Now I have all the key images and information. Let me compose a comprehensive, well-structured response:
Strength-Duration (SD) Curve in Orthopedics
What is the Strength-Duration Curve?
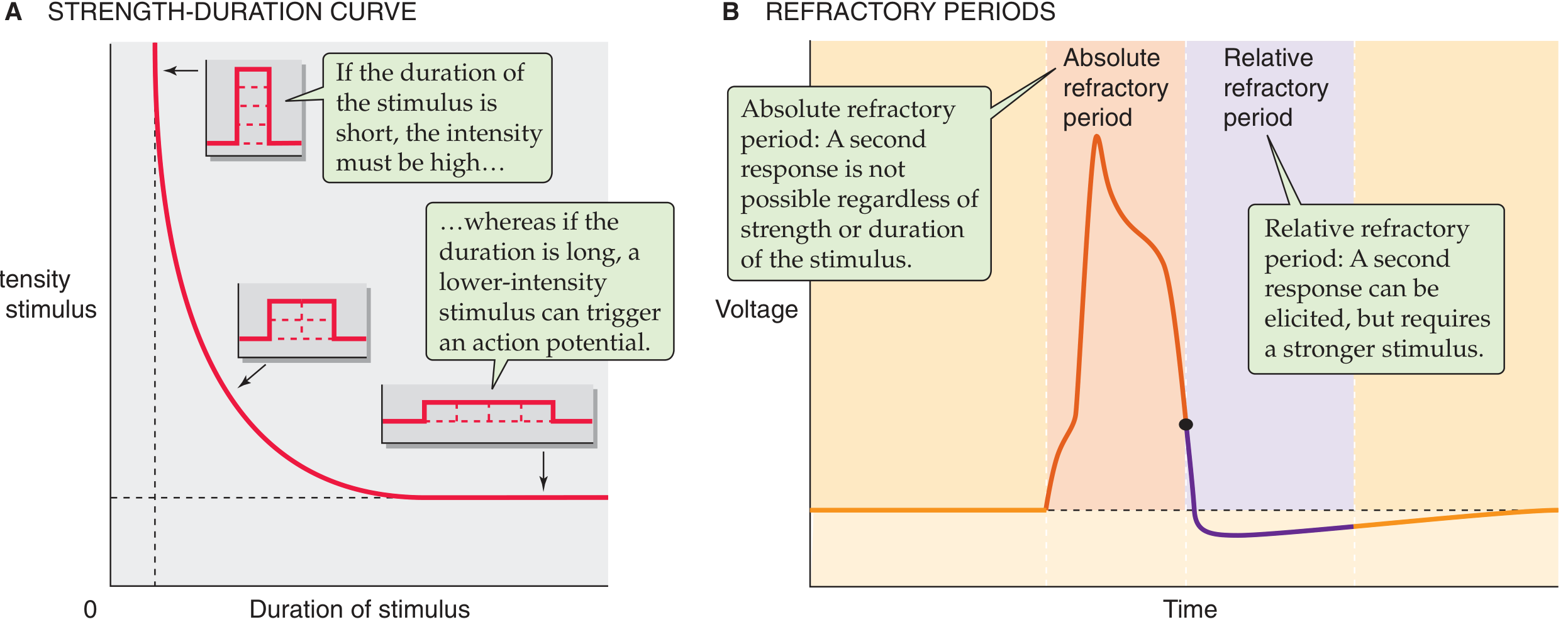
The Strength-Duration (SD) curve is a graphical representation of the inverse relationship between the intensity (strength) of an electrical stimulus and the minimum duration that stimulus must be applied to just reach the threshold for exciting a nerve or muscle (producing a minimal, visible contraction). It is plotted with stimulus intensity (mA or V) on the Y-axis and pulse duration (ms) on the X-axis.
The fundamental principle is: strength × duration = constant (at threshold). A short stimulus must be strong; a long stimulus can be weak - but both can fire the same action potential if their product is sufficient.
Figure: A (left) - Strength-duration curve showing the inverse relationship between stimulus intensity and duration. B (right) - Corresponding action potential with absolute and relative refractory periods. (Medical Physiology, Boron & Boulpaep, p. 276)
Physiological Basis
Law of Excitation (Imax Law / Weiss's Law)
When current is applied to excitable tissue, the charge Q = I × t must meet a minimum threshold. This means:
- A brief, high-intensity stimulus is equivalent in effect to a long, low-intensity stimulus.
- Below a critical duration (the utilization time), no contraction is possible regardless of intensity (vertical asymptote).
- Below a critical intensity (the rheobase), no contraction occurs regardless of duration (horizontal asymptote).
