ANS – Sympathetic vs Parasympathetic Sleep (REM vs NREM) EEG waves CSF formation & circulation Hypothalamus functions Pituitary gland Thyroid hormones Insulin & glucagon Adrenal cortex hormones Calcium homeostasis (PTH, Calcitonin, Vitamin D) Calcium (imp) EEG Sleep Thyroid (imp)
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have rich source material for all topics. Let me now compose the complete, comprehensive study notes.
Physiology Study Notes - Complete Review
1. ANS - Sympathetic vs Parasympathetic
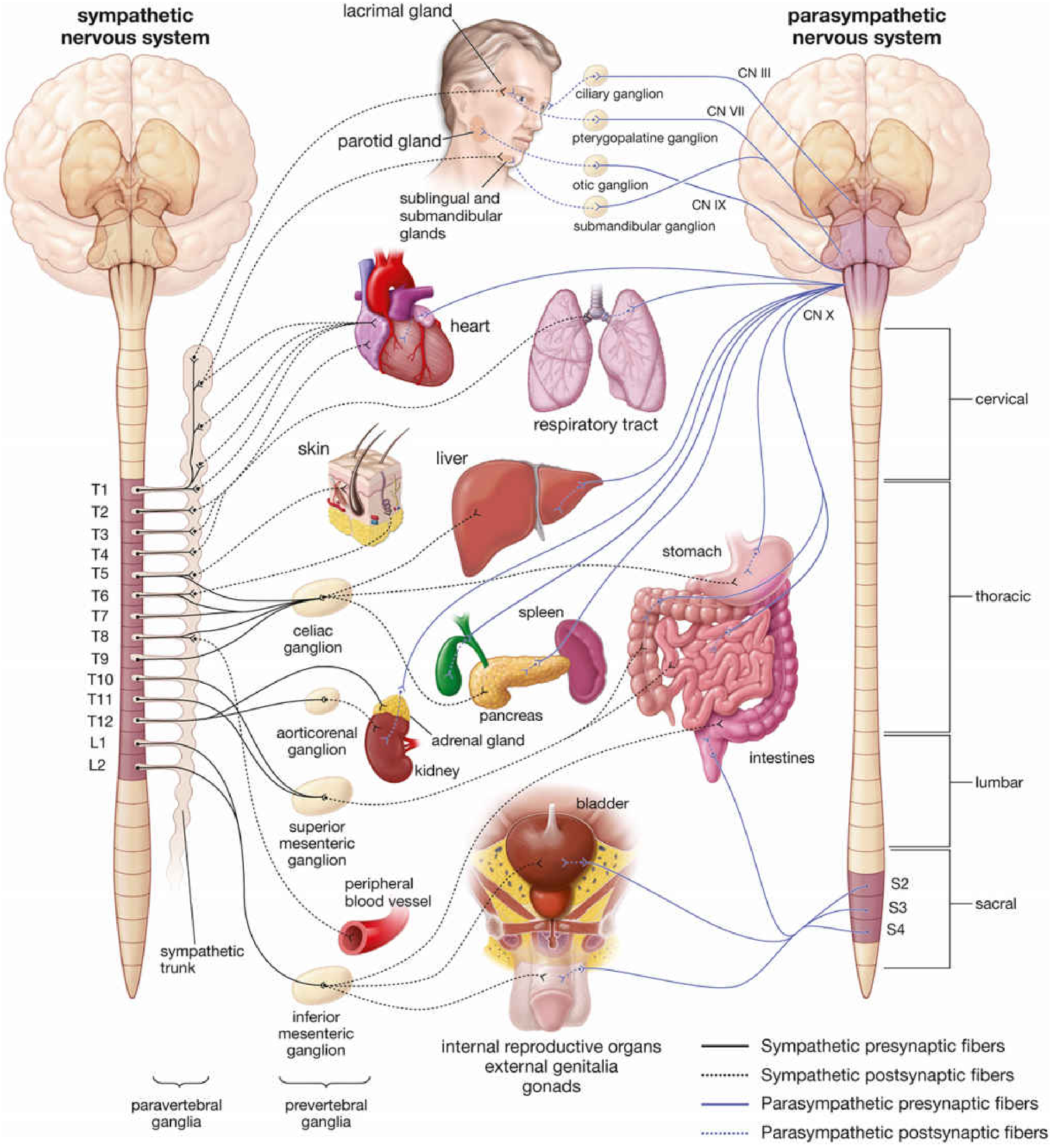
Origin (Outflow)
| Feature | Sympathetic | Parasympathetic |
|---|---|---|
| Outflow | Thoracolumbar (T1-L2) | Craniosacral (CN III, VII, IX, X + S2-S4) |
| Preganglionic fiber | Short | Long |
| Postganglionic fiber | Long | Short |
| Ganglion location | Paravertebral / prevertebral (far from organ) | Terminal ganglia (in/near organ wall) |
| Neurotransmitter (pre) | ACh (nicotinic) | ACh (nicotinic) |
| Neurotransmitter (post) | NE (adrenergic) | ACh (muscarinic) |
Exception: Adrenal medulla gets direct preganglionic sympathetic fibers (no postganglionic neuron); releases EPI + NE directly into blood.
