Anemia
Reading File
Asking for Preferences
Finding Sources
Searching PubMed
"iron deficiency anemia"[MeSH Terms] AND treatment
Reading File
Reading File
Searching PubMed
"iron deficiency" AND anemia AND management
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
I now have all the content needed to write a thorough, well-structured response on Iron Deficiency Anemia. Let me compose it.
Iron Deficiency Anemia (IDA)
Iron deficiency is the most common nutritional disorder in the world and the leading cause of anemia globally. It is particularly prevalent in toddlers, adolescent girls, women of childbearing age, and people in low-resource settings.
Normal Iron Metabolism
Understanding IDA starts with iron homeostasis:
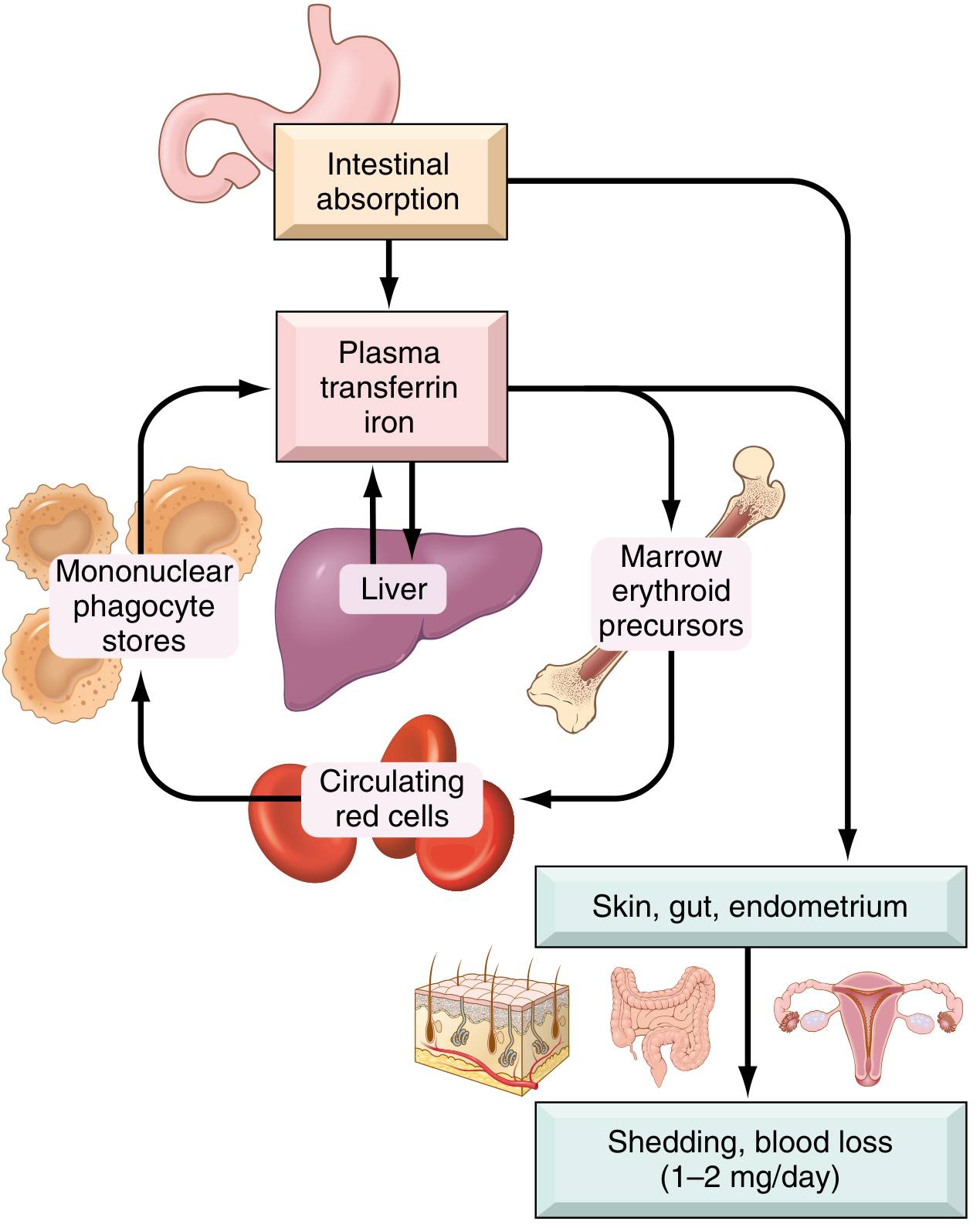
Key numbers:
| Parameter | Males | Females |
|---|---|---|
| Total body iron | ~3,450 mg | ~2,450 mg |
| Iron in hemoglobin | 2,100 mg | 1,750 mg |
| Storage iron (ferritin/hemosiderin) | 1,000 mg | 400 mg |
| Daily dietary requirement | 7-10 mg | 7-20 mg |
- Normal diet in the US contains 10-20 mg/day; ~20% of heme iron is absorbed vs. only 1-2% of nonheme iron.
- Iron is transported in plasma by transferrin (normally ~1/3 saturated, serum iron ~100-120 µg/dL).
- Hepcidin (liver-derived peptide) is the master regulator: it binds ferroportin on enterocytes and macrophages, promoting its degradation, thus reducing iron absorption and release. Low iron stores → low hepcidin → more absorption. Inflammation → high hepcidin → iron sequestration (basis of anemia of chronic disease).
