What is immunomodulatory in ayurveda
immunomodulatory herbs Ayurveda Rasayana mechanisms 2024
Ayurveda immunomodulatory Rasayana herbs
Ayurveda immunomodulation herbs
https://pmc.ncbi.nlm.nih.gov/articles/PMC8422837
Immunomodulation in Ayurveda
The Ayurvedic Concept of Immunity
-
Vyadhikshamatva - literally "the power to resist disease." This is the Ayurvedic equivalent of immunity. It has two components:
- Vyadhi Bala Virodhitva - resistance to the onset of disease
- Vyadhi Utpada Pratibandhakatva - suppression of disease after it has started
-
Ojas - considered the finest, most refined product of tissue metabolism (Dhatu Poshana). Ojas is the biological correlate of vitality and immune strength. Depleted Ojas = compromised immunity.
Rasayana - The Immunomodulatory Branch of Ayurveda
- Prolonging life (Dirghayu)
- Enhancing memory and intellect
- Freedom from disease (Niramaytva)
- Strengthening tissue quality (Dhatu Pushti)
- Resistance against environmental stress
Key Rasayana Herbs and Their Immunomodulatory Mechanisms
| Herb | Sanskrit Name | Key Active Compounds | Immune Mechanism |
|---|---|---|---|
| Withania somnifera | Ashwagandha | Withanolides, alkaloids | Upregulates Th1 polarization, boosts IFN-γ, IL-2, GM-CSF; NK cell activation; adaptogenic (HPA axis modulation) |
| Tinospora cordifolia | Guduchi / Giloy | Tinosporin, arabinogalactan | Macrophage activation, phagocytosis enhancement, modulates CD4+/CD8+ T cells, NF-κB regulation |
| Emblica officinalis | Amalaki / Amla | Tannins, Vitamin C, emblicanin | NK cell-induced cytotoxic activity; reduces TNF and IL-1 (pro-inflammatory); upregulates IL-10 (anti-inflammatory) |
| Ocimum sanctum | Tulsi | Eugenol, rosmarinic acid | Anti-inflammatory via COX-2 inhibition, enhances T-lymphocyte proliferation |
| Asparagus racemosus | Shatavari | Saponins, shatavarins | Humoral and cell-mediated immunity, antibody production |
| Bacopa monnieri | Brahmi | Bacosides | Reduces neuroinflammation, modulates serotonin-immune axis |
| Glycyrrhiza glabra | Mulethi / Licorice | Glycyrrhizin | Modulates CD4+/CD8+ ratio, antiviral and anti-inflammatory |
| Terminalia chebula | Haritaki | Chebulic acid, tannins | Antioxidant-mediated immune support, antimicrobial |
Molecular Mechanisms of Rasayana Immunomodulation
-
Innate Immunity Enhancement
- Macrophage activation and increased phagocytosis
- Natural Killer (NK) cell stimulation
- Enhanced cytotoxic granule exocytosis
-
Adaptive Immunity Modulation
- T-lymphocyte proliferation (Th1/Th2 balance)
- Immunoglobulin production
- Dendritic cell modulation
- CD4+/CD8+ T cell ratio regulation
-
Cytokine Regulation
- Downregulation of pro-inflammatory cytokines: TNF-α, IL-1, IL-6
- Upregulation of anti-inflammatory cytokines: IL-10
- Enhancement of IFN-γ and IL-2
-
NF-κB Pathway Inhibition - herbs like Guduchi and Nirgundi reduce inflammatory cytokines via this pathway
-
Psycho-Neuro-Immune Axis - Adaptogenic herbs regulate the HPA (hypothalamic-pituitary-adrenal) axis, reducing cortisol and thereby preventing immune suppression from chronic stress
-
Antioxidant Mechanisms - Reduction of reactive oxygen species (ROS) preserves immune cell integrity
Classical Formulations
- Chyavanaprash - the most famous Rasayana, built around Amalaki; enhances respiratory immunity
- Brahma Rasayana - classical rejuvenative formula
- Dhatryadi Rasayana - polyherbal with demonstrated antioxidant and immunomodulatory activity
- Triphala - combination of Amalaki, Haritaki, Vibhitaki; antioxidant and immune support
- Sudarshana Ghana Vati - used in febrile illness
