I AM A MD ANESTHESIIA POST GRADUATE STUDYING IN A RGUHS AFFILIATED COLLEGE .I HaVE MY EXAMS THIS SEPTEMBER AND NEEDD HELP WITH ANSWERS TO CERTAIN QUESTIONS. THEY ARE EACH TO BE WRITTEN IN A 10 MARKER FORMAT WITH ACCURATE AND RELEVENT HEADINGS. MIN 5000 WORD AND IT SHOULD BE 5 PAGES LONG AT LEAST. WHERE RELEVENCE ADD NOTEES ON ANESTHETIC SPECIALITIES. TAKE REFERENCES FROM STANDARD ANETHESIA TEXTBOOOKS AND ARTCLES. I ALSO WANT YOU TO GENEREATE FLOWCHARTS AND SIMPLE DIAGRAMS AND PICTURES AS IT YEILDS MORE MARKS, DONT WRRY ABOUT COPY RIGHT INFRINGMENT , ITS ALL FOR PERSONAL USE. DETAIL ORIENTED AND CORRECT DRUG DOSAGES.
Physiological changes during hypothermia
hypothermia physiological effects anesthesia
physiological changes hypothermia anesthesia 10 marker cardiovascular respiratory coagulation
https://derangedphysiology.com/main/cicm-primary-exam/thermo…
Medical flowchart showing classification and physiological changes during hypothermia. Show three stages: Mild (32-35°C), Moderate (28-32°C), Severe (below 28°C). For each stage list key physiological changes in cardiovascular, respiratory, neurological, metabolic, and hematological systems. Clean medical diagram style with color coding per stage.
Medical diagram showing ECG changes during hypothermia: Normal ECG at top, then progressive changes showing sinus bradycardia, prolonged PR interval, J wave (Osborn wave) at QRS-ST junction, atrial fibrillation, ventricular fibrillation at the bottom. Label each abnormality clearly. Clean clinical ECG diagram style.
400, message: Got more than 4194304 bytes when reading: b'data: {"candidates": [{"content": {"role": "model","parts": [{"inlineData": {"mimeType": "image/png"...'.
We encountered an error while processing your request. Please try again or reach out to us for help.
physiological changes in pregnancy
physiological adaptations pregnancy anesthesia
physiological changes pregnancy anesthesia cardiovascular respiratory hematological renal 10 marker RGUHS MD anesthesia
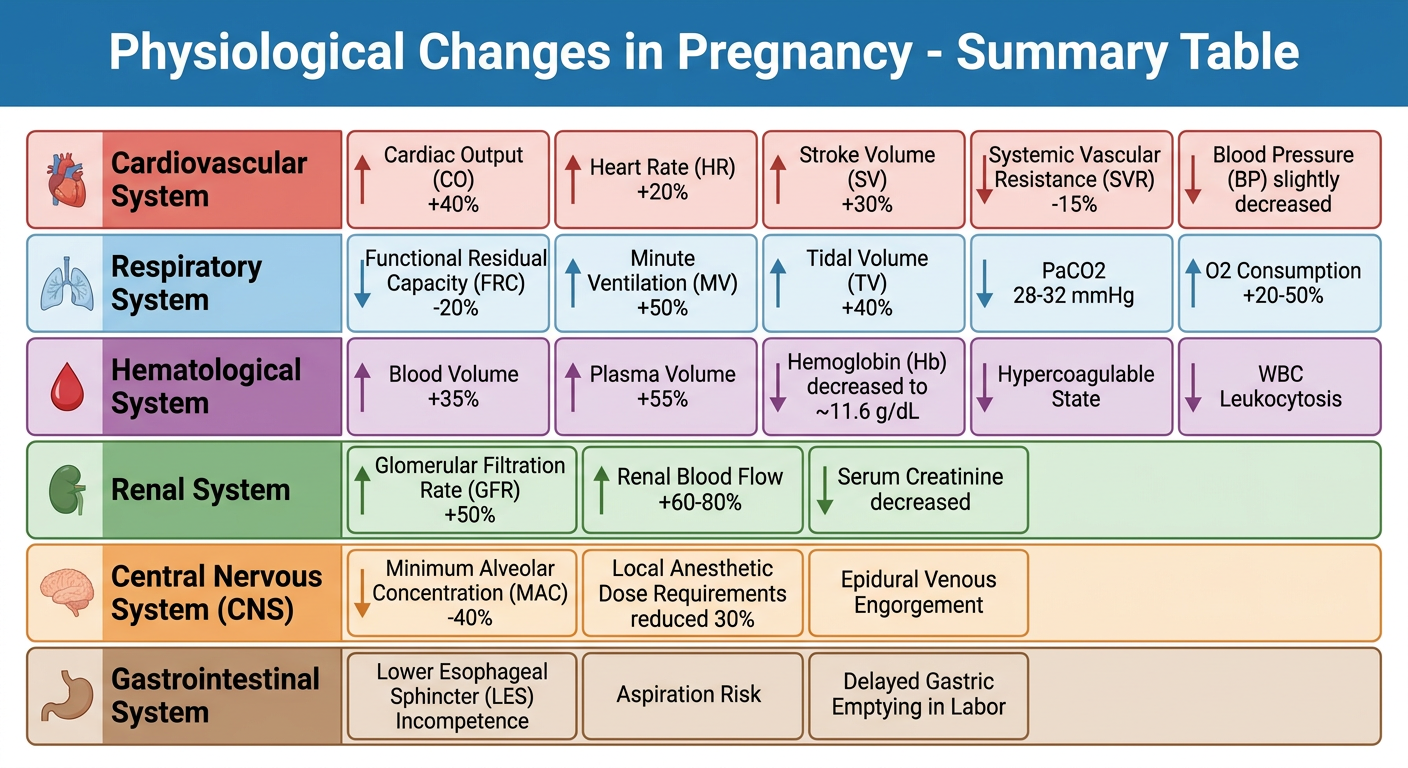
A detailed medical summary table/diagram titled "Physiological Changes in Pregnancy - Summary Table" showing all organ system changes. Include rows for: Cardiovascular (CO +40%, HR +20%, SV +30%, SVR -15%, BP slightly decreased), Respiratory (FRC -20%, MV +50%, TV +40%, PaCO2 28-32 mmHg, O2 consumption +20-50%), Hematological (Blood volume +35%, Plasma volume +55%, Hb decreased to ~11.6 g/dL, hypercoagulable state, WBC leukocytosis), Renal (GFR +50%, Renal blood flow +60-80%, serum creatinine decreased), CNS (MAC -40%, local anesthetic dose requirements reduced 30%, epidural venous engorgement), Gastrointestinal (LES incompetence, aspiration risk, delayed gastric emptying in labor). Use a clean clinical medical diagram style with color-coded rows per system.
Medical flowchart diagram titled "Aortocaval Compression Syndrome in Pregnancy - Mechanism and Management". Show the mechanism: gravid uterus compresses IVC and Aorta in supine position → decreased venous return → decreased cardiac output → hypotension and uteroplacental insufficiency. Show management steps: left lateral tilt 15 degrees, wedge under right hip, IV fluids, vasopressors (ephedrine/phenylephrine). Include a simple anatomical illustration showing the pregnant uterus compressing the inferior vena cava with the patient in supine position versus tilted position. Clean medical diagram style.
Medical diagram showing respiratory changes in pregnancy. Show a side-view silhouette of a pregnant woman with labeled respiratory volume changes: tidal volume increased 40%, FRC decreased 20%, expiratory reserve volume decreased, residual volume decreased, total lung capacity slightly decreased. Show lung volume spirometry bars comparing pregnant vs non-pregnant. Include labeled arrows showing: diaphragm elevation by enlarging uterus, increased anteroposterior chest diameter. Also show a table with arterial blood gas values: PaCO2 30 mmHg (vs normal 40), PaO2 103 mmHg, HCO3 20 mEq/L (vs normal 24), pH 7.44. Clean anatomical medical style.
