgG, Toxoplasma |
Practical Notes
- Sickle cell and thalassaemia screening are the most clinically important genetic tests for populations of African, Middle Eastern, Mediterranean, and South/Southeast Asian origin.
- Rh incompatibility is manageable but must be identified early — an Rh-negative woman with an Rh-positive partner needs anti-D prophylaxis during pregnancy.
- Hepatitis B: if one partner is HBsAg-positive and the other lacks immunity (Anti-HBs negative), vaccination of the non-immune partner is strongly recommended before marriage.
- HIV: a positive result does not preclude marriage but enables informed decision-making, treatment, and prevention of mother-to-child transmission.
This is a shared conversation. Sign in to Orris to start your own chat.