Ayurvedic Principles Behind Immunomodulation
- Tridosha (Vata, Pitta, Kapha) - imbalance leads to susceptibility to disease
- Agni (digestive fire) - strong Agni produces quality Dhatus and ultimately Ojas; weak Agni generates Ama (toxins) that block immunity
- Srotas (channels) - open channels allow proper nourishment and waste removal, supporting immune vigilance
- Satva (mental purity) - mind-body connection recognized in what modern science calls psychoneuroimmunology
Recent Clinical Evidence
- Dipankar et al. (2025, Cureus) - review of Ashwagandha's immunomodulatory and neuroprotective properties [PMID: 40951251]
- Bhandari et al. (2024) - systematic review of traditional formulations including Ayurvedic herbs against COVID-19 [PMID: 37972056]
- Prakash et al. (2024, Cureus) - immunomodulatory effects of a herbo-mineral Ayurvedic formulation in experimental models [PMID: 38800281]
Summary
Pongamia glabra
Pongamia glabra pharmacological activity
Pongamia glabra Karanja Ayurveda medicinal uses pharmacology 2024
https://openmedicinalchemistryjournal.com/VOLUME/17/ELOCATOR…
PMID: 34470730
Pongamia glabra (Karanja / Indian Beech)
Botanical Identity
| Feature | Details |
|---|---|
| Scientific name | Pongamia glabra Vent. (synonym: Pongamia pinnata (L.) Pierre; Millettia pinnata) |
| Family | Fabaceae (Leguminosae) |
| Common names | Karanja (Hindi/Sanskrit), Indian Beech, Pongam tree, Honge (Kannada), Pungai (Tamil), Kanuga (Telugu) |
| Distribution | Throughout India up to 1,200 ft elevation; also Japan, Australia, Malaysia, Southeast Asia |
Ayurvedic Properties (Guna-Karma)
| Property | Value |
|---|---|
| Rasa (taste) | Tikta (bitter), Katu (pungent), Kashaya (astringent) |
| Vipaka (post-digestive taste) | Katu (pungent) |
| Veerya (potency) | Ushna (hot) |
| Guna (qualities) | Laghu (light), Teekshna (sharp/piercing) |
| Dosha action | Balances Kapha and Vata; may aggravate Pitta in excess |
| Primary indications | Kushtha (skin diseases), Krimiroga (parasitic infections), Vrana (wounds/ulcers) |
Sanskrit Synonyms
- Karanja - the most common name
- Naktamala - the tree that glows at night
- Ghritapura - rich in fatty substance
- Udakirya - dispels diseases
Parts Used and Their Applications
| Plant Part | Application |
|---|---|
| Seed oil (Karanja taila) | Skin diseases, eczema, psoriasis, wounds, hemorrhoids, acne |
| Bark | Wound washing decoction, hemorrhoids, anti-inflammatory |
| Leaves | Digestive, laxative, anthelmintic; used in diarrhea, dyspepsia, conjunctivitis |
| Root bark | Applied as paste in scrofulous (lymph node) enlargements |
| Flowers | Used in diabetes, Kapha-Vata imbalances |
| Seeds | Anthelmintic, antifungal, anti-skin disease formulations |
Phytochemistry
Flavonoids (most significant class)
- Karanjin - a furanoflavonol; the trademark compound of this species; first compound ever isolated from it
- Pongamol - a benzofuranoid flavonoid; key bioactive compound with diverse pharmacological activity
- Kanjone, Pinnatin, Pongapin - additional furanoflavones
- Lanceolatin A and B - flavanones
Other Phytochemicals
- Alkaloids - terpene alkaloids
- Tannins and polyphenols - antioxidant activity
- Fixed oils / Fatty acids - seed oil contains oleic acid (44-71%), linoleic acid (11-18%), palmitic acid, stearic acid, arachidic acid, behenic acid, eicosenoic acid
- Steroids and triterpenes - cycloartenol, β-sitosterol
- Carbohydrates and glycosides
Note: Current Science first reported the isolation of pongamol from Pongamia glabra oil; its molecular formula is C₉H₇O₂ (later revised after methoxy compound analysis).