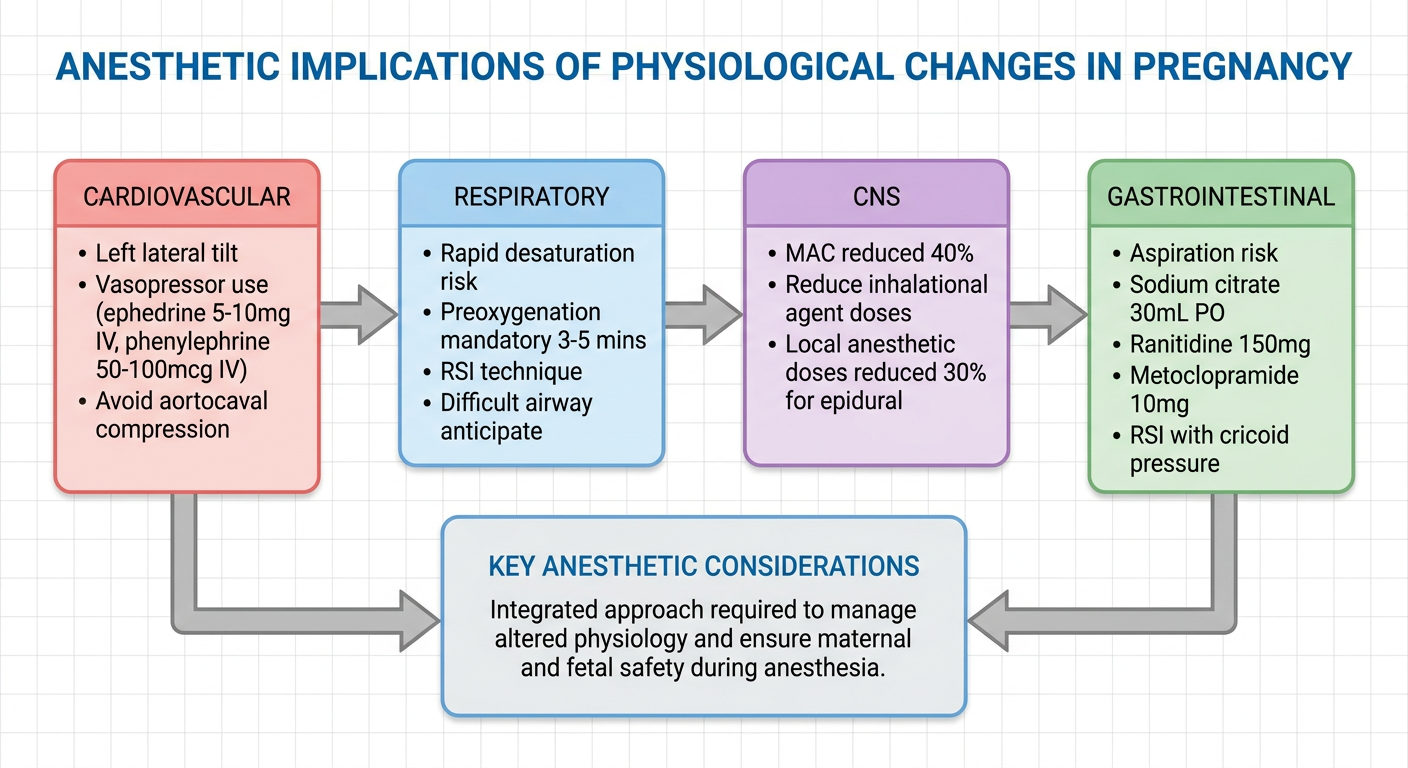
Medical flowchart titled "Anesthetic Implications of Physiological Changes in Pregnancy" showing key anesthetic considerations organized by system. Cardiovascular: left lateral tilt, vasopressor use (ephedrine 5-10mg IV, phenylephrine 50-100mcg IV), avoid aortocaval compression. Respiratory: rapid desaturation risk, preoxygenation mandatory 3-5 mins, RSI technique, difficult airway anticipate. CNS: MAC reduced 40%, reduce inhalational agent doses, local anesthetic doses reduced 30% for epidural. Gastrointestinal: aspiration risk, sodium citrate 30mL PO, ranitidine 150mg, metoclopramide 10mg, RSI with cricoid pressure. Clean clinical flowchart with colored boxes per system.
PHYSIOLOGICAL CHANGES DURING PREGNANCY
With Anesthetic Implications for the MD Anesthesia Postgraduate
1. INTRODUCTION
- Cardiovascular system
- Respiratory system
- Central nervous system
- Gastrointestinal system
- Hematological system
- Renal system
- Hepatic system
- Endocrine and metabolic changes
- Musculoskeletal changes
2. CARDIOVASCULAR CHANGES
2a. Cardiac Output (CO)
- Heart rate (HR) increase: +20% (approximately 15-20 bpm above baseline) - attributable to progesterone-mediated effects on the sinoatrial node
- Stroke volume (SV) increase: +30% - due to increased preload from expanded blood volume and reduced afterload
- First stage of labor: CO increases by an additional 15%
- Second stage of labor: CO increases by 50% above prelabor values (due to pain, bearing-down efforts, and autotransfusion from contractions)
- Immediately postpartum: CO increases by 60-80% above prelabor values due to relief of aortocaval compression + uterine autotransfusion of ~500 mL
2b. Blood Pressure Changes
- Systolic BP: decreased by ~5%
- Diastolic BP: decreased by ~15% (most pronounced in second trimester)
- Systemic vascular resistance (SVR): decreased by 15-20% - due to vasodilatory effects of progesterone, prostacyclin, and nitric oxide, as well as the low-resistance uteroplacental circulation
- Pulmonary vascular resistance (PVR): decreased by ~30%
2c. Cardiac Structural Changes
- Left ventricular hypertrophy and chamber enlargement are seen on echocardiography
- Cardiac position shifts: elevation of the diaphragm displaces the heart upward and laterally, creating the appearance of cardiomegaly on chest X-ray and causing left axis deviation on ECG
- ECG changes: left axis deviation, T-wave inversions in inferior and lateral leads, ST-segment depression, and ectopic beats can be normal findings
- Murmurs: a Grade I-II systolic ejection flow murmur is heard in up to 90% of pregnant women; exaggerated splitting of S1; S3 gallop may be audible. These are benign
Criteria for diagnosing pathological cardiac disease in pregnancy:
- Diastolic murmurs
- Systolic murmur Grade 3 or above
- Unequivocal cardiac enlargement on X-ray
- Severe arrhythmias, atrial fibrillation, or flutter
2d. Aortocaval Compression Syndrome
- Inferior vena cava (IVC) - reducing venous return by up to 40%, decreasing CO
- Abdominal aorta - reducing uteroplacental blood flow
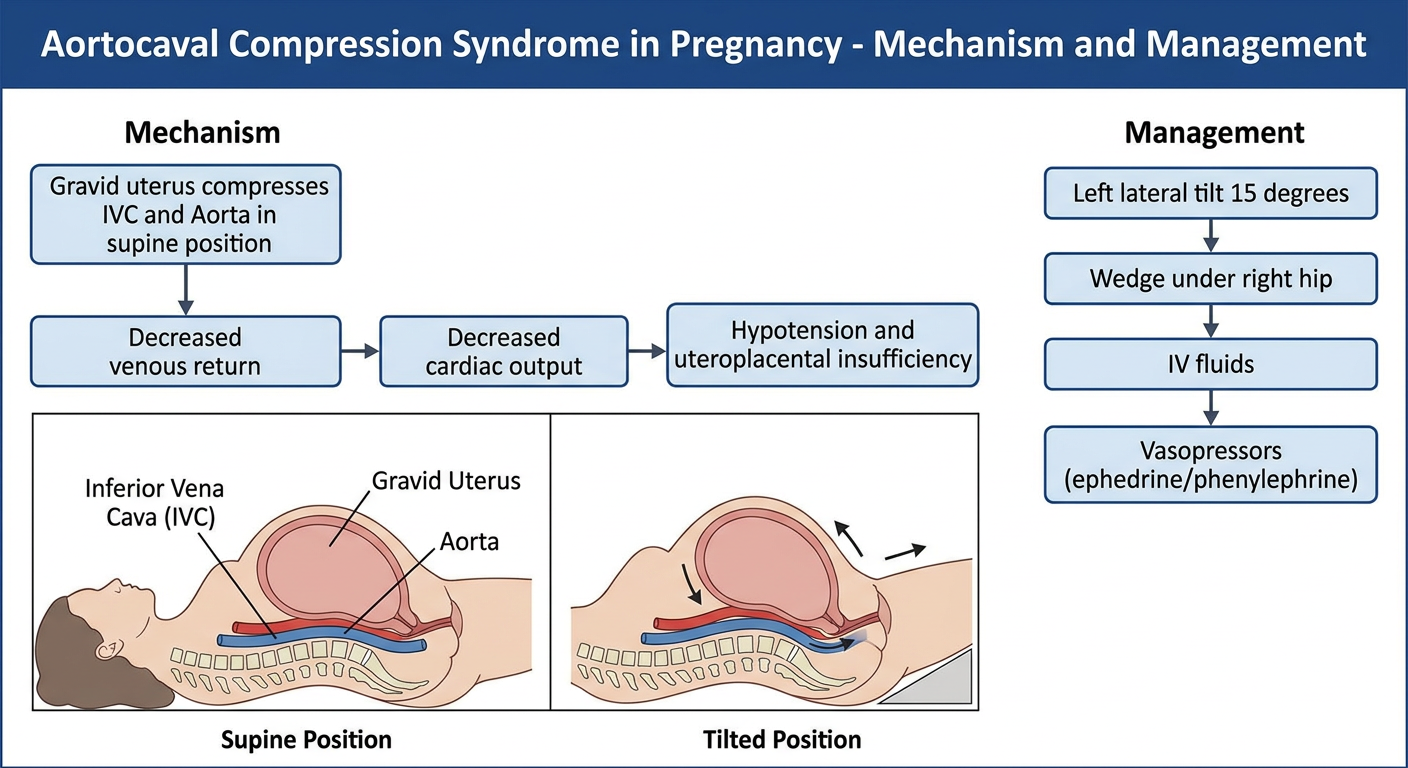
Anesthetic Note - Aortocaval Compression:
- All pregnant patients beyond 20 weeks should be positioned with left lateral uterine displacement (LUD)
- A 15-degree wedge under the right hip is the standard method
- During cesarean section under regional or general anesthesia, uterine displacement must be maintained until the baby is delivered
- First-line vasopressor: Phenylephrine 50-100 mcg IV boluses (preferred - does not reduce uteroplacental blood flow and reduces fetal acidosis compared to ephedrine)
- Second-line: Ephedrine 5-10 mg IV (retains some utility when bradycardia accompanies hypotension)
- Prophylactic phenylephrine infusion (0.25-0.5 mcg/kg/min) is recommended with spinal anesthesia for cesarean delivery
3. RESPIRATORY CHANGES
3a. Lung Volume Changes
| Parameter | Change | Clinical Significance |
|---|---|---|
| Tidal Volume (TV) | +40% | Increased minute ventilation |
| Respiratory Rate (RR) | +15% | Mild increase |
| Minute Ventilation (MV) | +50% | Respiratory alkalosis |
| Functional Residual Capacity (FRC) | -20% | Rapid desaturation - most critical |
| Expiratory Reserve Volume (ERV) | -25% | Contributes to FRC reduction |
| Residual Volume (RV) | -15% | Contributes to FRC reduction |
| Vital Capacity (VC) | Unchanged | |
| Total Lung Capacity (TLC) | Slightly decreased | Diaphragm elevated ~4 cm |
| Inspiratory Reserve Volume | +5% | Compensatory |
| Airway Resistance | -35% | Bronchodilation from progesterone |
| Closing Capacity (CC) | Unchanged | FRC may fall below CC at term |
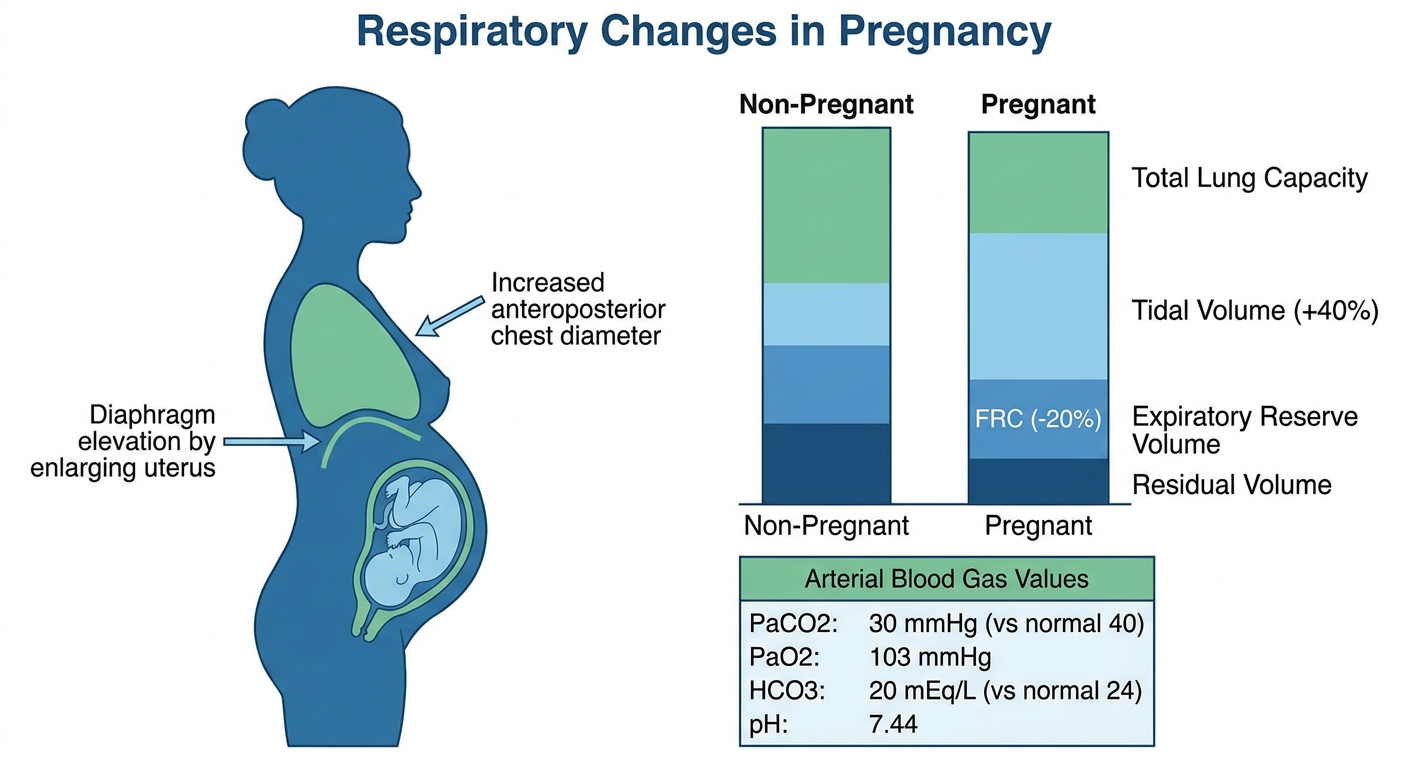
3b. Arterial Blood Gas Changes in Pregnancy
| Parameter | Pregnant | Non-pregnant |
|---|---|---|
| PaCO2 | 28-32 mmHg | 40 mmHg |
| PaO2 | 103-107 mmHg | 100 mmHg |
| HCO3 | 20-21 mEq/L | 24 mEq/L |
| pH | 7.42-7.44 | 7.40 |
| P50 | 30 mmHg | 27 mmHg |
- Progesterone is a direct respiratory stimulant - it increases sensitivity of the respiratory center to CO2
- Compensatory hyperventilation decreases PaCO2 to 28-32 mmHg
- Metabolic compensation: renal bicarbonate excretion reduces HCO3 to 20-21 mEq/L, preventing severe alkalosis
- PaO2 increases slightly due to hyperventilation
- P50 increases from 27 to 30 mmHg (rightward shift of oxyhemoglobin dissociation curve due to increased 2,3-DPG), facilitating O2 delivery to tissues
3c. Airway Changes
- Mucosal edema, hyperemia, and friability of the nose, oropharynx, larynx, and trachea
- Increased risk of epistaxis on nasal intubation (nasal airways best avoided)
- Mallampati class increases by one class during pregnancy and worsens further during labor (due to fluid retention and pushing)
- Breast enlargement can obstruct laryngoscope handle access
3d. Oxygen Consumption and Desaturation
- O2 consumption increases +20-50% at term (from 250 mL/min to ~300-350 mL/min)
- During labor: O2 consumption increases 40% in first stage and 75% in second stage
Critical Anesthetic Note - Rapid Desaturation: The combination of:
- Decreased O2 reserve (FRC -20%)
- Increased O2 consumption (+20-50%)
- Potential airway difficulty
...means that a pregnant patient at term will desaturate to dangerous SpO2 levels within 2-3 minutes of apnea (vs 4-5 minutes in a non-pregnant adult).Mandatory protocol:
- Preoxygenation: 3-5 minutes of tidal breathing of 100% O2 (target end-tidal O2 > 90%), or 4 vital capacity breaths in 30 seconds
