I am 2nd yr mbbs Student from knruhs University i wanna learn pathology from scratch i have my final exam in sept firsfirst week but I also have my pre final exam in July 1st week for that also I have to complete my whole syllabus and I am starting patho now it self can u help me to study patho and give me the correct practical time table to study patho with topics per day to complete syllabus easily n I also have my clg 9-5 and also have to study 2 more subjects like Pharmacology and microbiology... Guide me please to study for my university and also build my concept
Asking for Preferences
Searching the Web
KNRUHS 2nd year MBBS pathology syllabus topics list
Finding Sources
Reading Web Page
https://www.scribd.com/document/529010822/Second-MBBS-Pathol…
Finding Sources
Finding Sources
I have all the information I need to build your complete plan. Let me now put together the full study guide.
🩺 Complete Pathology Study Plan - KNRUHS 2nd MBBS
Your situation at a glance:
- Today: May 29, 2026 (Friday)
- Pre-final exam: July 1st week (~33 days away)
- Final exam: September 1st week (~95 days away)
- College hours: 9 AM - 5 PM (not available for study)
- Study time per day: 3-4 hours (evenings/night + early morning)
- Subjects: Pathology + Pharmacology + Microbiology
- Pathology level: Starting from zero
PHASE 1 - YOUR DAILY TIME BUDGET
| Slot | Time | Subject |
|---|---|---|
| Evening (5:30-6:30 PM) | 1 hour | Pharmacology |
| Evening (6:30-8:30 PM) | 2 hours | Pathology (main focus) |
| Night (9:00-9:45 PM) | 45 min | Microbiology |
| Morning (6:00-6:30 AM) | 30 min | Quick revision of previous day's patho |
Pathology gets the longest prime slot because it has the most content and needs concept-building. The morning 30-min slot is ONLY for writing 5-point notes you already read, not new learning.
PHASE 2 - THE FULL PATHOLOGY SYLLABUS
Standard 2nd MBBS pathology is split into General Pathology (GP) and Systemic Pathology (SP). For KNRUHS and all Indian universities, this is what you must cover:
GENERAL PATHOLOGY (GP) - ~16 topics
| # | Topic | Approximate Weight |
|---|---|---|
| 1 | Introduction to Pathology + Cell Injury | High |
| 2 | Cell Death: Necrosis, Apoptosis, Gangrene | High |
| 3 | Cellular Adaptations (Atrophy, Hypertrophy, Hyperplasia, Metaplasia, Dysplasia) | High |
| 4 | Intracellular accumulations + Calcification | Medium |
| 5 | Acute Inflammation | Very High |
| 6 | Chronic Inflammation + Granulomatous Inflammation | Very High |
| 7 | Healing and Repair (Wound healing) | High |
| 8 | Hemodynamic disorders (Edema, Congestion, Hyperemia, Thrombosis, Embolism, Infarction) | Very High |
| 9 | Shock | High |
| 10 | Neoplasia - Part 1 (Nomenclature, Carcinogenesis, Tumor markers) | Very High |
| 11 | Neoplasia - Part 2 (Spread, Grading, Staging, Paraneoplastic syndromes) | Very High |
| 12 | Immunity and Immunopathology (Hypersensitivity types I-IV) | High |
| 13 | Autoimmune diseases (SLE, RA basics) | Medium |
| 14 | Amyloidosis | Medium |
| 15 | Genetic and pediatric disorders (Down syndrome, Turner, Klinefelter, etc.) | Medium |
| 16 | Environmental and Nutritional pathology | Low-Medium |
SYSTEMIC PATHOLOGY (SP) - ~12 topics
| # | Topic | Approximate Weight |
|---|---|---|
| 17 | Hematology - Anemias (IDA, megaloblastic, hemolytic, aplastic) | Very High |
| 18 | Hematology - Leukemias + Lymphomas | Very High |
| 19 | Cardiovascular Pathology (Atherosclerosis, MI, Hypertension, Valvular diseases) | Very High |