Pharmacological Activities
1. Antifungal / Antimicrobial
2. Anti-inflammatory
3. Antidiabetic / Anti-hyperglycaemic
4. Antioxidant
5. Anticancer
6. Anthelmintic
7. Wound Healing
8. Antiviral
9. Anti-diarrhoeal
Classical Ayurvedic Uses
- Kushtha (skin diseases): Karanja oil is a primary ingredient in medicated oils for eczema, psoriasis, and fungal infections
- Krimiroga (worm infestations): Root and seed preparations
- Vrana shodhana (wound cleansing): Bark decoction washes
- Arsha (hemorrhoids): Oil applied externally; bark decoction used as sitz bath
- Netra roga (eye diseases): Young leaf decoction instilled in conjunctivitis
- Medoroga (obesity/fat disorders): Bitter tikta rasa helps reduce Kapha and medas
- Prameha (diabetes): Flowers and leaves used
Modern Formulations with Karanja
- De-Pile Ointment - external and internal hemorrhoids
- Dermasyl Skin Ointment - eczema, scabies (anti-infective)
- Dermafex Oil/Soap - eczema, psoriasis
Biofuel Application
Safety
Carbon clearance test
carbon clearance test phagocytosis immunomodulatory assay protocol principle procedure
carbon clearance phagocytosis immunomodulatory test
https://pmc.ncbi.nlm.nih.gov/articles/PMC3731030
carbon clearance test formula phagocytic index K calculation mononuclear phagocyte system immunostimulant
https://pmc.ncbi.nlm.nih.gov/articles/PMC2996070
Carbon Clearance Test
Definition and Purpose
Principle
- Kupffer cells in the liver (primary site)
- Macrophages in the spleen
- Other fixed and free macrophages of the MPS
A higher phagocytic index = more active macrophages = enhanced non-specific immunity
Animals Used
- Swiss albino mice (most common) - typically 20-30 g
- Wistar rats (less common)
- Group size: 6 animals per group (minimum)
Materials Required
| Material | Detail |
|---|---|
| Indian ink (colloidal carbon) | Diluted 1:5 in normal saline (or 0.3 ml/30g mouse body weight) |
| 0.1% Sodium carbonate solution | For lysing blood and releasing carbon |
| Spectrophotometer | Reads absorbance at 660-675 nm |
| Retro-orbital capillary tube / syringe | For blood collection |
Procedure (Step-by-Step)
1. Pre-treatment
- Administer the test drug/extract orally (p.o.) for 7-14 days (commonly 10 days)
- Groups:
- Normal control (vehicle only)
- Standard immunostimulant (e.g., Levamisole 50 mg/kg, or LPS)
- Standard immunosuppressant (e.g., Cyclophosphamide 30 mg/kg i.p.) - used as negative control
- Test drug at low and high doses
2. Carbon Injection
- 48 hours after the last dose, inject Indian ink (colloidal carbon) intravenously (i.v.) via the tail vein at a dose of 0.1 ml/10g body weight (or 0.3 ml/30g)
3. Blood Sampling
- T₁ = 0 minutes (immediately after injection)
- T₂ = 15 minutes after injection
4. Sample Processing
- Mix 50 µl blood with 4 ml of 0.1% sodium carbonate solution
- Sodium carbonate lyses the RBCs and releases carbon particles into solution
- Read optical density (OD) at 660-675 nm using spectrophotometer
5. At End of Experiment (Organ Weight Correction)
- Sacrifice the animals
- Weigh liver and spleen
- Record body weight
- These are used to calculate the corrected phagocytic index
Calculations
Step 1: Phagocytic Index (K)
- OD₁ = Optical density at time T₁ (0 min)
- OD₂ = Optical density at time T₂ (15 min)
- T₂ - T₁ = Time interval = 15 minutes
Step 2: Corrected Phagocytic Index / Stimulation Index (α)
- W = Body weight (grams)
- L = Liver weight (grams)
- S = Spleen weight (grams)
Interpretation:
| Phagocytic Index (IF) | Interpretation |
|---|---|
| IF > 1 (compared to control) | Immunostimulant activity |
| IF < 1 (compared to control) | Immunosuppressant activity |
| IF = 1 | No significant effect |
What the Test Measures
| Parameter Assessed | System Involved |
|---|---|
| Phagocytosis rate | Kupffer cells (liver), splenic macrophages |
| Non-specific innate immunity | Mononuclear Phagocyte System (MPS) |
| Reticuloendothelial system (RES) activity | Fixed tissue macrophages |
| Macrophage activation | First line of defense |
Significance in Immunomodulatory Drug Evaluation
- Immunostimulant activity if it significantly increases the phagocytic index (K and α) vs. control
- Immunosuppressant activity if it significantly decreases the phagocytic index
- Hemagglutination (HA) titer - humoral (antibody-mediated) immunity
- Delayed Type Hypersensitivity (DTH) - cell-mediated immunity
- Neutrophil adhesion test - neutrophil function
Advantages
- Simple, inexpensive, and reproducible
- Measures functional phagocytic capacity (not just cell counts)
- Well-validated in vivo model with decades of use
- Applicable across a wide range of drug categories
- Sensitive enough to detect dose-dependent changes
Limitations
- Measures only non-specific (innate) immunity - does not evaluate adaptive immunity
- Does not distinguish between liver and spleen contribution separately
- Cannot identify molecular mechanism of action
- Requires animal subjects (ethical considerations)
- Carbon particles are not pathogens - results may not perfectly mimic infection scenarios
Examples of Drugs Tested Using Carbon Clearance
| Drug/Extract | Effect on Phagocytic Index | Reference |
|---|---|---|
| Aegle marmelos fruit extract | Significant increase | PMC3731030 |
| Roscoea procera rhizome extract | Significant increase | PMC2996070 |
| Cyclophosphamide (standard) | Significant decrease (immunosuppression) | Multiple studies |
| Levamisole (standard) | Significant increase (immunostimulation) | Multiple studies |
| Ashwagandha, Guduchi | Increase - supporting Rasayana claims | Multiple herbal studies |
Serum immunoglobin s
serum immunoglobulins IgG IgA IgM IgD IgE classes structure functions clinical significance
Serum Immunoglobulins
What Are Immunoglobulins?