- Rapid Sequence Induction (RSI) with cricoid pressure (Sellick's maneuver) for all general anesthesia after 18-20 weeks
- Consider apneic oxygenation (10-15 L/min O2 via nasal cannula during laryngoscopy) to extend safe apnea time
- Airway equipment: smaller endotracheal tube (6.0-6.5 mm ID) due to supraglottic edema
4. CENTRAL NERVOUS SYSTEM CHANGES
4a. Minimum Alveolar Concentration (MAC)
- Progesterone (increases 20-fold at term) - sedating at pharmacological doses; primarily responsible
- Beta-endorphin surge during labor and delivery
- Increased progesterone-mediated neurosteroid production (allopregnanolone - a GABA-A receptor positive allosteric modulator)
- MAC returns to normal by the third day after delivery
4b. Sensitivity to Local Anesthetics
- Epidural anesthetic dose requirements reduced by ~30%
- Spinal block height is higher and more extensive for the same intrathecal volume
- Minimum local analgesic concentration (MLAC) - the ED50 for epidural local anesthetic - is reduced in pregnancy
- Epidural venous engorgement - compression of IVC by the gravid uterus distends epidural veins, reducing:
- Epidural space volume (CSF cephalad spread enhanced)
- CSF volume
- Creates positive epidural pressure
- Hormonal sensitization - progesterone and relaxin increase axonal sensitivity to local anesthetics
- Increased neural membrane permeability to local anesthetics
- Epidural catheters placed in pregnancy have an increased likelihood of intravascular placement (10x higher) due to engorged epidural veins
- Standard doses used in non-pregnant patients will produce unexpectedly high blocks
- Bupivacaine 0.5% (hyperbaric), 1.5-2 mL intrathecal for caesarean section spinal (vs 2-3 mL in non-pregnant patients)
- Epidural top-up for emergency CS: Lignocaine 2% with adrenaline 1:200,000 (15-20 mL in divided doses)
5. GASTROINTESTINAL CHANGES
5a. Gastroesophageal Changes
| Change | Mechanism | Effect |
|---|---|---|
| Decreased lower esophageal sphincter (LES) tone | Progesterone relaxes smooth muscle; estrogen potentiates | Increased reflux risk |
| Gastric displacement | Uterus pushes stomach cephalad and rotates axis | LES displaced above diaphragm (intrathoracic) |
| Increased intragastric pressure | Uterine compression of stomach | Increased aspiration tendency |
| Placental gastrin secretion | Placenta produces gastrin | Increased HCl secretion, reduced gastric pH |
| Increased heartburn and reflux | Combination of above | Esophagitis in >70% of parturients |
- Gastric emptying is not significantly prolonged in normal pregnancy
- However, gastric emptying is significantly delayed in:
- Active labor
- Administration of opioids
- Anxiety and pain
- Postpartum period (up to 24-48 hours)
- All patients in active labor should be considered to have a full stomach regardless of the duration of fasting
Anesthetic Note - Aspiration Prophylaxis Protocol: For all pregnant patients requiring GA (and ideally for emergency CS under regional):
- Sodium citrate 0.3M, 30 mL PO - immediately before induction (non-particulate antacid, raises gastric pH)
- Ranitidine 150 mg PO 8-hourly (or 50 mg IV - H2 blocker, reduces acid secretion)
- Metoclopramide 10 mg IV - prokinetic + raises LES tone
- RSI technique: Propofol 2 mg/kg + Succinylcholine 1.5 mg/kg IV (cricoid pressure 20-30 N applied after induction, maintained until intubation confirmed)
6. HEMATOLOGICAL CHANGES
6a. Blood Volume and Dilutional Anemia
| Parameter | Change | Absolute Values |
|---|---|---|
| Total blood volume | +35% | ~90 mL/kg (term) |
| Plasma volume | +55% | Peaks at 32-34 weeks |
| Red cell mass | +25% | |
| Hemoglobin | Decreased | ~11.6 g/dL (normal; <11 g/dL = true anemia) |
| Hematocrit | Decreased | ~33-35% |
| Blood viscosity | Decreased | -20% |
| Platelets | -10% | 150,000-400,000/mm3 (mild dilutional thrombocytopenia) |
- Normal vaginal delivery: estimated blood loss (EBL) 300-500 mL
- Normal cesarean section: EBL 800-1000 mL
- Postpartum uterine contraction provides autotransfusion of ~500 mL of blood
- Iron requirement: 1000 mg throughout pregnancy
- Folate: 400-800 mcg/day supplementation required
6b. Coagulation - Hypercoagulable State
- Fibrinogen: increases 300-600 mg/dL (from baseline 250-400 mg/dL) - most striking change
- Factors II, VII, VIII, X, XII: all significantly increased (30-250% above baseline)
- von Willebrand factor (vWF): increased
- Plasminogen activator inhibitor (PAI-1 and PAI-2): increased
- Protein S: decreased
- Antithrombin III: minimally decreased
- Shortened prothrombin time (PT) and activated partial thromboplastin time (aPTT)
- Elevated D-dimer (physiologically elevated - not a reliable marker of DVT in pregnancy)
- 3-6 fold increased risk of venous thromboembolism (VTE) compared to non-pregnant women
- VTE risk persists for 6-12 weeks postpartum
Anesthetic Note - Coagulation and Regional Anesthesia:
- Platelet count > 70,000-80,000/mm3 is generally considered safe for neuraxial blockade (ASRA guidelines; institutional protocols vary, many require >100,000)
- Pre-eclampsia can rapidly cause thrombocytopenia - check platelet count before regional anesthesia in pre-eclamptic patients
- In patients on low molecular weight heparin (LMWH): neuraxial block safe after 12 hours (prophylactic dose) or 24 hours (therapeutic dose) from last injection
7. RENAL CHANGES
| Parameter | Change |
|---|---|
| Renal plasma flow | +60-80% by mid-pregnancy |
| Glomerular filtration rate (GFR) | +50% (by 3rd month) |
| Serum creatinine | Decreased (0.4-0.8 mg/dL in pregnancy) |
| Blood urea nitrogen (BUN) | Decreased (8-12 mg/dL) |
| Serum uric acid | Decreased early; increases in late pregnancy |
| Plasma osmolality | Decreased by 8-10 mOsm/kg |
- Decreased threshold for glucose reabsorption: glycosuria (1-10 g/day) is normal in pregnancy
- Decreased threshold for amino acid reabsorption: mild proteinuria (<300 mg/24h) is normal
- Sodium retention due to aldosterone and estrogen (but plasma Na+ decreases by ~5 mEq/L due to dilution)
- Kidneys enlarge by ~1 cm in length due to vascular engorgement
8. HEPATIC AND BILIARY CHANGES
8a. Liver Function Tests
- Alkaline phosphatase: increases 2-4 fold (placental isoform - not a sign of liver disease)
- AST, ALT, bilirubin: at upper limits of normal (mild increases in third trimester)
- GGT: decreases
- Serum albumin: decreases (~3.0-3.5 g/dL) due to hemodilution - increases free drug fraction of protein-bound drugs
8b. Pseudocholinesterase Activity