Causes / Etiology
IDA develops from one of four mechanisms:
1. Dietary Lack
- Rare in high-resource countries (most dietary iron is heme-iron from meat)
- Common in infants (breast milk provides only ~0.3 mg/L iron), impoverished individuals, older adults with restricted diets, and vegans
2. Impaired Absorption
- Celiac disease, sprue, other malabsorption syndromes
- Post-gastrectomy (reduced acidity in proximal duodenum; faster transit)
- Dietary inhibitors: tannins (tea), carbonates, oxalates, phosphates
- Dietary enhancers: ascorbic acid, citric acid, amino acids
3. Increased Requirement
- Infants, children, and adolescents during growth spurts
- Pregnancy and menstruation
- Women in low-resource countries with multiple, closely-spaced pregnancies
4. Chronic Blood Loss (most common cause in developed countries)
- GI bleeding: peptic ulcer, colorectal cancer, angiodysplasia, hookworm
- Gynecologic: menorrhagia
- Urinary tract bleeding (less common)
- Iron deficiency in an adult male or postmenopausal female must be attributed to GI blood loss until proven otherwise - missing a GI cancer here can be a fatal error.
Stages of Iron Deficiency
Iron deficiency progresses through three sequential stages:
| Stage | Storage Iron | Serum Iron / Transferrin Sat | Hemoglobin / Hematocrit | Bone Marrow |
|---|---|---|---|---|
| Pre-latent (depletion) | ↓↓ | Normal | Normal | Absent stainable iron |
| Latent (iron-deficient erythropoiesis) | Absent | ↓ serum Fe; ↑ TIBC; Sat <15% | Normal | Erythroid hyperplasia |
| IDA (overt anemia) | Absent | ↓↓ serum Fe; ↓↓ ferritin; ↑ TIBC | ↓ Hgb + ↓ Hct | Hypochromic microcytic cells |
Morphology / Blood Smear

Bone marrow findings:
- Mild to moderate increase in erythroid progenitors
- Absent stainable iron in macrophages on Prussian blue stain - this is the gold standard diagnostic finding
Laboratory Findings
| Test | Finding in IDA |
|---|---|
| Hemoglobin / Hematocrit | ↓ |
| MCV | ↓ (microcytic) |
| MCH / MCHC | ↓ (hypochromic) |
| Serum iron | ↓ |
| Serum ferritin | ↓ (<12 µg/L) - most sensitive early marker |
| TIBC (transferrin) | ↑ |
| Transferrin saturation | ↓ (<15%) |
| Serum hepcidin | ↓ (reduced stores inhibit synthesis) |
| Blood smear | Microcytic, hypochromic; pencil cells |
| Reticulocyte count | Low (or normal) |
Note: Ferritin is an acute-phase reactant. In concurrent inflammation, ferritin can be falsely normal even with true iron deficiency (overlap with anemia of chronic disease).
Clinical Features
General anemia symptoms (non-specific):
- Fatigue, pallor, exertional dyspnea, palpitations, headache, dizziness
Features specific to severe / longstanding IDA (from iron depletion in non-hematopoietic tissues):
- Koilonychia - spoon-shaped nails
- Alopecia - hair loss
- Atrophic glossitis - smooth, sore tongue
- Angular cheilitis - cracking at corners of mouth
- Pica - craving for non-food items (clay, ice = pagophagia, flour)
- Plummer-Vinson syndrome (rare triad): microcytic hypochromic anemia + atrophic glossitis + esophageal webs
- Gastric mucosal atrophy; intestinal malabsorption
Investigation Approach
For adult men and postmenopausal women with IDA, GI evaluation is mandatory:
- Colonoscopy first (most common source is colorectal carcinoma or angiodysplasia)
- Upper endoscopy + push enteroscopy if colonoscopy negative
- Duodenal biopsy to exclude celiac disease
- Treat H. pylori if found (decreases iron absorption; causes microerosions)
- Capsule endoscopy if all three above are unrevealing
- If capsule study negative → investigate non-GI causes
(Goldman-Cecil Medicine, Chapter 145)
Treatment
Oral Iron
- First-line for most patients
- Ferrous sulfate 325 mg (65 mg elemental iron) three times daily
- Reticulocyte count rises in 5-7 days after starting iron
- Hemoglobin normalizes over weeks; continue for 3-6 months after normalization to replenish stores
- Side effects: constipation, nausea, dark stools (reduce adherence)
- Take on empty stomach for better absorption; ascorbic acid helps; avoid antacids, tea, dairy within 1-2 hours
IV Iron
- Indicated when oral iron is not tolerated, malabsorption is present, ongoing blood loss exceeds oral replacement capacity, or rapid repletion is needed (perioperative, heart failure, IBD)
- Agents: ferric carboxymaltose, iron sucrose, ferumoxytol, low-molecular-weight iron dextran
Treat the Underlying Cause
- This is as important as iron replacement. IDA that is not explained must prompt a search for occult GI malignancy.
IDA vs. Anemia of Chronic Disease (ACD) - Key Distinction
| Feature | IDA | ACD |
|---|---|---|
| Serum iron | ↓ | ↓ |
| TIBC | ↑ | ↓ or normal |
| Ferritin | ↓ | Normal or ↑ |
| Hepcidin | ↓ | ↑ |
| Marrow iron | Absent | Present (increased) |
Recent Evidence (2024-2025)
The AGA Clinical Practice Update on IDA (2024) provides updated guidance on GI workup. A 2025 Lancet Haematology consensus statement by Benson et al. addresses evidence-based management across children, adults, and pregnant individuals - including updated IV iron indications and dosing.
Sources:
- Robbins, Cotran & Kumar Pathologic Basis of Disease, pp. 612-615
- Goldman-Cecil Medicine, Chapter 145
- DeLoughery TG et al. AGA Clinical Practice Update on IDA, 2024. Clin Gastroenterol Hepatol.
- Benson AE et al. Management of iron deficiency, Lancet Haematol 2025.
This is a shared conversation. Sign in to Orris to start your own chat.