Katzung pharmacologynotes on estrogen, progestins and androgens
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have all the essential content from Katzung. Let me compile the comprehensive notes.
Katzung Pharmacology: Estrogens, Progestins & Androgens
(Katzung's Basic and Clinical Pharmacology, 16th Edition - Chapter 40)
THE ESTROGENS
Natural Estrogens
The three major endogenous estrogens are:
- Estradiol (17β-estradiol, E2) - the major secretory product of the ovary and the most potent
- Estrone (E1) - formed mainly in the liver from estradiol or in peripheral tissues from androstenedione
- Estriol (E3) - weakest; formed peripherally
Estradiol is produced by theca and granulosa cells of the ovarian follicle during the follicular phase. After ovulation, the corpus luteum produces estrogens and progesterone.
At menopause, significant estrogen levels persist via conversion of androstenedione to estrone and estradiol in adipose tissue.
Synthetic Estrogens
- Diethylstilbestrol (DES) - nonsteroidal; daughters of DES-treated mothers have increased risk of vaginal adenocarcinoma
- Ethinyl estradiol, mestranol - used in oral contraceptives
- Conjugated equine estrogens (Premarin) - used in HRT

Pharmacokinetics
- Estradiol is well absorbed via oral, transdermal, vaginal, and IM routes
- Oral estrogen undergoes significant first-pass metabolism; converted to estrone in gut/liver
- Transdermal route avoids first-pass effect: 50-100 mcg estradiol transdermally ≈ 0.625-1.25 mg oral conjugated estrogens for gonadotropin suppression
- Oral estrogen increases hepatic synthesis of CBG, SHBG, angiotensinogen (renin substrate), TBG - transdermal preparations do NOT
- Elimination: conjugated in liver, excreted in urine and bile
Mechanism of Action
- Estrogens diffuse into cells and bind cytoplasmic/nuclear estrogen receptors (ER-α, ER-β)
- Ligand-receptor complex dimerizes and binds estrogen response elements (EREs) on DNA
- Coactivators and corepressors modulate transcription
- Estrogen-receptor complex can also interact with transcription factors (AP-1, SP-1) without direct DNA binding
Physiologic & Pharmacologic Effects
| System | Effect |
|---|---|
| Female genitalia | Growth and development; endometrial proliferation; cervical mucus thinning |
| Breasts | Ductal development, fat deposition |
| Bone | Inhibits osteoclast activity, maintains bone density; epiphyseal closure |
| Cardiovascular | Favorable lipid profile (↑HDL, ↓LDL); vasodilation |
| Liver | ↑ CBG, SHBG, TBG, angiotensinogen, clotting factors (II, VII, IX, X) |
| CNS | Positive mood effects; hot flush relief |
| Metabolic | Slight ↑ glucose tolerance impairment at high doses |
Clinical Uses of Estrogens