Functional Effects (Organ by Organ)
| Organ | Sympathetic ("fight or flight") | Parasympathetic ("rest & digest") |
|---|---|---|
| Heart rate | Increases (β1) | Decreases (M2) |
| Contractility | Increases (β1) | Slight decrease |
| Bronchi | Dilates (β2) | Constricts |
| GI motility | Decreases (α2, β2) | Increases |
| GI sphincters | Contracts (closes) | Relaxes |
| Pupils | Dilates - mydriasis (α1) | Constricts - miosis (M3) |
| Salivary glands | Thick, viscous saliva (α1) | Watery, profuse saliva |
| Bladder detrusor | Relaxes (β2) | Contracts (M3) |
| Bladder sphincter | Contracts (α1) | Relaxes |
| Blood vessels (skin, viscera) | Constricts (α1) | Minimal direct effect |
| Sweat glands | Activates (cholinergic sympathetic - muscarinic) | - |
| Adrenal medulla | EPI/NE secretion | - |
| Liver | Glycogenolysis (β2, α1) | - |
| Eye (ciliary muscle) | Relaxes (β2) - far vision | Contracts (M3) - near vision |
Key receptors: α1 (vasoconstriction, pupil dilation), α2 (presynaptic inhibition), β1 (heart), β2 (bronchi, blood vessels), M2 (heart), M3 (smooth muscle, glands).
- Histology: A Text and Atlas, p. 988-989
2. Sleep - REM vs NREM
NREM Sleep (Non-Rapid Eye Movement)
NREM has 4 stages (or 3 in newer classification merging stages 3+4):
| Stage | EEG | Features |
|---|---|---|
| N1 (Stage 1) | Theta waves (4-7 Hz) | Lightest sleep; hypnic jerks; easily awakened |
| N2 (Stage 2) | Sleep spindles (8-14 Hz) + K complexes | True sleep begins; ~50% of total sleep |
| N3 (Stage 3) | Delta waves (<4 Hz, >20%) | Slow-wave sleep (SWS) / deep sleep |