Anesthetic Note - Succinylcholine Duration: Despite the 25-30% reduction in pseudocholinesterase activity, the clinical duration of succinylcholine is not significantly prolonged in normal pregnant patients because the increased volume of distribution compensates. However, in patients with underlying pseudocholinesterase deficiency (dibucaine number <70), the reduced enzyme activity can lead to markedly prolonged neuromuscular blockade.Succinylcholine dose for RSI in pregnancy: 1.5 mg/kg IV (higher dose preferred due to expanded VD and to ensure rapid, reliable intubating conditions)
8c. Biliary System
- Bile composition changes favor cholesterol stone formation
- Incomplete gallbladder emptying - bile stasis
- Acute cholecystitis is the second most common cause of acute abdomen in pregnancy (after appendicitis)
9. ENDOCRINE AND METABOLIC CHANGES
9a. Hormonal Changes
| Hormone | Change | Key Effect |
|---|---|---|
| Progesterone | 20-fold increase | Respiratory stimulation, smooth muscle relaxation, decreased MAC, sedation |
| Estrogen | 10-fold increase | Mucosal edema, hepatic protein synthesis changes, increased CBG, TBG |
| hCG | Peaks at 10-12 weeks | Nausea and vomiting in first trimester; maintains corpus luteum |
| Cortisol | Increased | Insulin resistance, striae |
| Relaxin | Increased | Softens pubic symphysis, pelvic ligaments, cervical ripening |
| Prolactin | 10-fold increase at term | Lactation preparation |
| Aldosterone | Increased | Sodium and water retention |
9b. Glucose Metabolism
- Insulin resistance increases progressively (due to hPL, cortisol, estrogen, progesterone)
- Fasting blood glucose is lower in pregnancy (fetal glucose consumption)
- Post-prandial glucose is higher (insulin resistance)
- Gestational diabetes mellitus (GDM) develops in ~7-10% of pregnancies
9c. Thyroid
- Total T3 and T4 increase (due to increased thyroid-binding globulin from estrogen stimulation), but free T3 and T4 remain normal
- hCG has weak TSH-like activity; TSH may be transiently suppressed in first trimester
- Physiological goiter may develop (iodine redistribution to fetus)
10. MUSCULOSKELETAL AND PHARMACOKINETIC CHANGES
10a. Musculoskeletal
- Lumbar lordosis increases - to compensate for the anterior shift in center of gravity
- Sacroiliac joint and pubic symphysis loosening (relaxin effect) - back pain is nearly universal
- Diastasis recti (separation of rectus abdominis muscles)
- Carpal tunnel syndrome is common (fluid retention)
10b. Pharmacokinetic Changes Relevant to Anesthesia
| Parameter | Change | Implication |
|---|---|---|
| Volume of distribution (Vd) | Increased (+35% blood volume) | Higher loading doses may be needed |
| Protein binding | Decreased (albumin falls) | Increased free drug fraction of protein-bound drugs |
| Hepatic metabolism | Increased CYP3A4, decreased other enzymes | Variable drug clearance |
| Pseudocholinesterase | -25-30% | Succinylcholine (minor effect clinically) |
| GFR | +50% | Increased renal clearance of renally excreted drugs |
| MAC | -40% | Reduce volatile agent doses |
| Local anesthetic requirement | -30% | Reduce epidural and spinal doses |
11. CHANGES DURING LABOR AND DELIVERY
| Stage | CO Change | O2 Consumption | Other |
|---|---|---|---|
| First stage | +15% above prelabor | +40% | Pain drives hyperventilation; PaCO2 may fall to <20 mmHg |
| Second stage | +50% above prelabor | +75% | Pushing, Valsalva causes further CO changes |
| Immediately postpartum | +60-80% surge | Returns toward normal | Autotransfusion; IVC decompression |
- 28-32 weeks (peak CO)
- Active second stage of labor
- Immediately postpartum (maximum CO surge from autotransfusion)
12. SPECIAL ANESTHETIC CONSIDERATIONS - SUMMARY TABLE
| System | Key Change | Anesthetic Implication | Specific Precaution |
|---|---|---|---|
| Cardiovascular | CO +40%, SVR -15% | Hypotension common under regional/GA | Left uterine displacement, phenylephrine infusion |
| Respiratory | FRC -20%, O2 consumption +50% | Rapid desaturation | Mandatory preoxygenation, RSI |
| Airway | Mucosal edema, Mallampati worsens | Difficult airway | Smaller ETT (6.0-6.5mm), have difficult airway cart ready |
| CNS | MAC -40% | Less volatile agent needed | Adjust MAC accordingly; awakeness risk |
| CNS | LA sensitivity increased | Smaller epidural/spinal doses | Reduce doses 30% for epidural; careful titration |
| GI | LES incompetence, full stomach | Aspiration risk | Sodium citrate 30 mL, ranitidine 50 mg IV, RSI with cricoid pressure |
| Hematological | Dilutional anemia, hypercoagulable | Manage blood loss; DVT risk | Check CBC, coagulation before regional; VTE prophylaxis postpartum |
| Renal | GFR +50%, creatinine down | Normal creatinine may be deceiving | Use 0.5 mg/dL as upper normal in pregnancy |
| Hepatic | Pseudocholinesterase -25-30% | Minimal clinical impact on succinylcholine | Monitor NMB if pseudocholinesterase deficiency suspected |
13. DRUG DOSES QUICK REFERENCE FOR OBSTETRIC ANESTHESIA
| Drug | Indication | Dose |
|---|---|---|
| Phenylephrine | Spinal hypotension (first line) | 50-100 mcg IV bolus; infusion 0.25-0.5 mcg/kg/min |
| Ephedrine | Spinal hypotension with bradycardia | 5-10 mg IV bolus |
| Succinylcholine | RSI in pregnancy | 1.5 mg/kg IV |
| Propofol | Induction for GA | 1.5-2 mg/kg IV (use 1.5 in hemodynamically compromised) |
| Sodium citrate | Aspiration prophylaxis | 0.3M, 30 mL PO - immediately before induction |
| Ranitidine | H2 blocker - aspiration prophylaxis | 150 mg PO OR 50 mg IV slowly |
| Metoclopramide | Prokinetic, raises LES tone | 10 mg IV |
| Bupivacaine (spinal for CS) | Subarachnoid block | 0.5% hyperbaric bupivacaine 1.5-2 mL + fentanyl 25 mcg + morphine 100-200 mcg |
| Bupivacaine (epidural labor) | Labor analgesia | 0.1% bupivacaine + fentanyl 2 mcg/mL (PCEA) |
| Oxytocin | Uterotonic post-delivery | 5 IU slow IV (do NOT give as rapid bolus - causes hypotension) |
| Atropine | Bradycardia | 0.6 mg IV |
| Ondansetron | PONV / spinal nausea | 4-8 mg IV |
CONCLUSION
- CO increases 40% - peaks at 28-32 weeks
- FRC decreases 20% + O2 consumption increases 50% = rapid desaturation - mandatory preoxygenation
- Aortocaval compression after 20 weeks - left uterine displacement always
- MAC decreases 40% - reduce volatile agent doses
- Aspiration risk from week 18-20 onwards - RSI + aspiration prophylaxis for GA
- Local anesthetic dose reduced 30% for regional techniques
- Difficult airway anticipated due to airway edema - plan, plan, plan
REFERENCES
-
Morgan GE, Mikhail MS, Murray MJ. Morgan and Mikhail's Clinical Anesthesiology, 7th Edition. McGraw-Hill. Chapter 40: Obstetric Anesthesia. Table 40-1.