| 20 | Respiratory Pathology (Pneumonia, TB, COPD, Lung carcinoma) | Very High |
| 21 | Gastrointestinal Pathology (Peptic ulcer, Carcinoma stomach, IBD, Colorectal Ca) | High |
| 22 | Hepatobiliary Pathology (Hepatitis, Cirrhosis, Jaundice, Carcinoma) | Very High |
| 23 | Renal Pathology (Glomerulonephritis, Nephrotic/Nephritic, RCC, Wilms) | High |
| 24 | Endocrine Pathology (Diabetes, Thyroid, Adrenal) | High |
| 25 | Female Reproductive Pathology (Cervix, Endometrium, Ovary, Breast) | High |
| 26 | CNS Pathology (Meningitis, Gliomas, Metastasis) | Medium |
| 27 | Bone and Soft tissue tumors | Medium |
| 28 | Practical Pathology (Histology slides, Blood films, Urine analysis, LFT, RFT, TFT) | High (practical exam) |
PHASE 3 - DAY-BY-DAY TIMETABLE
PRE-FINAL PREPARATION: May 29 - June 30 (33 days)
Goal: Cover ALL General Pathology + most high-yield Systemic Pathology
Daily Pathology time: 2 hours
Book to use: Start with Harsh Mohan's Textbook of Pathology (concise, India-exam-oriented). Supplement with Robbins Basic Pathology for concepts. For quick reads: Pathoma by Dr. Husain Sattar (free videos on YouTube - HIGHLY recommended for concept building).
WEEK 1 (May 29 - June 4): Cell Injury, Death, Adaptations
| Day | Date | Topic | What to Do |
|---|---|---|---|
| 1 | May 29 (Fri) | Introduction to Pathology + Overview | Read what is pathology, types of pathology, how disease occurs. Make a 1-page overview. |
| 2 | May 30 (Sat) | Cell Injury - Causes & Mechanisms | Study reversible vs irreversible injury, free radical injury, ischemic injury. Draw the injury cascade. |
| 3 | May 31 (Sun) | FULL DAY - Cell Injury Deep Dive | Sunday = no college. Give 4-5 hours. Revise Day 1+2, then study apoptosis mechanisms in detail. |
| 4 | June 1 (Mon) | Necrosis - All types | Coagulative, liquefactive, caseous, fat necrosis, fibrinoid, gangrenous. Draw a comparison table. |
| 5 | June 2 (Tue) | Apoptosis vs Necrosis + Gangrene | Compare in a table. Wet vs dry vs gas gangrene. |
| 6 | June 3 (Wed) | Cellular Adaptations | Atrophy, hypertrophy, hyperplasia, metaplasia, dysplasia - definitions, examples, clinical significance. |
| 7 | June 4 (Thu) | Intracellular accumulations + Calcification | Fatty change (steatosis), glycogen, proteins, pigments (melanin, hemosiderin, bilirubin). Dystrophic vs metastatic calcification. |
Week 1 Revision: On Sunday June 7, spend 1 hour revising all of Week 1 before starting Week 2.
WEEK 2 (June 5 - June 11): Inflammation
| Day | Date | Topic | What to Do |
|---|---|---|---|
| 8 | June 5 (Fri) | Acute Inflammation - Vascular events | Vasodilation, increased permeability, exudate vs transudate. |
| 9 | June 6 (Sat) | Acute Inflammation - Cellular events | Margination, rolling, adhesion, diapedesis, chemotaxis. Know the molecules (selectins, integrins, ICAM). |
| 10 | June 7 (Sun) | FULL DAY - Acute Inflammation complete | Mediators of inflammation (histamine, prostaglandins, leukotrienes, complement, cytokines). Write a flowchart. |
| 11 | June 8 (Mon) | Outcomes of acute inflammation | Resolution, suppuration, organization, chronic inflammation. Exudate types. |
| 12 | June 9 (Tue) | Chronic Inflammation | Features, cells involved (macrophages, lymphocytes, plasma cells, fibroblasts), causes. |
| 13 | June 10 (Wed) | Granulomatous Inflammation | Definition, types, TB granuloma vs sarcoid vs foreign body. Draw and label a granuloma. |