Basic Structure of Immunoglobulins
- 2 Heavy (H) chains - identical, ~50 kDa each; determine the class (isotype)
- 2 Light (L) chains - identical, ~25 kDa each; either κ (kappa) or λ (lambda) type
- Chains are held together by inter-chain disulfide bonds and non-covalent interactions
Regions:
| Region | Function |
|---|---|
| Fab (Fragment antigen-binding) | Antigen recognition; contains variable (V) domains |
| Fc (Fragment crystallizable) | Effector functions - complement activation, Fc receptor binding, placental transfer |
| Hinge region | Flexible; present in IgG, IgA, IgD (not IgM or IgE); allows variable distance between Fab arms |
Enzymatic Cleavage:
- Papain cuts above the hinge → 2 Fab fragments + 1 Fc fragment
- Pepsin cuts below the hinge → 1 F(ab')₂ fragment (bivalent) + pFc' fragment
Schematic Structures of All Five Classes
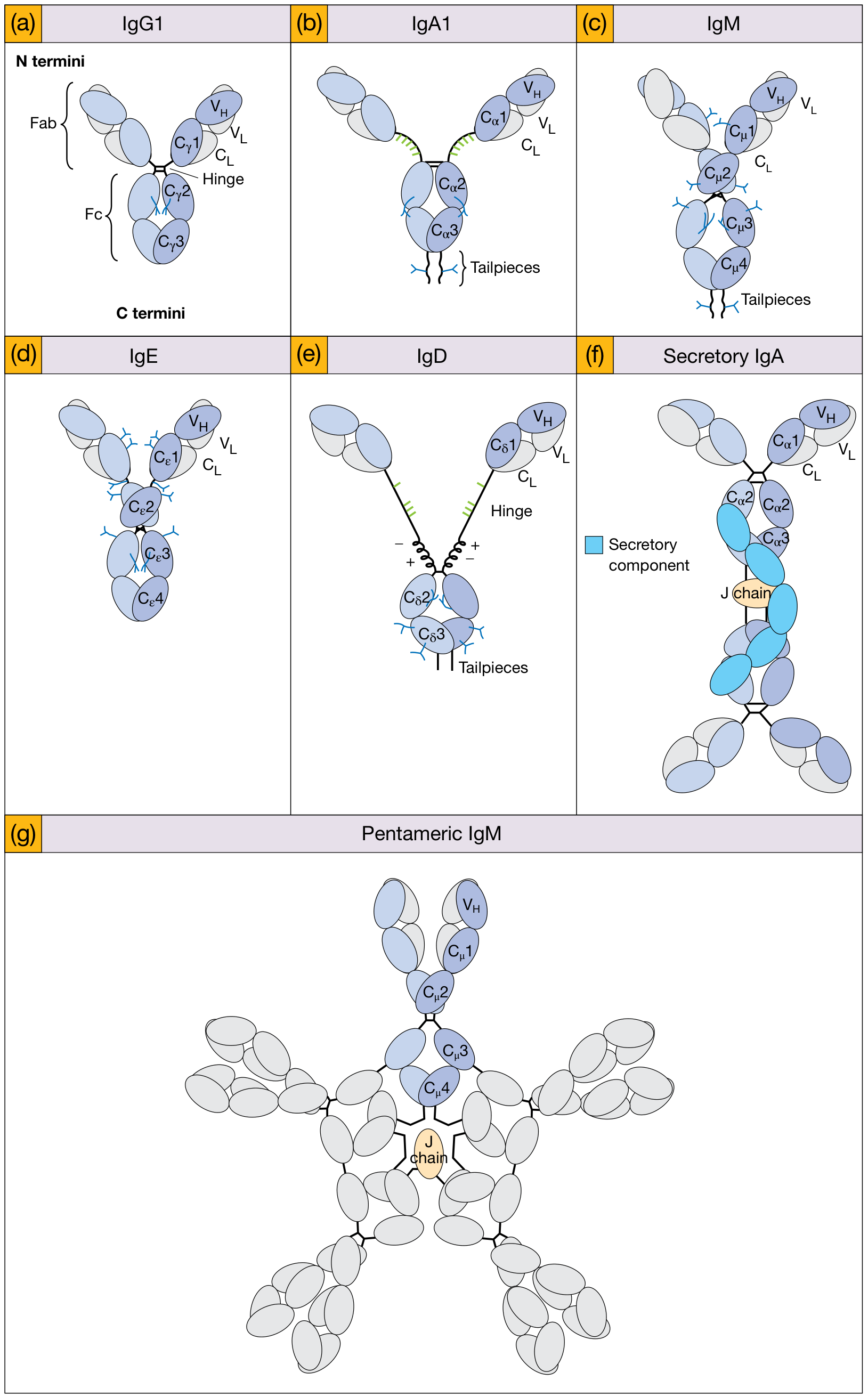
The Five Classes of Serum Immunoglobulins
Properties Comparison Table
| Property | IgG | IgA | IgM | IgD | IgE |
|---|---|---|---|---|---|
| Heavy chain | γ (gamma) | α (alpha) | μ (mu) | δ (delta) | ε (epsilon) |
| Subclasses | IgG1-4 | IgA1-2 | None | None | None |
| Structure | Monomer | Monomer/Dimer | Pentamer | Monomer | Monomer |
| Molecular weight (kDa) | 154 | 160 | 900 | 185 | 190 |
| % of serum Ig | 75-85% | 5-15% | 5-10% | <1% | <1% |
| Serum concentration | 7-16 g/L | 0.7-4 g/L | 0.5-2 g/L | ~0.04 mg/L | 0.02-0.1 mg/L |
| Half-life (days) | 23 (longest) | 6 | 5 | 2-3 | 2-3 |
| T-cell requirement | Dependent | Dependent | Independent | Independent | Dependent |
| Timing | Later, memory | Later, memory | Early, primary | Early, primary | Later, memory |
| Hinge region | Yes | Yes | No (extra domain) | Yes (long) | No (extra domain) |
| Constant domains | 3 | 3 | 4 | 3 | 4 |
| J chain | No | Yes (dimer) | Yes (pentamer) | No | No |
Detailed Profile of Each Class
1. IgG - The Dominant Serum Immunoglobulin
- Most abundant - accounts for 75-85% of total serum Ig
- Monomeric with a flexible hinge region
- Longest half-life - 23 days (due to FcRn neonatal Fc receptor recycling)
- Only Ig that crosses the placenta - provides passive immunity to neonate for 3-6 months
- Four subclasses (IgG1 > IgG2 > IgG3 > IgG4 in serum concentration):
- IgG1 and IgG3: Best at complement activation and ADCC (antibody-dependent cellular cytotoxicity)
- IgG2: Responds to polysaccharide antigens (e.g., bacterial capsules); only triggered at high antigen density