- Menopausal hormone therapy (HRT) - vasomotor symptoms (hot flushes), urogenital atrophy, osteoporosis prevention; best initiated early in menopause
- Primary hypogonadism / ovarian failure - replacement in Turner syndrome, premature ovarian insufficiency
- Oral contraception (with progestins)
- Osteoporosis prevention/treatment
- Dysmenorrhea, endometriosis (with progestins)
- Acne/hirsutism - suppress ovarian androgen via gonadotropin suppression
- Formerly: prostate cancer (DES), breast cancer in postmenopausal women
Adverse Effects of Estrogens
- Uterine bleeding - most important; use smallest effective dose cyclically; always add progestin to prevent endometrial hyperplasia
- Cancer risk: endometrial carcinoma (15x risk with large-dose prolonged use; prevented by adding progestin); small ↑ in breast cancer with prolonged use
- Thromboembolic disease - ↑ risk via increased clotting factors
- Nausea, breast tenderness - minimize with lowest dose
- Cholestasis, gallbladder disease
- Hypertension
- Migraine headaches
- DES exposure in utero - vaginal adenocarcinoma in daughters
Contraindications
- Estrogen-dependent tumors (endometrial, breast carcinoma)
- Undiagnosed vaginal bleeding
- Active liver disease
- History of thromboembolic disorders
- Heavy smokers (especially >35 years)
THE PROGESTINS
Natural Progestins: Progesterone
- The most important human progestin; also a precursor to estrogens, androgens, and adrenocortical steroids
- Synthesized in ovary (primarily corpus luteum), testis, adrenal cortex, and placenta (during pregnancy)
- Normal male: 1-5 mg/day; females - follicular phase: minimal; luteal phase: 0.5-2+ mcg/dL
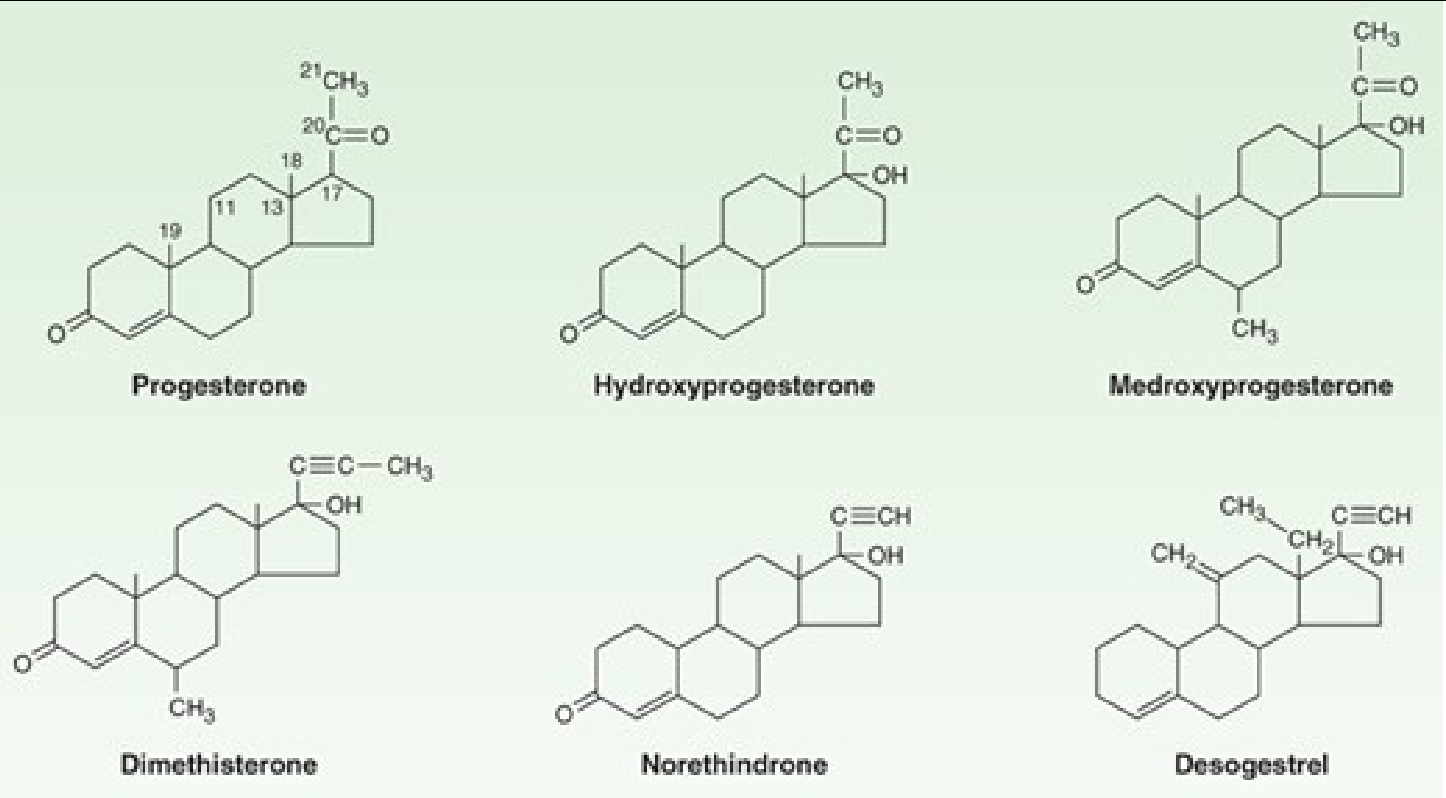
Synthetic Progestins
Two major classes:
- Progesterone derivatives (C-21): medroxyprogesterone acetate, megestrol acetate, hydroxyprogesterone caproate - low androgenic activity
- 19-Nortestosterone derivatives (C-19): norethindrone, norgestrel, levonorgestrel, desogestrel, gestodene, norgestimate - more androgenic; used in oral contraceptives
Pharmacokinetics
- Progesterone: rapidly absorbed by any route; half-life ~5 minutes; almost completely metabolized in first pass through liver - making ordinary oral preparations ineffective
- Micronized progesterone (oral) overcomes first-pass problem
- Metabolism: converted to pregnanediol in liver, conjugated with glucuronic acid, excreted in urine as pregnanediol glucuronide (used as index of progesterone secretion)
- Synthetic progestins: longer half-lives, less first-pass metabolism; most given orally or IM
Mechanism of Action
- Progestins enter cells, bind progesterone receptors (PR-A and PR-B) in nucleus and cytoplasm