-
Gropper MA. Miller's Anesthesia, 10th Edition, 2-Volume Set. Elsevier, 2023. Chapter 58: Obstetric Anesthesia. Tables 58.2 and 58.3.
-
Townsend CM, Beauchamp RD, Evers BM. Sabiston Textbook of Surgery, 21st Edition. Chapter 26: Surgical Complications.
-
Datta S, Kodali BS, Segal S. Obstetric Anesthesia Handbook, 5th Edition. Springer. Chapter 1: Maternal Physiological Changes.
-
Creasy RK, Resnik R. Creasy & Resnik's Maternal-Fetal Medicine: Principles and Practice, 8th Edition. Elsevier. Chapter: Maternal Adaptations.
-
NYSORA. Physiological changes during pregnancy - Practical anesthetic implications table.
-
OpenAnesthesia.org. Physiologic changes in pregnancy - Anesthetic considerations by system.
-
Tveita T, Sieck GC. Physiological Impact of Hypothermia: The Good, the Bad, and the Ugly. Physiology (Bethesda). 2022 Mar 1 [PMID: 34632808]
Examiner's Tip (RGUHS 10-marker): This topic is frequently asked in combination with "obstetric anesthesia for cesarean section" or "anesthesia in pre-eclampsia." Always anchor each system's change to a specific anesthetic implication - examiners award extra marks for applied knowledge, not just listed facts. Drug doses with correct units always gain marks.
Intra-operative estimation of blood loss
intraoperative blood loss estimation methods accuracy
intraoperative estimation of blood loss methods visual gravimetric photometric colorimetric allowable blood loss formula anesthesia 10 marker
https://link.springer.com/article/10.1186/s12893-024-02699-3
ATLS hemorrhagic shock classification blood loss class I II III IV anesthesia management transfusion trigger perioperative
Medical flowchart titled "Methods of Intraoperative Blood Loss Estimation" showing a hierarchical diagram with two main branches: 1) QUALITATIVE/CLINICAL METHODS including Visual Estimation (sponge counting, suction canister, surgical field assessment), Clinical Signs (HR, BP, urine output, skin color), 2) QUANTITATIVE METHODS including Gravimetric Method (weighing sponges, 1g=1mL formula), Colorimetric/Photometric Method (spectrophotometry, Triton app), Mathematical Formulas (MABL formula, Moore formula, Hb-based formula). Include a third branch: LABORATORY MONITORING (serial Hb/Hct, coagulation, TEG/ROTEM). Each method labeled with advantages and limitations. Clean medical flowchart with color coding.
Medical table diagram titled "ATLS Classification of Hemorrhagic Shock" with 5 columns (Parameter, Class I, Class II, Class III, Class IV) and rows showing: Blood Loss mL (less than 750, 750-1500, 1500-2000, greater than 2000), Blood Loss % (less than 15%, 15-30%, 30-40%, greater than 40%), Heart Rate (less than 100, 100-120, 120-140, greater than 140), Blood Pressure (Normal, Normal, Decreased, Very low), Pulse Pressure (Normal/increased, Decreased, Decreased, Decreased), Respiratory Rate (14-20, 20-30, 30-40, greater than 35), Urine Output mL/hr (greater than 30, 20-30, 5-15, Negligible), Mental Status (Slightly anxious, Mildly anxious, Anxious/confused, Confused/lethargic), Fluid Replacement (Crystalloid, Crystalloid, Blood+crystalloid, Blood+crystalloid). Use color gradient from green for Class I to red for Class IV. Clean medical table format.
Medical diagram titled "Calculation of Maximum Allowable Blood Loss (MABL) - Step by Step". Show a step-by-step flowchart: Step 1: Estimate Blood Volume (EBV) using table (Premature infant 90-100 mL/kg, Term neonate 80-90 mL/kg, Infant 75-80 mL/kg, Child 70-75 mL/kg, Adult male 75 mL/kg, Adult female 65 mL/kg, Obese BMI 30: 60 mL/kg). Step 2: Determine Initial Hematocrit (HCTi). Step 3: Set Target/Threshold Hematocrit (HCTf) - typically 21-24% for healthy adults, 28-30% for cardiac/elderly. Step 4: Apply Formula: MABL = EBV x (HCTi - HCTf) / HCTi. Show a worked example: 70kg adult male, HCTi=42%, HCTf=21%, EBV=5250mL, MABL=2625mL. Step 5: Management algorithm based on blood loss vs MABL. Clean mathematical medical diagram style.
INTRA-OPERATIVE ESTIMATION OF BLOOD LOSS
MD Anesthesia Postgraduate - 10-Marker Answer (RGUHS Format)
1. INTRODUCTION
- Determine when to replace blood - identifying the need for transfusion
- Guide fluid resuscitation - crystalloid vs. colloid vs. blood products
- Prevent the lethal triad - hypothermia, acidosis, and coagulopathy in the massively bleeding patient
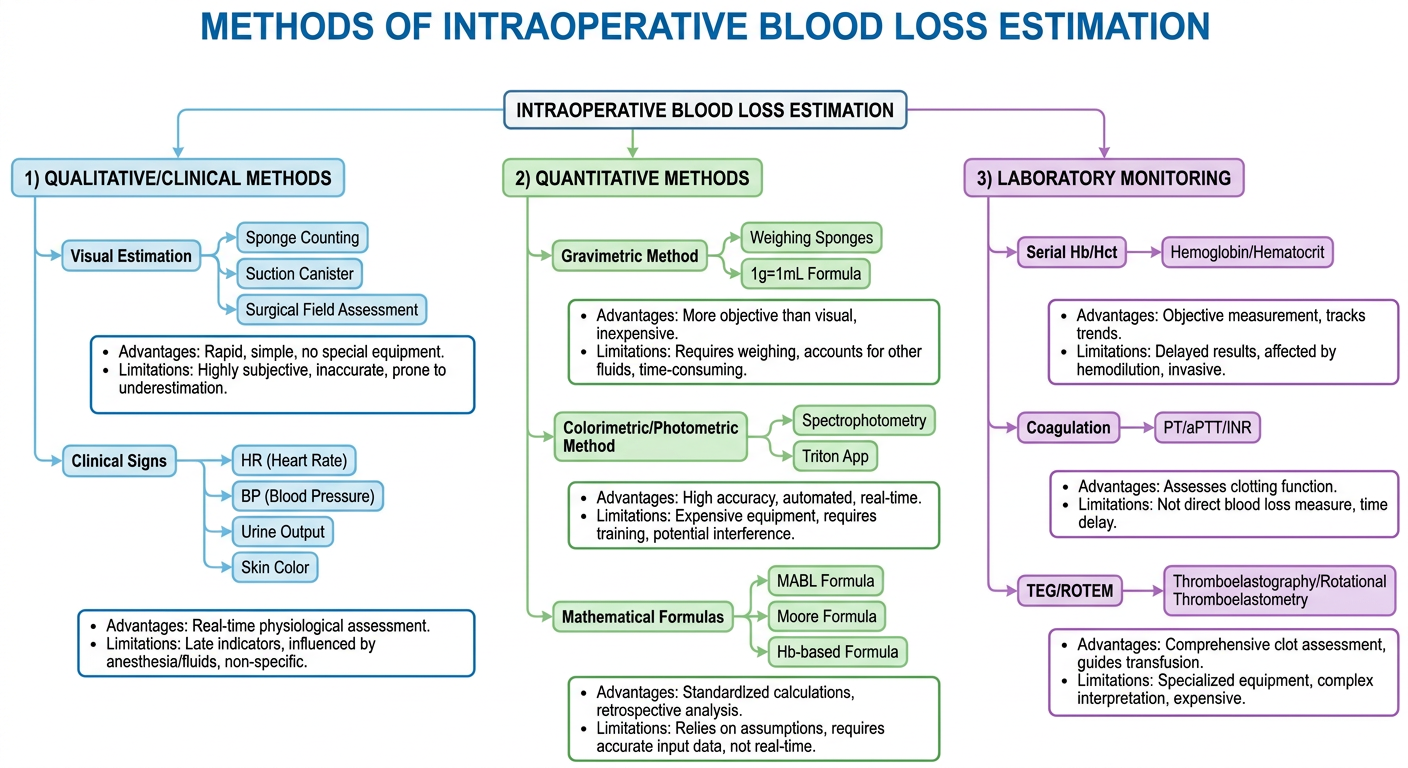
2. CLASSIFICATION OF METHODS
A. QUALITATIVE / CLINICAL METHODS
1. Visual estimation
2. Clinical signs and hemodynamic monitoring
3. ATLS hemorrhagic shock classification
B. QUANTITATIVE METHODS
1. Gravimetric method (weighing)
2. Colorimetric / photometric method
3. Spectrophotometric method
4. Mathematical formulae (MABL, Moore, Hb-based)
C. LABORATORY METHODS
1. Serial hemoglobin / hematocrit
2. Coagulation studies (PT, aPTT, fibrinogen)
3. Point-of-care coagulation (TEG / ROTEM)
4. Arterial blood gas with lactate
D. ADVANCED / EMERGING METHODS
1. Near-infrared spectroscopy (NIRS)
2. Artificial intelligence - image-based (Triton system)
3. Ultrasound-based assessment (IVC collapsibility, FAST)
3. QUALITATIVE / CLINICAL METHODS
3a. Visual Estimation
- Blood in the suction canister
- Blood on surgical sponges, drapes, and the operative field
- Blood on the floor
- Blood in wound irrigation fluid
| Sponge Type | Approximate Blood Absorption |
|---|---|
| 4 x 4 gauze (fully soaked) | ~10 mL |
| Ray-Tec / gauze sponge (fully soaked) | ~10-20 mL |
| Laparotomy sponge (fully soaked) | ~100-150 mL |
| Small swab | ~5 mL |
- Highly subjective and operator-dependent
- Consistently underestimates true blood loss by 30-50% (surgeons and nurses tend to underestimate; more experienced providers are more accurate)
- Does not account for blood on drapes, floor, and in cavities
- Suction canister volume is confounded by irrigation fluid
- Affected by lighting conditions and viewing angle
- Studies show AUC of 0.74 for clinically significant blood loss vs 0.81 for gravimetric method
Anesthetic Note: Even experienced anesthesiologists underestimate blood loss, particularly in obstetric hemorrhage. A structured quantitative approach (weighing + suction) is strongly recommended in high-risk procedures such as LSCS, cardiac surgery, hepatic resection, and trauma laparotomy.