| N4 (Stage 4) | Delta waves (>50%) | Deepest; GH release; sleepwalking/night terrors |
(Note: Modern AASM classification merges N3+N4 into a single N3 stage)
REM Sleep (Rapid Eye Movement)
- EEG resembles waking state - low voltage, high frequency (beta-like, "desynchronized")
- Rapid eye movements, muscle atonia (paralysis of voluntary muscles via glycine/GABA inhibition)
- Most vivid dreaming occurs here
- Occurs in cycles of ~90 minutes; first REM period is short (~10 min), lengthens toward morning
- Penile/clitoral tumescence (physiological)
- Increased brain O2 consumption
Sleep Architecture
- Total sleep time: ~7-9 hours in adults
- Cycles: 4-6 per night, each ~90 minutes
- Early night: More NREM (deep, slow-wave)
- Late night: More REM
- REM deprivation → REM rebound on recovery nights
Key Neurochemistry
| State | Dominant neurotransmitters |
|---|---|
| Wake | ACh (high), NE (high), Serotonin (high), Histamine (high) |
| NREM | All aminergic systems decrease; GABA increases |
| REM | ACh (high - REM-on); NE + Serotonin virtually silent (REM-off) |
- Adenosine builds up during wakefulness → sleep pressure (caffeine blocks adenosine receptors)
- SCN (suprachiasmatic nucleus) controls circadian rhythm; melatonin from pineal gland promotes sleep onset
3. EEG Waves ⭐ (Important)
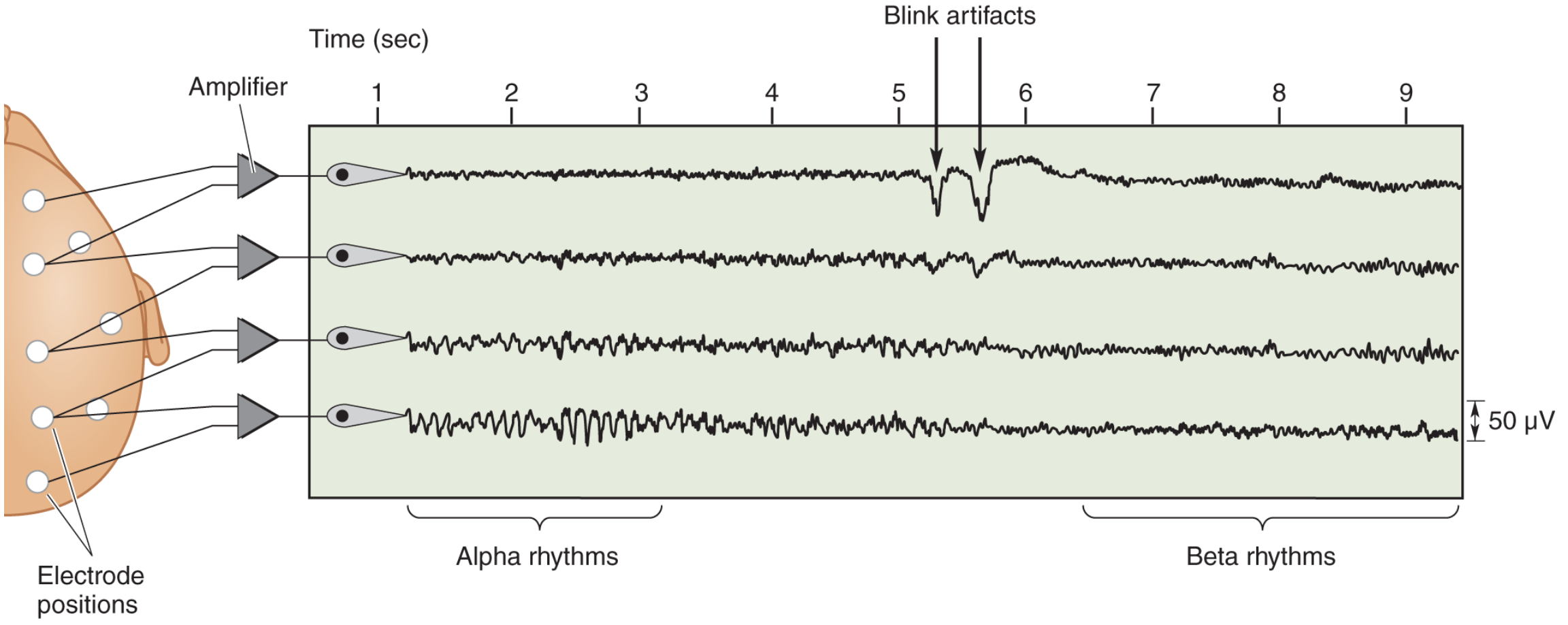
A normal EEG. First seconds show alpha activity (8-13 Hz), largest occipital. At the arrows, subject opened eyes - alpha suppressed, replaced by faster beta rhythms.