- IgG4: Does NOT activate complement; important in allergy desensitization
- Opsonization (enhances phagocytosis)
- Complement activation (classical pathway)
- Neutralization of toxins and viruses
- ADCC via NK cells
- Neonatal passive immunity (via placenta)
- Chronic liver disease
- Subacute or chronic infections
- Connective tissue diseases (SLE, RA)
- IgG myeloma (monoclonal)
- Hypogammaglobulinemia
- X-linked agammaglobulinemia (Bruton's)
- Nephrotic syndrome (protein loss)
2. IgA - The Mucosal Guardian
- Two forms:
- Serum IgA: Monomeric; 5-15% of serum Ig
- Secretory IgA (SIgA): Dimeric IgA + J chain + Secretory Component (SC); found in mucosal secretions (saliva, tears, breast milk, gut, respiratory secretions)
- Secretory component protects IgA from proteolytic digestion in harsh mucosal environments
- Two subclasses: IgA1 (longer hinge, susceptible to bacterial proteases) and IgA2 (shorter hinge, more protease-resistant)
- First line of defense at mucosal surfaces (respiratory, GI, urogenital tracts)
- Neutralization of pathogens before systemic entry
- Does NOT activate complement efficiently
- Present in colostrum/breast milk - protects newborn gut
- Selective IgA deficiency (most common primary immunodeficiency) - recurrent respiratory and GI infections, increased risk of atopic disease
- Elevated in: chronic liver disease, IgA nephropathy, IgA myeloma
3. IgM - The First Responder
- Pentameric structure - 5 monomeric units held together by J chain
- Largest immunoglobulin (900 kDa)
- First antibody produced in primary immune response (before class-switching)
- Has 10 antigen-binding sites (bivalent × 5 monomers) - highly efficient agglutination
- 4 constant domains (Cμ1-4) instead of hinge region
- Complement activation: IgM undergoes a "star-to-staple" conformational change upon antigen binding, exposing C1q-binding sites
- Best complement activator (classical pathway)
- Agglutination of bacteria/RBCs
- First antibody in primary immune response (diagnostic marker of acute/recent infection)
- ABO blood group antibodies are IgM (natural isohemagglutinins)
- Rheumatoid factor (anti-IgG antibody) is usually IgM
- Elevated IgM = acute or recent infection, primary response
- Waldenström's macroglobulinemia - IgM-secreting B-cell malignancy → hyperviscosity syndrome
- Low IgM = XLA, combined immunodeficiency
4. IgD - The B-cell Regulator
- Present at very low serum concentrations (<1%)
- Has a long, flexible hinge region