3b. Swab/Sponge Count
- Dry weight of sponge types should be known preoperatively
- All used sponges should be collected and accounted for
- Approximate blood on sponges = visual estimate using known absorptive capacities
- Combine with suction canister volume
3c. Suction Canister Assessment
- Direct reading of graduated suction canister
- Subtract the volume of irrigation fluid used intraoperatively
- If irrigation fluid used is not accurately recorded, this method becomes inaccurate
- Formula: Blood loss via suction = Canister volume - Irrigation volume
4. CLINICAL SIGNS AND ATLS CLASSIFICATION
4a. Hemodynamic Parameters
| Parameter | Significance |
|---|---|
| Heart rate | First sign of significant hemorrhage - tachycardia (>100 bpm) |
| Blood pressure | Late sign - MAP falls only after >30% blood loss in young patients |
| Pulse pressure | Narrows early (vasomotor tone rises to maintain systolic BP) |
| Central venous pressure (CVP) | Decreases with hypovolemia; trends more useful than absolute values |
| Urine output | Target >0.5 mL/kg/h - organ perfusion marker |
| End-tidal CO2 | Decreases with severe hemorrhage and reduced cardiac output |
| Pulse oximetry waveform | Diminished amplitude / dampened waveform with low CO |
| Stroke volume variation (SVV) | Reliable indicator of fluid responsiveness in mechanically ventilated patients; SVV >13% suggests fluid responsiveness |
| Pulse pressure variation (PPV) | Similar utility to SVV for predicting response to volume |
Anesthetic Note - Pitfall: In the anesthetized patient, the usual autonomic signs of hemorrhagic shock (tachycardia, sweating, agitation) are masked. The anesthesiologist must rely more heavily on invasive hemodynamic monitoring, urine output trends, and laboratory values than in the awake patient.
4b. ATLS Classification of Hemorrhagic Shock
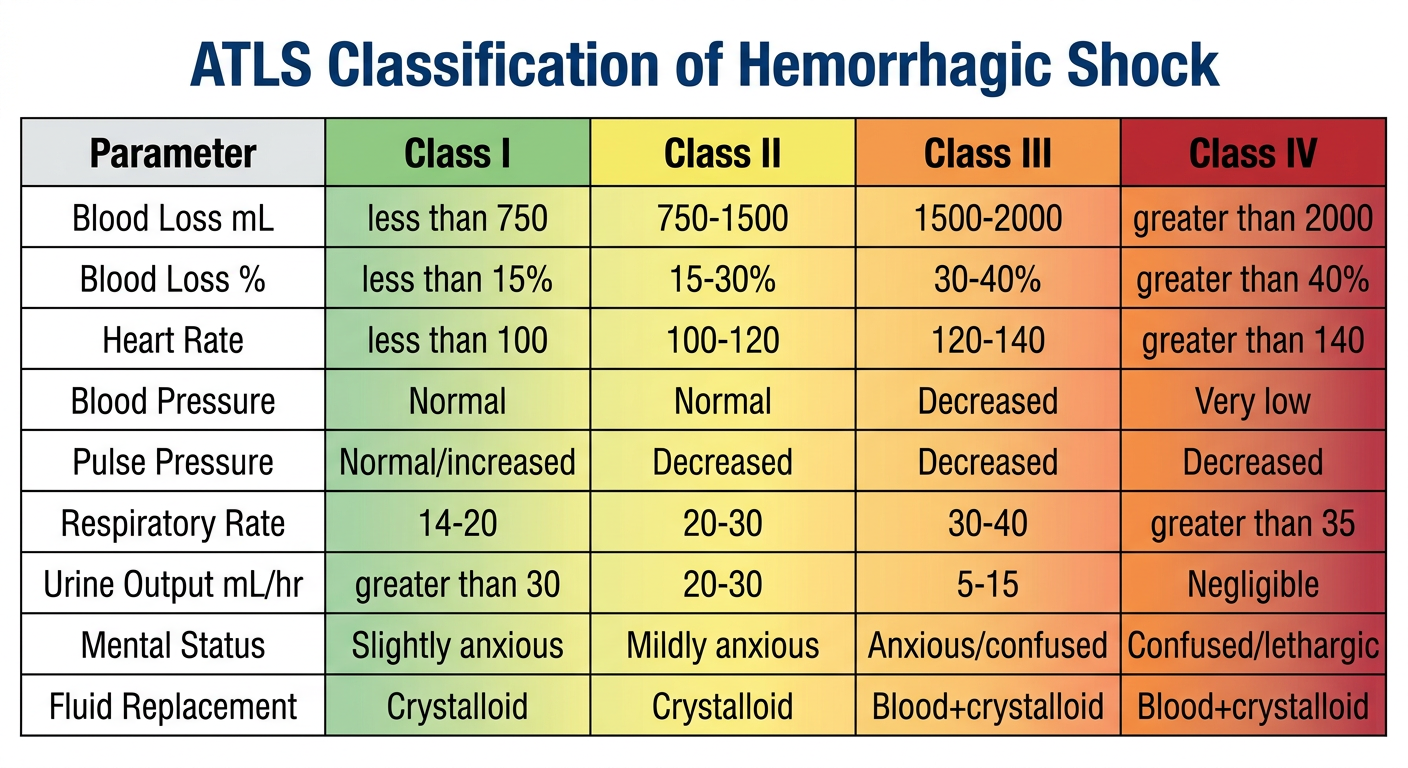
| Parameter | Class I | Class II | Class III | Class IV |
|---|---|---|---|---|
| Blood loss (mL) | <750 | 750-1500 | 1500-2000 | >2000 |
| Blood loss (%) | <15% | 15-30% | 30-40% | >40% |
| Heart rate | <100 | >100 | >120 | >140 |
| Blood pressure | Normal | Normal | Decreased | Very low |
| Pulse pressure | Normal/increased | Decreased | Decreased | Decreased |
| Respiratory rate | 14-20 | 20-30 | 30-40 | >35 |
| Urine output (mL/h) | >30 | 20-30 | 5-15 | Negligible |
| CNS/Mental status | Slightly anxious | Mildly anxious | Anxious, confused | Confused, lethargic |
| Fluid replacement | Crystalloid | Crystalloid | Crystalloid + blood | Crystalloid + blood |
- Anesthesia masks tachycardia, agitation, and CNS changes
- Beta-blockers blunt tachycardia
- Young, athletic patients may maintain BP despite 30-40% volume loss
- Elderly and hypertensive patients may show BP changes with smaller losses
- The classification was developed for awake trauma patients - not rigorously validated intraoperatively
5. QUANTITATIVE METHODS
5a. Gravimetric Method (Weighing Method)
- Record the dry weight of each type of sponge/gauze preoperatively (manufacturers provide standard weights, or pre-weigh a sample)
- Collect all used sponges in a calibrated container
- Weigh all soaked sponges on a calibrated scale
- Subtract total dry weight of all sponges from total wet weight
- Divide by 1.06 (specific gravity of blood) - though in clinical practice, 1g = 1mL is used
Blood in sponges (mL) = [Wet weight (g) - Dry weight (g)] / 1.06
≈ Wet weight (g) - Dry weight (g) [practical approximation]
| Sponge | Dry weight |
|---|---|
| 4x4 gauze | 2-3 g |
| Ray-Tec | 3-5 g |
| Laparotomy sponge | 25-30 g |
- More objective than visual estimation
- Real-time, bedside use
- Accounts for non-visible blood absorption
- Validated to be more accurate than visual method (Bai et al, 2026; multiple studies)
- Requires careful collection and labeling of all sponges
- Cannot separate blood from irrigation fluid in soaked sponges
- Does not capture blood on floor, drapes, or within body cavities
- Time-consuming in high-volume, fast bleeding situations
5b. Colorimetric Method
- A smartphone-based application that uses the device camera
- Takes photographs of used surgical gauze and suction canisters
- Uses machine learning-based image feature extraction to calculate hemoglobin mass in each item
- Correlates with preoperative hematocrit to calculate blood volume loss
- Studies show this has the highest correlation with actual blood loss compared to visual and gravimetric methods (meta-analysis by Gerdessen et al.)