EEG Wave Summary Table
| Wave | Frequency | Amplitude | State/Association |
|---|---|---|---|
| Delta (δ) | < 4 Hz | High | Deep NREM sleep (N3/N4); coma; infants; abnormal in awake adults |
| Theta (θ) | 4-7 Hz | Medium | Light sleep (N1); drowsiness; emotional states; normal in children |
| Alpha (α) | 8-13 Hz | Medium | Relaxed, awake, eyes closed; largest over occipital cortex; disappears on eye opening |
| Mu (μ) | 8-13 Hz | Medium | Similar to alpha; over motor/somatosensory cortex; disappears with motor activity |
| Beta (β) | 15-30 Hz | Low | Alert/active thinking; eye opening; mental activity; benzodiazepines increase beta |
| Gamma (γ) | 30-90 Hz | Very low | Activated, attentive cortex; perception binding; cognitive processing |
Sleep-Specific EEG Features
| Feature | Frequency | Stage |
|---|---|---|
| Sleep spindles | 8-14 Hz (brief bursts) | N2 (hallmark of N2) |
| K complexes | Nonrhythmic sharp wave + slow wave | N2 (often precedes spindles) |
| Delta waves | <4 Hz (large amplitude) | N3/N4 (slow-wave sleep) |
| Ripples | 80-200 Hz (brief) | Sleep (memory consolidation) |
Clinical Correlates
- 3 Hz spike-and-wave: Absence seizures
- Triphasic waves: Hepatic encephalopathy
- Burst suppression: Deep anesthesia / severe anoxic injury
- Isoelectric (flat) EEG: Brain death criterion
- Alpha coma: Eyes-open coma (poor prognosis)
- Benzodiazepines → increase beta activity
- Barbiturates → increase beta at low doses, burst suppression at high doses
Source: Neuroscience: Exploring the Brain, 5th Ed., p. 1710-1712
4. CSF Formation & Circulation
Formation
- Produced mainly by choroid plexus (lateral, 3rd, 4th ventricles) - ~500 mL/day
- Total volume in CNS: ~150 mL (turns over ~3x/day)
- Mechanism: Active secretion (Na+/K+ ATPase driven) + ultrafiltration of plasma
- Composition: Clear, colorless; low protein (~15-45 mg/dL), glucose ~60% of serum, no cells normally
Circulation Pathway
Lateral ventricles → Foramen of Monro → 3rd ventricle → Cerebral aqueduct (of Sylvius) → 4th ventricle → Foramina of Magendie (median) + Luschka (lateral) → Subarachnoid space → Arachnoid granulations → Superior sagittal sinus → Venous blood
Memory aid: "Monro-Sylvius-Magendie-Luschka"
Absorption
- Primarily via arachnoid granulations (villi) into dural venous sinuses
- Pressure-dependent, unidirectional flow
Clinical Points
- Hydrocephalus: Obstruction of flow (communicating vs non-communicating)
- Normal pressure hydrocephalus: Triad - gait apraxia, dementia, urinary incontinence ("wet, wobbly, wacky")
- Lumbar puncture at L3-L4 or L4-L5 (below spinal cord termination at L1-L2)
5. Hypothalamus Functions
The hypothalamus integrates the neuroendocrine, autonomic, and behavioral systems.
Releasing/Inhibiting Hormones (for Anterior Pituitary)
| Hypothalamic Hormone | Effect on Ant. Pituitary |
|---|---|
| TRH | Releases TSH, Prolactin |
| CRH | Releases ACTH |
| GnRH | Releases LH, FSH |
| GHRH | Releases GH |
| Somatostatin (SS) | Inhibits GH, TSH |
| Dopamine (PIH) | Inhibits Prolactin |
Other Functions
| Function | Region |
|---|---|
| Temperature regulation | Anterior hypothalamus (cooling); Posterior (heat conservation) |
| Thirst / osmolarity | Osmoreceptors → ADH release (posterior pituitary) |
| Hunger/Satiety | Lateral (hunger); Ventromedial (satiety - "satiety center") |
| Circadian rhythm | Suprachiasmatic nucleus (SCN) |
| Autonomic control | Posterior = sympathetic; Anterior = parasympathetic |
| Emotion/aggression | Limbic connections |
| Sleep-wake | Lateral hypothalamus (orexin/hypocretin - wakefulness) |
| Posterior pituitary hormones | Synthesizes ADH (vasopressin) and Oxytocin (released from posterior pituitary) |
Memory aid: "TRH CRH GnRH GHRH SS DA"
6. Pituitary Gland
Anterior Pituitary (Adenohypophysis)
Derived from Rathke's pouch (oral ectoderm). Regulated by hypothalamic portal system.