Lapicque's Equation (1907)
I = b (1 + c/d)
Where:
- I = threshold current
- b = rheobase
- c = chronaxie
- d = stimulus duration
Key Parameters
1. Rheobase
The minimum intensity of current required to stimulate a muscle when applied for an infinitely long duration - the horizontal asymptote of the curve.
| Parameter | Normal (Innervated) | Denervated |
|---|
| Rheobase | 2-18 mA (5-35 V) | Increased (higher threshold) |
| Example (Deltoid) | ~14 V / 5 mA | Higher |
| Example (Triceps) | ~18 V / 5 mA | Higher |
- Pulse duration used to measure rheobase: 100-300 ms
- Greater rheobase = lower excitability = more denervation
2. Chronaxie
The minimum time required for a current of exactly double rheobase intensity to just elicit a contraction. It is the single most important diagnostic parameter.
| Parameter | Normal | Denervated |
|---|
| Chronaxie | < 1 ms (0.1-0.7 ms) | > 1 ms (often 10-100 ms) |
| Relationship to excitability | Inversely proportional | Increased = less excitable |
Clinical significance: Chronaxie directly reflects the membrane's time constant. Denervated muscle fibers (which have no fast Na+ channels for rapid depolarization) need much longer stimuli - hence chronaxie increases dramatically.
3. Utilization Time
The time required for a rheobasic strength stimulus to produce a contraction. No response occurs below this time.
Types of SD Curves - Diagnostic Patterns
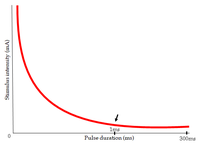
Type 1: Normal Innervation ("Nerve Curve")
Characteristics:
- Shape: Smooth, continuous rectangular hyperbola
- Curve begins to rise sharply at approximately 1 ms - the critical point where nerve can no longer be stimulated efficiently
- At longer durations (>1 ms): Intensity plateaus (rheobase reached)
- Rheobase: 2-18 mA / 5-35 V
- Chronaxie: < 1 ms
- A brisk, snap-like (vermicular) contraction is produced
Interpretation: All nerve fibers intact. Normal lower motor neuron supply preserved.
Type 2: Complete Denervation ("Muscle Curve")
Characteristics:
- Curve is shifted far to the right
- Steep rise continuing even below 100 ms - no plateau at short durations
- No response at short pulse durations (< 1 ms)
- Very high rheobase (may need 50-100+ mA)
- Chronaxie: > 10 ms (often 20-100 ms)
- Contraction is slow, worm-like (peristaltic), not brisk
- Requires galvanic (DC) current, not faradic (AC)
Interpretation: All motor nerve fibers have degenerated (Wallerian degeneration complete). Pure muscle fibers with no innervation are being stimulated directly.
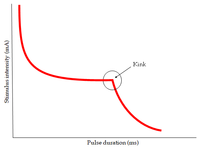
Type 3: Partial Denervation ("Kink Curve")
Characteristics:
- A characteristic kink (inflection point) is visible in the curve
- Left side of the curve (short durations): represents intact innervated fibers - curves like a normal SD curve
- Right side of the curve (longer durations): represents denervated muscle fibers - shifted right with high intensity needed
- The kink appears where the two populations of fibers have different thresholds
Interpretation: Mixed population - some nerve fibers intact, some degenerated. This is the most clinically important pattern, seen in partial nerve injuries, recovering nerves, radiculopathies, and early re-innervation.
Summary Comparison Table
| Feature | Normal | Complete Denervation | Partial Denervation |
|---|
| Curve shape | Smooth hyperbola | Steep, right-shifted | Kinked/bifid |
| Rheobase | 2-18 mA | Very high | Intermediate |
| Chronaxie | < 1 ms | > 10-100 ms | Mixed |
| Rise at | ~1 ms | ~100 ms | Both ~1 ms & ~100 ms |
| Contraction quality | Brisk (vermicular) | Slow, sluggish | Mixed |
| Current type needed | Faradic or galvanic | Galvanic only | Both |
Clinical Applications in Orthopedics
1. Diagnosis of Nerve Injury / Denervation
The SD curve is performed 3 weeks after nerve injury - this allows time for Wallerian degeneration to complete distally. Before 3 weeks, results may not yet show the full denervation pattern.
Used in:
- Peripheral nerve injuries (trauma, stretch, laceration)
- Brachial plexus injuries
- Radiculopathies (disc prolapse, spinal stenosis, spondylosis)
- Compartment syndrome with nerve compromise
- Thoracic outlet syndrome
From Campbell's Operative Orthopaedics (15th ed., 2026): "Galvanic stimulation is useful in determining chronaxie and the strength-duration curve. These determinations frequently give early evidence of denervation after nerve injury and are useful in following the evolution of reinnervation, which is less readily assessed by other methods."