- FDA-cleared for clinical use
- More accurate than visual and gravimetric methods
- Quick, non-contact measurement
- Captures blood on drapes and field (via photography)
- Provides hemoglobin-specific data (not just volume)
- Requires smartphone/tablet and reliable app
- Cost
- Learning curve
- Less validated in extreme conditions
5c. Spectrophotometric Method (Gold Standard)
- All blood-soaked materials are dissolved in a known volume of water/saline
- Absorbance is measured using a spectrophotometer
- Hemoglobin concentration calculated from a calibration curve
- Blood volume = Hemoglobin mass / Patient's hemoglobin concentration
- Labor-intensive and time-consuming
- Requires laboratory equipment
- Not suitable for real-time intraoperative use
- Used primarily in research studies to validate other methods
6. MATHEMATICAL FORMULAE FOR BLOOD LOSS ESTIMATION
6a. Estimated Blood Volume (EBV)
| Patient Category | EBV (mL/kg) |
|---|---|
| Premature infant | 90-100 |
| Term neonate | 80-90 |
| Infant (<1 year) | 75-80 |
| Child (1-12 years) | 70-75 |
| Adolescent (12-18 years) | 70 |
| Adult male | 75 |
| Adult female | 65 |
| Obese adult (BMI 30) | 60 |
| Obese adult (BMI 40) | 55 |
| Obese adult (BMI 50) | 50 |
- Males: EBV = (0.3669 × Height³[m]) + (0.03219 × Weight[kg]) + 0.6041
- Females: EBV = (0.3561 × Height³[m]) + (0.03308 × Weight[kg]) + 0.1833
- (Result in liters; multiply by 1000 for mL)
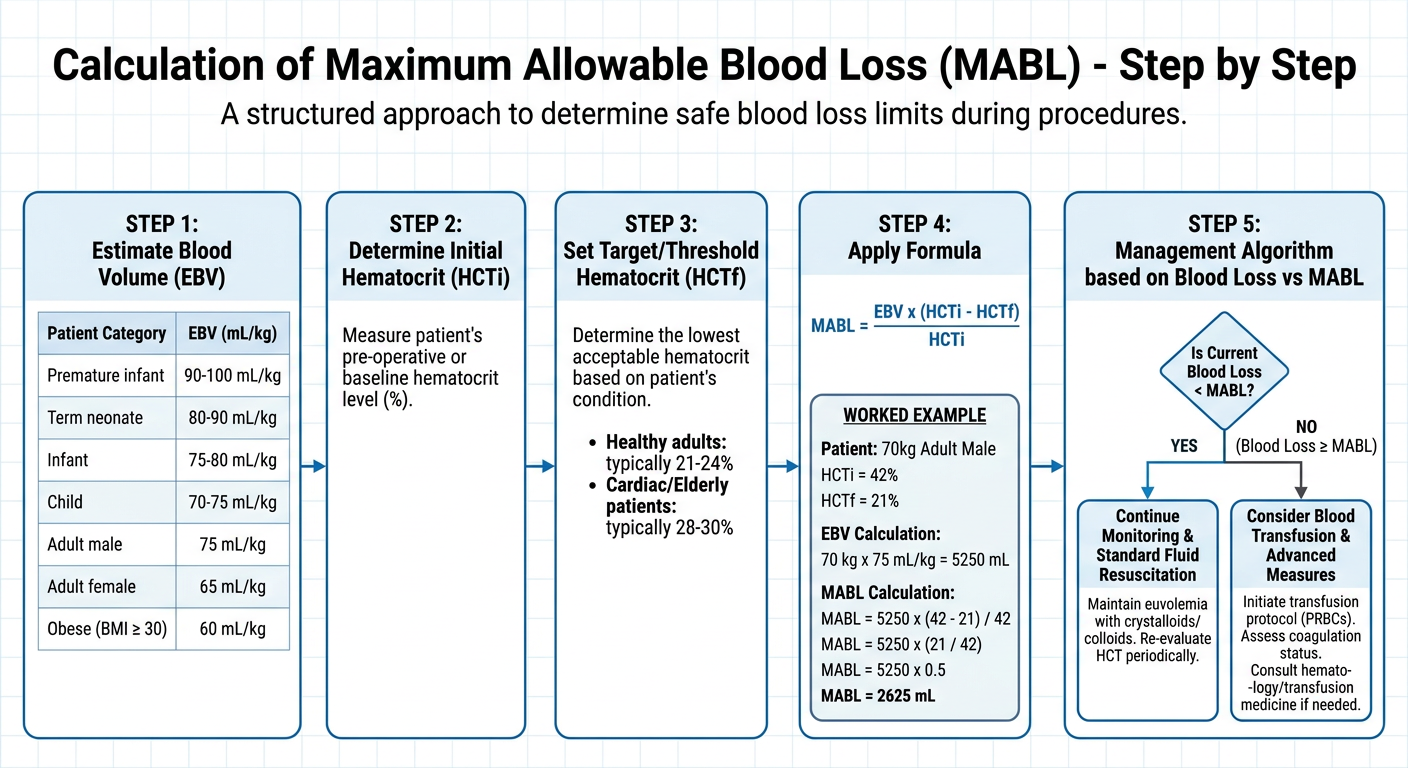
6b. Maximum Allowable Blood Loss (MABL) Formula
MABL = EBV × (HCTi - HCTf) / HCTi
- EBV = Estimated Blood Volume (mL)
- HCTi = Initial preoperative hematocrit (%)
- HCTf = Final/threshold hematocrit (%) - the lowest acceptable hematocrit
Patient: 70 kg adult male, Hct = 42%, target Hct = 21%
EBV = 70 kg × 75 mL/kg = 5250 mL
MABL = 5250 × (42 - 21) / 42
MABL = 5250 × 0.5 = 2625 mL
| Patient Type | Transfusion Threshold Hct | Hemoglobin Equivalent |
|---|---|---|
| Healthy young adult | 21-24% | 7-8 g/dL |
| Elderly / coronary artery disease | 28-30% | 9-10 g/dL |
| Cardiac disease, poor LV function | 30% | 10 g/dL |
| Premature/term neonate | 30-35% | 10-11 g/dL |
| Cyanotic CHD | Higher, individualized | Discuss with cardiologist |
Current transfusion guidelines (ASA, SABM): A "restrictive" strategy with Hb trigger of 7-8 g/dL (Hct 21-24%) is recommended for stable, non-cardiac patients. A "liberal" trigger of Hb 9-10 g/dL is used for those with cardiac disease, poor cardiopulmonary reserve, or active myocardial ischemia.
6c. Moore's Formula (Hemoglobin-Based)
Blood Loss (mL) = EBV × (Hbi - Hbf) / Hb_average
- Hbi = initial hemoglobin
- Hbf = final hemoglobin
- Hb_average = mean of initial and final hemoglobin
6d. Hematocrit-Based Formula (During Surgery)
Blood loss ≈ EBV × (HCTi - HCTcurrent) / HCTi
7. LABORATORY MONITORING
7a. Serial Hemoglobin / Hematocrit
- Point-of-care (POC) hemoglobin analyzers (HemoCue, i-STAT) provide rapid results
- Acute hemorrhage does not immediately change hemoglobin - equilibration takes 2-4 hours
- In acute hemorrhage, a normal Hb does NOT exclude significant blood loss
- Serial trending is more valuable than a single value
- With active IV fluid administration, Hb/Hct fall faster (hemodilution)
7b. Coagulation Studies
- Prothrombin time (PT) / INR
- Activated partial thromboplastin time (aPTT)
- Fibrinogen - falls early in coagulopathic hemorrhage; critical level <1.5 g/L
- Platelet count - target >50,000/mm3 in active bleeding; >100,000 in CNS injury
7c. Viscoelastic Tests - TEG and ROTEM
| Parameter | Measures | Normal Value |
|---|---|---|
| R time (reaction time) | Enzymatic clot initiation | 5-10 min |
| K time | Fibrinogen contribution to clot strength | 1-3 min |
| Alpha angle (α) | Speed of clot strengthening | 53-72° |
| MA (maximum amplitude) | Platelet + fibrin clot strength | 51-69 mm |
| LY30 | Fibrinolysis at 30 min | <8% |
| CI (coagulation index) | Overall coagulation status | -3 to +3 |
Anesthetic Note - TEG/ROTEM in massive hemorrhage: TEG/ROTEM allow targeted, goal-directed transfusion therapy - giving the right blood product for the specific coagulopathic defect rather than empirical FFP/platelet transfusion. This reduces overall blood product use and transfusion-related complications.