| Hormone | Cell Type | Primary Target | Key Effects |
|---|---|---|---|
| GH | Somatotrophs (most numerous) | Liver → IGF-1 | Growth, lipolysis, anti-insulin |
| TSH | Thyrotrophs | Thyroid | T3/T4 synthesis & release |
| ACTH | Corticotrophs | Adrenal cortex | Cortisol, androgens |
| LH | Gonadotrophs | Gonads | Ovulation (F); testosterone (M) |
| FSH | Gonadotrophs | Gonads | Follicle growth (F); spermatogenesis (M) |
| Prolactin | Lactotrophs | Breast | Lactation; inhibits GnRH |
| MSH | Melanotrophs | Melanocytes | Pigmentation |
Posterior Pituitary (Neurohypophysis)
Derived from neural ectoderm (diencephalon). Stores and releases hormones synthesized in hypothalamus.
| Hormone | Synthesized in | Effect |
|---|---|---|
| ADH (Vasopressin) | Supraoptic nucleus | Water reabsorption (collecting duct V2R), vasoconstriction (V1R) |
| Oxytocin | Paraventricular nucleus | Uterine contraction, milk ejection, social bonding |
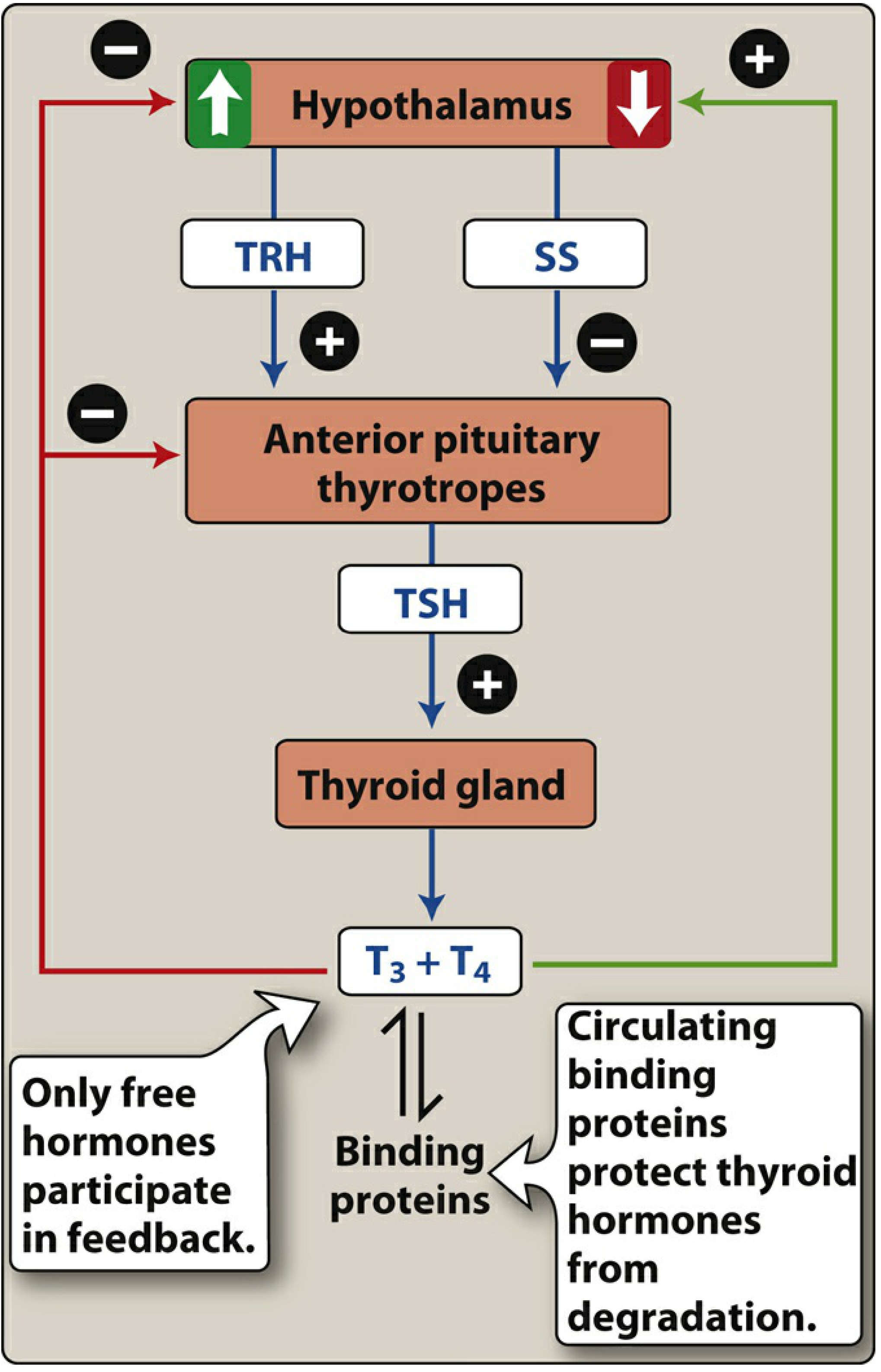
7. Thyroid Hormones ⭐ (Important)
Synthesis Steps (in thyroid follicle)
- Iodide (I-) uptake - Na+/I- symporter (NIS) on basolateral membrane - stimulated by TSH
- Oxidation: I- → I2 by thyroid peroxidase (TPO) (requires H2O2)
- Organification: Iodination of tyrosine residues on thyroglobulin → MIT (monoiodotyrosine) + DIT (diiodotyrosine)
- Coupling (by TPO):
- MIT + DIT → T3 (triiodothyronine, more active)
- DIT + DIT → T4 (thyroxine, prohormone)
- Storage: As thyroglobulin in follicular lumen (colloid) - the body's largest hormone store
- Release: TSH stimulates proteolysis of thyroglobulin → T3 + T4 secreted
- T4 → T3 conversion in periphery by deiodinase (T3 is 4x more potent)
Antibodies in Hashimoto thyroiditis: Anti-TPO antibodies (diagnostic)
Transport in Blood
- ~99.97% bound to Thyroxine-Binding Globulin (TBG), albumin, transthyretin
- Only free hormone is active and participates in feedback
- T4 half-life: ~7 days; T3 half-life: ~1 day
Mechanism of Action
- Nuclear receptors → gene transcription
- T4 deiodinated to T3 inside cells (T3 is the active form)
- Increases basal metabolic rate, O2 consumption, mitochondriogenesis
- Permissive for catecholamine effects (upregulates β-receptors)