- Ligand-receptor complex dimerizes and binds progesterone response elements (PREs)
- PRE is similar to corticosteroid response element; specificity depends on which receptor isoform is present
- PR forms homodimers (A-A, B-B) or heterodimers (A-B)
Physiologic Effects of Progesterone
| System | Effect |
|---|---|
| Uterus | Converts proliferative to secretory endometrium; ↓ uterine contractility (relaxes myometrium); ↑ viscosity of cervical mucus (blocks sperm penetration) |
| Temperature | ↑ basal body temperature by ~0.5°F after ovulation (thermogenic effect) |
| Breasts | Lobulo-alveolar development |
| Carbohydrate metabolism | ↑ basal insulin levels and insulin response to glucose; promotes glycogen storage (permissive for insulin); promotes ketogenesis |
| Aldosterone antagonism | Competes with aldosterone at mineralocorticoid receptor → natriuresis (compensatory aldosterone ↑ follows) |
| CNS | Mild sedative/anesthetic properties; raises seizure threshold |
| Fat | Stimulates lipoprotein lipase; favors fat deposition |
Clinical Uses of Progestins
- Hormonal contraception - most important use (with estrogen or progestin-only)
- Hormone replacement therapy (HRT) - added to estrogen to prevent endometrial hyperplasia/cancer in women with intact uterus
- Dysfunctional uterine bleeding - progesterone or MPA; withdrawal induces shedding
- Dysmenorrhea, endometriosis - suppress ovulation
- Endometrial carcinoma - high-dose megestrol or MPA for palliation
- Premenstrual syndrome - limited evidence; only effective with ovulation-suppressing doses
- Diagnostic use: administration followed by withdrawal bleeding confirms adequate estrogen priming (tests endometrial responsiveness)
- Threatened/habitual abortion - prevent miscarriage in corpus luteum deficiency
Adverse Effects & Contraindications
- Androgenic progestins (19-nortestosterone derivatives): ↓ HDL cholesterol - cardiovascular concern
- ↑ Blood pressure in some patients
- Combined estrogen + progestin HRT may ↑ breast cancer risk significantly more than estrogen alone
- Cholestatic jaundice (especially first 3 cycles)
- Depression in ~6-8% with some preparations
OTHER OVARIAN HORMONES
- The normal ovary also produces small amounts of testosterone, androstenedione, DHEA - physiologic roles include normal pubic/axillary hair, female libido, and metabolic effects
- Inhibin (αβ dimer): inhibits FSH secretion
- Activin (ββ dimer): stimulates FSH secretion; modulates response to LH/FSH in granulosa cells
- Relaxin: promotes cervical ripening, ↑ glycogen synthesis, ↓ uterine contractility
HORMONAL CONTRACEPTION
Combined Oral Contraceptives (COCs)
Contain estrogen (ethinyl estradiol) + progestin in fixed or sequential formulations.