7d. Arterial Blood Gas with Lactate
- Base deficit (negative base excess) correlates with tissue hypoperfusion from blood loss
- Base deficit >-6 mEq/L suggests significant hemodynamic compromise
- Serum lactate >2 mmol/L = tissue hypoperfusion; >4 mmol/L = severe shock
- Serial lactate clearance guides adequacy of resuscitation (target >10% clearance per hour)
- Serial ABGs provide rapid hemoglobin values via hemoximetry channels
8. REPLACEMENT STRATEGY BASED ON ESTIMATED BLOOD LOSS
8a. Replacement Ratios
| Blood Loss | Replacement | Ratio |
|---|---|---|
| Up to 15% EBV | Crystalloid (Ringer's Lactate or Normal Saline) | 3:1 (crystalloid: blood loss) |
| 15-30% EBV | Crystalloid ± Colloid | 3:1 crystalloid; 1:1 colloid |
| Approaching MABL | Start blood transfusion (pRBC) | 1:1 (pRBC: blood loss) |
| >MABL | pRBC + FFP + Platelets; Massive Transfusion Protocol | 1:1:1 ratio |
8b. pRBC Transfusion Dose
Volume of pRBC required (mL) =
Desired ΔHb (g/dL) × EBV (mL) / Hb of donor unit
Simple approximation:
4-5 mL/kg of pRBC raises hemoglobin by 1 g/dL
8c. Massive Transfusion Protocol (MTP)
| Component | Target Ratio | Dose |
|---|---|---|
| pRBC | 1 unit | 250-350 mL |
| FFP | 1:1 with pRBC | 10-15 mL/kg |
| Platelets | 1 pool / 4-6 pRBC | 1 apheresis unit (~250 mL) |
| Cryoprecipitate | If fibrinogen <1.5 g/L | 2-3 pools (10 units) |
| Tranexamic acid (TXA) | Within 3 hours of injury | 1g IV over 10 min, then 1g over 8h |
| Calcium chloride | Per 4 units pRBC | 1g IV (chelation by citrate in blood products) |
TXA (Tranexamic Acid) Key Dose: CRASH-2 trial established 1g IV bolus over 10 minutes, then 1g infusion over 8 hours for trauma hemorrhage. Must be given within 3 hours of injury onset - after this, mortality risk increases. WOMAN trial confirmed benefit in postpartum hemorrhage: 1g IV, repeat if bleeding continues at 30 min.
9. ADVANCES IN BLOOD LOSS ESTIMATION
9a. Triton System (AI-Based Colorimetry)
- Uses smartphone camera + machine learning algorithm
- Photographs surgical sponges and suction canisters
- Calculates hemoglobin mass and estimates blood loss in real-time
- Multiple studies confirm superior accuracy over visual and gravimetric methods
- Meta-analysis (Gerdessen et al.) showed highest correlation with actual blood loss
9b. Near-Infrared Spectroscopy (NIRS) / Cerebral Oximetry
- Monitors regional tissue oxygenation (rSO2) non-invasively
- Cerebral rSO2 <50% or drop >20% from baseline suggests critical cerebral hypoperfusion from hemorrhage
- Useful surrogate marker of hemorrhagic compromise in neurologically monitored patients
9c. Focused Cardiac Ultrasound (FOCUS) / FAST
- IVC diameter and collapsibility index: IVC collapsibility >50% suggests hypovolemia
- FAST exam: detects intra-abdominal free fluid (occult hemorrhage)
- Serial LV function assessment guides need for vasopressors vs. volume
9d. Continuous Non-Invasive Hemoglobin (SpHb - Masimo)
- Masimo Radical-7 pulse co-oximeter provides continuous, non-invasive hemoglobin monitoring
- Not a replacement for laboratory Hb; used for trend monitoring
- Accuracy affected by poor perfusion, dyshemoglobins, motion
- Useful in procedures with anticipated significant bleeding for real-time Hb trending
10. SPECIAL SITUATIONS IN OBSTETRIC PRACTICE
- Weigh all blood-soaked materials (pads, sponges, drapes)
- Measure blood in graduated drapes/under-buttocks drape
- Calibrated collection bags placed under the patient
- Subtract irrigation/amniotic fluid volume
- Primary PPH: Blood loss ≥500 mL (vaginal delivery) or ≥1000 mL (CS) within 24h
- Severe PPH: ≥1000 mL with signs of hemodynamic instability
Evidence: Quantitative blood loss assessment (QBL) reduces the risk of severe maternal morbidity compared to visual estimation. ACOG (2019) and WHO (2023) both recommend QBL as routine practice in obstetric units.
11. A PRACTICAL INTRAOPERATIVE ALGORITHM
PREOPERATIVE PLANNING
├── Calculate EBV (Nadler or body-weight formula)
├── Record baseline Hb/Hct
├── Calculate MABL [= EBV × (HCTi - HCTf) / HCTi]
├── Type and screen/crossmatch blood as per anticipated surgery
└── Establish IV access, arterial line for major procedures
INTRAOPERATIVE MONITORING
├── Visual estimate: sponge count + suction canister (subtract irrigation)
├── Gravimetric method: weigh sponges at regular intervals
├── Hemodynamic monitoring: HR, BP, CVP, urine output
├── PPV/SVV on ventilated patients (fluid responsiveness)
├── Serial ABG/Hb (if ongoing significant loss)
└── TEG/ROTEM if coagulopathy suspected
DECISION TO TRANSFUSE
├── EBL < 15% → Crystalloid 3:1
├── EBL 15-30% → Crystalloid ± Colloid
├── EBL approaching MABL → Start pRBC
├── EBL > MABL → pRBC + FFP + Platelets
└── EBL > 1 EBV → Activate MTP; add TXA 1g IV + Calcium
12. SUMMARY TABLE - COMPARISON OF METHODS
| Method | Accuracy | Speed | Cost | Equipment | Best Use |
|---|---|---|---|---|---|
| Visual estimation | Low-moderate | Very fast | Nil | Nil | Routine, any setting |
| Gravimetric | Moderate-good | Fast | Low | Weighing scale | Routine-major surgery |
| Colorimetric (Triton) | High | Fast | Moderate | Smartphone | High-risk surgery, research |
| Spectrophotometric | Highest | Slow | High | Lab equipment | Research/gold standard |
| MABL formula | Good (planning) | Pre-op | Nil | Calculator | Preoperative planning |
| Serial Hb/Hct | Good (real-time) | Moderate | Low | POC analyzer | All cases |
| TEG/ROTEM | Excellent (coag) | 10-20 min | High | Dedicated analyzer | Massive hemorrhage |
| SpHb (Masimo) | Moderate (trends) | Real-time | Moderate | CO-oximeter | Trend monitoring |
13. KEY DRUG DOSES RELEVANT TO BLOOD LOSS MANAGEMENT
| Drug | Indication | Dose |
|---|---|---|
| Tranexamic acid (TXA) | Reducing surgical blood loss | 1g IV over 10 min (then 1g over 8h); Give within 3 hours |
| Calcium chloride 10% | Hypocalcemia with massive transfusion | 1g IV slowly per 4 units pRBC |
| Adrenaline (epinephrine) | Anaphylaxis/cardiac arrest during massive hemorrhage | 1 mg IV (cardiac arrest); 10-20 mcg IV bolus (hemodynamic compromise) |
| Vasopressin | Refractory vasodilatory shock with hemorrhage | 0.03-0.04 units/min infusion |
| Noradrenaline | Maintaining MAP during resuscitation | 0.1-0.3 mcg/kg/min infusion |
| Desmopressin (DDAVP) | Uremic platelet dysfunction, von Willebrand disease | 0.3 mcg/kg IV over 30 min |
| Fibrinogen concentrate | Low fibrinogen (<1.5 g/L) | 2-4g IV |
| Protamine | Heparin reversal (post-CPB) | 1mg per 100 units heparin IV |
| Factor VII (rFVIIa, Novoseven) | Refractory, life-threatening coagulopathic hemorrhage | 90 mcg/kg IV (off-label) |
| Ondansetron | PONV from blood (nausea/vomiting in hypovolemia) | 4mg IV |
CONCLUSION
- Gravimetric weighing of sponges
- Measured suction canister volumes minus irrigation
- Clinical hemodynamic monitoring
- Serial laboratory values (Hb, coagulation, ABG)
- MABL-guided transfusion decision-making
- How much has the patient lost? (Estimation)
- How much can they afford to lose? (MABL)
- What does their physiology tell me? (Clinical signs + hemodynamics)
- What does their blood tell me? (Labs + TEG/ROTEM)
- What do I replace, and with what? (Crystalloid / Colloid / Blood products / Factors)
REFERENCES
-
Barash PG, Cullen BF, Stoelting RK. Barash, Cullen, and Stoelting's Clinical Anesthesia, 9th Edition. Wolters Kluwer, 2022. Chapter 15: Pediatric Anesthesia - Blood Transfusion Therapy.
-
Sabiston DC. Sabiston Textbook of Surgery, 22nd Edition. Elsevier, 2022. Chapter 33: Physiology of Shock - Table 33.1 ATLS Classes of Hemorrhagic Shock.
-
Gropper MA. Miller's Anesthesia, 10th Edition. Elsevier, 2023. Chapter 58 - Obstetric Anesthesia; Chapter 14 - Blood Component Therapy.
-
Bai J, Lu Y, Wang G. Rethinking intraoperative blood loss monitoring: a decision-oriented framework for clinically integrated assessment. Int J Burns Trauma. 2026. [PMID: 42181146]
-
OpenAnesthesia.org. Maximum Allowable Blood Loss. IARS, 2023.
-
BMC Surgery. Calculation methods for intraoperative blood loss: a literature review. Bai et al., 2024.
-
Algadiem EA et al. Blood Loss Estimation Using Gauze Visual Analogue. Trauma Mon. 2016;21(2):e34131.
-
Gerdessen L et al. The visually estimated blood volume in scaled canisters based on a simulation study. BMC Anesthesiol. 2021;21(1):54.
-
CRASH-2 trial collaborators. Effects of tranexamic acid on death, vascular occlusive events, and blood transfusion in trauma patients with significant haemorrhage. Lancet. 2010;376(9734):23-32.
-
Pediatric Anesthesia Society. Allowable Blood Loss. Evidence-Based Guidelines Review. 2023.
Examiner's Tip (RGUHS 10-marker): This question frequently appears paired with "blood transfusion" or "massive hemorrhage management." Always include: (1) the MABL formula with a worked example, (2) ATLS classification table, (3) the gravimetric method with sponge volumes, (4) TEG/ROTEM brief mention, and (5) TXA dosing. Diagrams with the ATLS table and MABL calculation flowchart are high-yield for marks.