Physiological Effects
| System | Effect |
|---|---|
| Metabolism | ↑ BMR, ↑ O2 consumption, ↑ heat production |
| Cardiovascular | ↑ HR, ↑ CO, ↑ β-receptor sensitivity |
| Development | Essential for brain development (fetal) + linear growth |
| GI | ↑ Gut motility |
| Bone | ↑ Bone turnover |
| Glucose | ↑ Glucose absorption and glycogenolysis |
Hypothyroidism vs Hyperthyroidism
| Feature | Hypothyroidism | Hyperthyroidism |
|---|---|---|
| TSH | ↑ (primary) | ↓ |
| Metabolism | Slow - weight gain, cold intolerance | Fast - weight loss, heat intolerance |
| Heart | Bradycardia | Tachycardia, palpitations |
| GI | Constipation | Diarrhea |
| Skin | Dry, coarse, myxedema | Warm, moist, pretibial myxedema (Graves) |
| Cause | Hashimoto (anti-TPO, anti-Tg) | Graves (TSI/TSH-R antibodies) |
| Treatment | Levothyroxine (T4) | PTU, methimazole, β-blockers, RAI |
Drug Inhibitors of Thyroid Synthesis
- PTU, Methimazole: Block TPO (organification + coupling)
- PTU also: Blocks peripheral T4→T3 conversion
- High-dose iodide (Wolff-Chaikoff): Transiently inhibits organification
- Lithium: Inhibits thyroglobulin proteolysis → blocks T3/T4 release
Source: Lippincott Illustrated Reviews Pharmacology, p. 779-781
8. Insulin & Glucagon
Insulin
- Secreted by β-cells of islets of Langerhans
- Stimulated by: glucose, amino acids, GIP, GLP-1, vagal (ACh), β2-adrenergic
- Inhibited by: hypoglycemia, somatostatin, α2-adrenergic (sympathetic)
- Mechanism: Glucose → ↑ ATP/ADP → closes K+ channels → depolarization → Ca2+ influx → insulin exocytosis
Key Actions:
| Tissue | Effect |
|---|---|
| Liver | ↑ Glycogen synthesis, ↑ glycolysis, ↓ gluconeogenesis, ↑ lipogenesis |
| Muscle | ↑ Glucose uptake (GLUT4), ↑ glycogen synthesis, ↑ protein synthesis |
| Adipose | ↑ Glucose uptake (GLUT4), ↑ lipogenesis, ↓ lipolysis |
| General | ↓ Blood glucose, ↑ K+ uptake into cells |
GLUT transporters: GLUT4 is insulin-dependent (muscle, fat). GLUT2 is in liver/pancreas (high capacity, low affinity). GLUT1 is constitutive (brain, RBCs).
Glucagon
- Secreted by α-cells
- Stimulated by: hypoglycemia, amino acids (especially alanine), stress, sympathetic stimulation
- Inhibited by: glucose, insulin, somatostatin