Mechanism:
- Suppression of FSH and LH (prevents follicle development and ovulation)
- Alteration of cervical mucus (hostile to sperm)
- Alteration of endometrium (hostile to implantation)
- Altered tubal motility
Cardiovascular risks:
- Thromboembolism: ↑ 4-fold; attributable to estrogen component (↑ clotting factors)
- MI risk: increased in obese, hypertensive, hyperlipidemic, diabetic, or smoking women; risk 4/100,000 in non-smokers aged 30-40 vs. 185/100,000 in heavy smokers aged 40-44
- Stroke: risk ↑ in current users >35 years; subarachnoid hemorrhage ↑ in both current and past users
- Progestin component ↓ HDL proportional to its androgenic activity
Cancer:
- COCs may reduce risk of ovarian and endometrial cancer (protective with long use)
- Small ↑ in breast cancer with prolonged use (ongoing evidence assessment)
Other adverse effects:
- Cholestatic jaundice, hepatic adenomas
- Gallbladder disease
- Depression (6-8%)
- Hypertension (estrogen component via renin-angiotensin)
ESTROGEN & PROGESTIN ANTAGONISTS
Selective Estrogen Receptor Modulators (SERMs)
Tamoxifen:
- Partial agonist/antagonist; antagonist in breast, agonist in bone and uterus
- Used in ER-positive breast cancer treatment and chemoprevention
- 35% ↓ contralateral breast cancer
- Favorable lipid profile, ↑ bone density
- Risk: endometrial cancer (agonist at uterus)
Raloxifene:
- Antagonist at breast and uterus; agonist at bone
- No ↑ endometrial cancer risk (unlike tamoxifen)
- Used for postmenopausal osteoporosis and breast cancer risk reduction
Clomiphene:
- Partial agonist/antagonist; blocks estrogen feedback at hypothalamus
- Results in ↑ GnRH → ↑ FSH/LH → ovulation induction
- Used for anovulatory infertility (especially PCOS)
- Dose: 100 mg/day x 5 days
- Adverse effects: hot flushes, ovarian enlargement, ~10% multiple pregnancy, visual disturbances
- Caution: possible ↑ low-grade ovarian cancer risk with >1 year use
Mifepristone (RU-486):
- Potent progesterone and glucocorticoid receptor antagonist
- Used for medical abortion (with misoprostol), endometriosis, Cushing syndrome
THE ANDROGENS & ANABOLIC STEROIDS
Synthesis & Secretion
- Testosterone is the most important androgen secreted by the testis
- Males: ~8 mg/day produced; 95% from Leydig cells, 5% from adrenals
- Plasma levels: ~0.6 mcg/dL (post-pubertal males); ~0.03 mcg/dL (females)
- The testis also secretes small amounts of DHT, androstenedione, and DHEA
Binding & Transport
- 65% bound to SHBG (sex hormone-binding globulin)
- ~33% bound to albumin
- ~2% free (biologically active)
- SHBG ↑ by: estrogen, thyroid hormone, cirrhosis
- SHBG ↓ by: androgen, growth hormone, obesity
Metabolism
- In target tissues (prostate, skin, seminal vesicles), testosterone is converted to dihydrotestosterone (DHT) by 5α-reductase - the active form in those tissues
- In other tissues (liver, muscle), testosterone acts directly
- In brain: testosterone is aromatized to estradiol which mediates some CNS effects
- Testosterone is metabolized to 17-ketosteroids (androsterone, etiocholanolone) and excreted in urine
Mechanism of Action
- Testosterone or DHT (depending on the tissue) binds the intracellular androgen receptor (AR)
- Ligand-receptor complex translocates to nucleus, binds androgen response elements (AREs)
- Activates gene transcription for male secondary sex characteristics, spermatogenesis, protein anabolism
Physiologic & Pharmacologic Effects
Male secondary sex characteristics (puberty):
- Growth of penis, scrotum, prostate, seminal vesicles
- Pubic, axillary, facial, and body hair growth; male pattern baldness
- Laryngeal enlargement (voice deepening)
- Increased muscle mass and strength
- Bone growth and epiphyseal closure
- Erythropoiesis (↑ RBC production)
Adult males (large doses):