2. Monitoring Re-innervation / Recovery
Serial SD curves over weeks/months reveal:
- Kink appearing in a previously flat denervated curve = early re-innervation (nerve fibers are returning to the muscle)
- Kink shifting left over time = progressive re-innervation
- Return of normal curve pattern = complete re-innervation
- This is often detectable weeks before clinical strength recovery or EMG changes become apparent
3. Lower Motor Neuron vs. Upper Motor Neuron Lesions
- SD curve shows abnormality ONLY in lower motor neuron (LMN) lesions (anterior horn cell, nerve root, peripheral nerve)
- It is normal in upper motor neuron (UMN) lesions (stroke, spinal cord injury above level) because peripheral motor nerves remain intact
- This makes it a useful differentiating tool
4. Guiding Therapeutic Electrical Stimulation
The SD curve's chronaxie value is used to select optimal stimulation parameters for NMES (neuromuscular electrical stimulation) and FES (functional electrical stimulation):
- Use pulse durations around chronaxie for maximum efficiency and patient comfort
- Denervated muscles require much longer pulse widths (10-1000 ms galvanic) vs. innervated muscles (0.1-1 ms faradic)
- Prevents unnecessary fatigue and patient discomfort by avoiding ineffective short pulses
5. Prognosis and Medico-legal Assessment
- A right-shifted curve or high chronaxie = poor prognosis for spontaneous recovery
- Return of the kink = favorable sign of re-innervation
- Serial testing provides objective documentation of nerve recovery progress, useful in medico-legal contexts for compensation assessment
6. Radiculopathy Assessment
A 2023 scoping review (EC Orthopaedics) specifically examined the role of the SD curve in radiculopathy, finding it valuable for detecting segmental denervation changes in patients with disc herniation and nerve root compression.
How the Test is Performed
- Equipment: Galvanic stimulator capable of delivering rectangular pulses from 0.01 ms to 1000 ms
- Electrodes: Active electrode (cathode, negative) placed over the motor point of the muscle; indifferent electrode (anode) placed proximally
- Procedure:
- Start with long-duration pulses (300-1000 ms) to find rheobase
- Progressively reduce pulse duration while increasing intensity to find minimum threshold at each duration
- Plot threshold intensity vs. duration on log-log or semi-log paper
- Timing: Performed 3 weeks post-injury; repeated every 4-6 weeks to monitor progress
Factors Affecting the SD Curve
| Factor | Effect |
|---|
| Denervation | Right shift, higher rheobase, longer chronaxie |
| Re-innervation | Left shift, kink development, falling chronaxie |
| Edema / inflammation | Increases skin resistance, alters readings |
| Temperature | Lower temp raises threshold |
| Electrode placement | Off motor point = inaccurate |
| Subcutaneous fat | Higher tissue resistance |
| Ischemia | Reduces excitability |
| Patient age | Elderly have higher thresholds |
Advantages of the SD Curve
- Quick, inexpensive, non-invasive (relatively)
- Requires minimal training
- Can detect denervation before EMG changes become manifest in some cases
- Serial testing objectively tracks re-innervation
- Distinguishes complete from partial denervation
- Differentiates LMN from UMN lesions
Limitations
- Provides qualitative rather than quantitative grading of degree of denervation
- Cannot localize the site of the nerve lesion
- In large muscles, only a small area of fibers is sampled
- Patient cooperation and pain tolerance affect results
- Not reliable in < 3 weeks post-injury
- Largely superseded by EMG/nerve conduction studies for precise lesion characterization, though still used as a complementary tool and in resource-limited settings
- Intrarater reliability is moderate (r = 0.541) while interrater reliability is better (r = 0.945)
Comparison with Other Electrodiagnostic Tests
| Test | What it measures | Localization | Denervation timing |
|---|
| SD Curve | Excitability of nerve/muscle | No | After 3 weeks |
| EMG | Motor unit action potentials | Yes (partial) | After 3 weeks |
| Nerve Conduction Study | Conduction velocity, amplitude | Yes | After 5-7 days |
| H-reflex | Sensory-motor reflex arc | Proximal | Acute |
Summary
The Strength-Duration curve is a foundational electrodiagnostic tool in orthopedics and physical medicine, mapping the inverse relationship between stimulus strength and pulse duration needed to excite nerve and muscle. Its key parameters - rheobase (minimum current at infinite duration) and chronaxie (duration at twice rheobase) - shift predictably with denervation, allowing clinicians to:
- Diagnose peripheral nerve injury and denervation (from 3 weeks post-injury)
- Monitor recovery and re-innervation serially over time
- Differentiate complete from partial denervation (the "kink" pattern)
- Guide therapeutic electrical stimulation parameters
- Prognosticate nerve recovery in peripheral nerve and root injuries
While modern EMG/NCS has largely taken over for precise neurophysiological diagnosis, the SD curve remains a valuable, low-cost, widely available bedside tool - especially in following the course of nerve recovery where the appearance of the kink and its gradual leftward shift gives early evidence of re-innervation that may precede clinical and EMG findings.
Sources:
- Campbell's Operative Orthopaedics, 15th ed. (2026), Electrical Stimulation section
- Medical Physiology (Boron & Boulpaep), p. 276, Figure 7-3
- Physiopedia: Strength-Duration Curve
- Akulwar-Tajane et al., "Exploring the Role of Strength-Duration Curve in Radiculopathy," EC Orthopaedics 14.9 (2023)