Key Actions:
| Tissue | Effect |
|---|---|
| Liver (primary target) | ↑ Glycogenolysis, ↑ gluconeogenesis, ↑ ketogenesis |
| Adipose | ↑ Lipolysis (↑ FFA for ketogenesis) |
- Acts via Gs → adenylyl cyclase → ↑ cAMP → PKA
- Counter-regulatory hormones: Glucagon, cortisol, epinephrine, GH (all raise blood glucose)
9. Adrenal Cortex Hormones
Three zones - mnemonic: "GFR" = Salt (mineralocorticoids), Sugar (glucocorticoids), Sex (androgens)
| Zone | Hormone | Regulator | Key Actions |
|---|---|---|---|
| Zona Glomerulosa (outer) | Aldosterone | Renin-Angiotensin, ↑ K+ | Na+ retention, K+ excretion, H+ excretion (collecting duct) |
| Zona Fasciculata (middle) | Cortisol | ACTH (CRH) | Anti-inflammatory, gluconeogenesis, protein catabolism, immunosuppression |
| Zona Reticularis (inner) | DHEA, androgens | ACTH | Weak androgens; pubic/axillary hair |
Cortisol Actions (Glucocorticoid)
- ↑ Blood glucose (gluconeogenesis, protein catabolism → amino acids)
- ↑ Lipolysis (central obesity with Cushing)
- Anti-inflammatory: ↓ PLA2 → ↓ arachidonic acid → ↓ prostaglandins + leukotrienes
- Immunosuppressive: ↓ T-cells, ↓ cytokines
- ↑ BP (permissive for catecholamines; some mineralocorticoid activity)
- Inhibits bone formation
Aldosterone
- Primary stimulus: Angiotensin II (via RAAS), hyperkalemia
- Acts on principal cells of collecting duct → ↑ ENaC expression → Na+ reabsorption → water follows → volume expansion
- Also ↑ H+ secretion by intercalated cells → metabolic alkalosis in excess
10. Calcium Homeostasis ⭐ (Important)
Normal serum calcium: 8.5-10.5 mg/dL (ionized: 4.5-5.6 mg/dL)
Three regulators: PTH, Calcitonin, Vitamin D
Parathyroid Hormone (PTH)
- From chief cells of parathyroid glands
- Stimulated by: ↓ Ca2+, ↓ Mg2+, ↓ Vitamin D
- Inhibited by: ↑ Ca2+ (via CaSR - calcium sensing receptor)
Actions (remember: PTH raises Ca, lowers Phos)
| Organ | PTH Effect |
|---|---|
| Bone | ↑ Osteoclast activity (via osteoblast RANK-L) → Ca2+ + Phosphate released |
| Kidney (PCT) | ↑ Ca2+ reabsorption; ↑ Phosphate excretion (phosphaturic); ↑ 1α-hydroxylase → ↑ Vitamin D activation |
| Kidney (DCT) | ↑ Ca2+ reabsorption |
| GI (indirect) | Via Vitamin D → ↑ Ca2+ absorption |