- Suppress FSH/LH → testicular atrophy and decreased spermatogenesis
Women receiving androgens:
- Facial and body hair, deepening voice, clitoral enlargement, frontal baldness, prominent musculature
Anabolic effects:
- ↓ urinary nitrogen excretion (↑ protein synthesis / ↓ protein breakdown)
- Effect more pronounced in women and children than in normal men
Clinical Uses of Androgens
-
Androgen replacement therapy in hypogonadal men:
- Testosterone enanthate or cypionate IM; transdermal patches/gels; subcutaneous pellets
- Start at puberty: 50 mg IM every 4 weeks, gradually increasing; adult dose 200 mg every 2 weeks
- Oral methyltestosterone (25-50 mg/day) or fluoxymesterone (2-10 mg/day) also used
-
Delayed puberty in boys - short-term testosterone to initiate pubertal development
-
Anemia - stimulate erythropoiesis (aplastic anemia, anemia of renal failure - largely replaced by erythropoietin)
-
Wasting/cachexia - anabolic steroids in AIDS wasting, burns, chronic illness
-
Breast cancer - previously used in postmenopausal women (now rarely)
-
Endometriosis - danazol (17α-ethinyl testosterone derivative) suppresses gonadotropins
-
Hereditary angioedema - danazol ↑ C1 esterase inhibitor
| Preparation | Route | Dose |
|---|---|---|
| Methyltestosterone | Oral/sublingual | 25-50 mg/d (oral); 5-10 mg/d (buccal) |
| Fluoxymesterone | Oral | 2-10 mg/d |
| Testosterone enanthate | IM | See text |
| Testosterone cypionate | IM | See text |
| Testosterone transdermal | Skin patch/gel | 2.5-10 mg/d (patch); 5-10 g/d (1% gel) |
Adverse Effects of Androgens
- Virilization in women: hirsutism, acne, clitoromegaly, voice deepening, menstrual irregularity
- Hepatotoxicity: especially 17-alkylated androgens (methyltestosterone, fluoxymesterone) - peliosis hepatis, cholestatic jaundice, hepatocellular carcinoma
- Oral testosterone → liver tumors (avoid)
- Suppression of spermatogenesis - testicular atrophy
- Polycythemia (↑ RBC)
- Premature epiphyseal closure in children
- Cardiovascular: anabolic steroids ↓ HDL, ↑ LDL → atherogenesis; hypertension
- Behavioral: aggression, psychosis with abuse
Androgen Suppression & Antiandrogens
Used in prostate cancer and conditions of androgen excess:
- GnRH agonists (leuprolide, goserelin): continuous stimulation → desensitization → ↓ LH → ↓ testosterone ("medical castration")
- 5α-Reductase inhibitors (finasteride, dutasteride): block conversion of testosterone → DHT; used in BPH, prostate cancer, male pattern baldness
- Androgen receptor antagonists (flutamide, bicalutamide): block AR; used with GnRH agonists for complete androgen blockade
- Abiraterone: inhibits CYP17 (17α-hydroxylase), blocks androgen synthesis; used in castration-resistant prostate cancer
- Spironolactone: aldosterone antagonist with anti-androgenic properties; used in PCOS, hirsutism
Preparations Available
| Class | Examples |
|---|---|
| Estrogens | Conjugated estrogens (Premarin), Estradiol, Estradiol transdermal (Estraderm), Estradiol cypionate (Depo-Estradiol), DES |
| Progestins | Progesterone (Prometrium), Medroxyprogesterone acetate (Provera), Levonorgestrel (Plan B), Megestrol (Megace), Norethindrone acetate (Aygestin) |
| Androgens/Anabolics | Testosterone, Testosterone enanthate (Delatestryl), Testosterone cypionate (Depo-testosterone), Testosterone transdermal (Androderm, AndroGel), Methyltestosterone (Android), Fluoxymesterone (Androxy), Nandrolone decanoate, Oxandrolone, Oxymetholone |
| Antagonists | Anastrozole (Arimidex), Tamoxifen, Raloxifene, Clomiphene, Mifepristone, Bicalutamide (Casodex), Abiraterone (Zytiga) |
Source: Katzung's Basic and Clinical Pharmacology, 16th Edition, Chapter 40 - The Ovary; Chapter 40 (continued) - The Testis
This is a shared conversation. Sign in to Orris to start your own chat.