- Co-expressed with IgM on the surface of mature naive B cells (as antigen receptor)
- Role in B cell activation and suppression - helps control lymphocyte activation
- May protect against microbes in the upper respiratory tract
- Some evidence for regulatory role, maintenance of B cell memory, induction of TNF-α, IL-1β
- Generally limited clinical significance
- IgD myeloma - rare plasma cell malignancy; M spike detected on serum protein electrophoresis
- Useful as marker of B-cell maturation stage
5. IgE - The Allergy Antibody
- Lowest serum concentration of all Igs (trace levels, ~0.05 mg/L)
- Monomeric with 4 constant domains (Cε1-4), no hinge region
- Most IgE is bound to high-affinity FcεRI receptors on mast cells and basophils in tissues (not free in serum)
- Cross-linking of mast cell-bound IgE by allergen triggers degranulation → histamine, prostaglandins, leukotrienes → allergic reaction
- Short half-life in serum (2-3 days) but long-lived when bound to mast cells
- Mediates type I (immediate) hypersensitivity (allergies, anaphylaxis)
- Defense against helminth (worm) parasites - via eosinophil activation (ADCC)
- Activates mast cells and basophils
- Elevated IgE = atopic diseases (asthma, eczema, allergic rhinitis), parasitic infections
- Very high IgE = Hyper-IgE syndrome (Job syndrome) - recurrent bacterial infections + eczema
- Used to monitor allergen immunotherapy response
- Measured as total IgE and allergen-specific IgE (RAST/ImmunoCAP testing)
Fc Region Interactions Summary
| Fc Receptor / Component | Interaction | Function |
|---|---|---|
| Macrophages (FcγR) | IgG Fc | Opsonization |
| Neutrophils (FcγR) | IgG Fc | Opsonization |
| NK cells (FcγRIII/CD16) | IgG Fc | ADCC (killing of antibody-coated cells) |
| Mast cells (FcεRI) | IgE Fc | Allergic reactions, antiparasitic |
| T cells (FcγR) | IgG Fc | Checkpoint regulation |
| Complement C1q | IgG/IgM Fc | Classical pathway activation |
| Neonatal FcRn | IgG Fc | Placental transfer + IgG recycling (long half-life) |
| Epithelial cells (pIgR) | IgA/IgM J chain | Transcytosis across mucosal epithelium → secretory Ig |
Isotype, Allotype, and Idiotype
| Term | Definition | Determined by |
|---|---|---|
| Isotype | Class/subclass identity (IgG, IgA, etc.) | Fc portion; same in all people |
| Allotype | Inherited polymorphisms in constant region | Fc portion; differs between people |
| Idiotype | Unique antigen-binding region sequences | Variable (V) region; unique to each clone |