Net effect: ↑ serum Ca2+, ↓ serum Phosphate
Vitamin D (Calcitriol - 1,25-dihydroxycholecalciferol)
Activation pathway:
- Skin: 7-dehydrocholesterol + UV → Cholecalciferol (D3)
- Liver: D3 → 25-hydroxyvitamin D (storage form; measured clinically)
- Kidney: 25-OH-D → 1,25(OH)2D (calcitriol - active) via 1α-hydroxylase (stimulated by PTH, ↓ Ca2+, ↓ PO4)
Actions:
- ↑ Intestinal Ca2+ + phosphate absorption (via calbindin)
- ↑ Renal Ca2+ + phosphate reabsorption
- ↑ Bone mineralization (at normal Ca levels); can stimulate osteoclasts in excess
- Net: ↑ Ca2+, ↑ Phosphate (both)
Calcitonin
- From parafollicular C-cells of thyroid
- Stimulated by: ↑ Ca2+
- Actions (opposes PTH):
- Inhibits osteoclasts → ↓ bone resorption
- ↑ Renal Ca2+ + phosphate excretion
- Net: ↓ serum Ca2+
- Physiological role is minor in adults; more important in children and during pregnancy/lactation
- Clinical use: Paget's disease, hypercalcemia (short-term)
Summary Table
| PTH | Vitamin D (calcitriol) | Calcitonin | |
|---|---|---|---|
| Source | Parathyroid | Kidney (activated) | Thyroid C-cells |
| Stimulus | ↓ Ca2+ | ↓ Ca2+, PTH | ↑ Ca2+ |
| Serum Ca2+ | ↑ | ↑ | ↓ |
| Serum Phosphate | ↓ | ↑ | ↓ |
| Bone | Resorption ↑ | Mineralization ↑ | Resorption ↓ |
| GI absorption | ↑ (indirect) | ↑ (direct) | No effect |
Clinical Points
| Condition | Ca2+ | PO4 | PTH | Notes |
|---|---|---|---|---|
| Primary hyperPTH | ↑ | ↓ | ↑ | Kidney stones, bones, groans, psychic moans |
| Hypo PTH | ↓ | ↑ | ↓ | Tetany, Chvostek, Trousseau, prolonged QT |
| Vit D deficiency | ↓ (or N) | ↓ | ↑ (secondary) | Rickets (children), Osteomalacia (adults) |
| Malignancy | ↑ | Variable | ↓ | PTHrP or osteolytic mets |
| Sarcoidosis | ↑ | ↑ | ↓ | Macrophages produce 1α-hydroxylase |
| Hypercalcemia Tx | - | - | - | IV fluids, furosemide, bisphosphonates, calcitonin |
Tetany features:
- Chvostek sign: Tap facial nerve → facial twitch
- Trousseau sign: Inflate BP cuff → carpal spasm
Sources: Neuroscience: Exploring the Brain 5th Ed. | Lippincott Illustrated Reviews Pharmacology | Histology: A Text and Atlas | Medical Physiology (Boron & Boulpaep)
This is a shared conversation. Sign in to Orris to start your own chat.