| 14 | June 11 (Thu) | Wound Healing + Repair | Primary vs secondary intention, phases of healing, factors affecting, complications. |
WEEK 3 (June 12 - June 18): Hemodynamics + Shock + Neoplasia Part 1
| Day | Date | Topic | What to Do |
|---|---|---|---|
| 15 | June 12 (Fri) | Edema + Hyperemia + Congestion | Mechanisms of edema (Starling forces), types, cardiac vs renal vs hepatic edema, nutmeg liver. |
| 16 | June 13 (Sat) | Thrombosis + Embolism | Virchow's triad, thrombus vs embolus, types of emboli - pulmonary, fat, air, amniotic. |
| 17 | June 14 (Sun) | FULL DAY - Infarction + Shock | Red vs white infarcts, zones, shock types, stages of shock, organ changes in shock. |
| 18 | June 15 (Mon) | Neoplasia - Definitions + Nomenclature | Benign vs malignant, naming conventions, differences in a comparison table. |
| 19 | June 16 (Tue) | Carcinogenesis | Chemical, radiation, viral carcinogenesis. Oncogenes, tumor suppressor genes (TP53, Rb). |
| 20 | June 17 (Wed) | Tumor spread + Grading + Staging | Local invasion, lymphatic, hematogenous. TNM staging, grading systems. |
| 21 | June 18 (Thu) | Tumor markers + Paraneoplastic syndromes | AFP, CEA, PSA, CA-125, CA 19-9, BHCG. Paraneoplastic: PTHrP, SIADH, ACTH. |
WEEK 4 (June 19 - June 25): Immunopathology + Genetic Disorders + Hematology
| Day | Date | Topic | What to Do |
|---|---|---|---|
| 22 | June 19 (Fri) | Hypersensitivity Type I & II | Anaphylaxis, atopy, cytotoxic reactions, examples for each. |
| 23 | June 20 (Sat) | Hypersensitivity Type III & IV + Autoimmunity | Immune complex (SLE), delayed type (TB test), autoimmune diseases, SLE criteria. |
| 24 | June 21 (Sun) | FULL DAY - Amyloidosis + Genetic disorders | Amyloid types, Congo red stain, apple-green birefringence. Down, Turner, Klinefelter, Marfan, NF. |
| 25 | June 22 (Mon) | Anemias - Classification + IDA | Classify by MCV, by mechanism. Iron deficiency anemia - causes, blood picture, treatment. |
| 26 | June 23 (Tue) | Megaloblastic anemia + Hemolytic anemias | B12/Folate deficiency, hypersegmented neutrophils. Sickle cell, thalassemia, G6PD, hereditary spherocytosis. |
| 27 | June 24 (Wed) | Aplastic anemia + Leukemias overview | Aplastic anemia pathogenesis. ALL vs AML vs CLL vs CML - key differences, auer rods, Philadelphia chromosome. |
| 28 | June 25 (Thu) | Lymphomas | Hodgkin (RS cell, subtypes) vs Non-Hodgkin. |
WEEK 5 (June 26 - June 30): High-yield Systemic for Pre-final
| Day | Date | Topic | What to Do |
|---|---|---|---|
| 29 | June 26 (Fri) | Cardiovascular - Atherosclerosis + MI | Pathogenesis of atherosclerosis, MI zones, complications. |
| 30 | June 27 (Sat) | Respiratory - Pneumonia + TB | Lobar vs bronchopneumonia, TB pathology, ghon complex, military TB. |
| 31 | June 28 (Sun) | FULL DAY - Liver Pathology + Hepatitis | Hepatitis types, chronicity, cirrhosis, portal hypertension, jaundice types. |
| 32 | June 29 (Mon) | GIT Pathology | Peptic ulcer, gastric carcinoma, IBD (Crohn vs UC table), colorectal carcinoma. |
| 33 | June 30 (Tue) | PRE-FINAL RAPID REVISION | Only flowcharts, comparison tables, diagrams. No new reading. |
Pre-final is roughly July 1st week. After June 30, the first 2-3 days of July are pure revision and past paper practice.
JULY - AFTER PRE-FINAL: Complete Systemic Pathology (July 10 - August 15)
Once pre-final is done, you get a few days break, then resume with full SP coverage.
| Week | Dates | Topics |
|---|---|---|
| Week 1-post | July 10-16 | Renal pathology (GN, nephrotic/nephritic, RCC, Wilms) |
| Week 2-post | July 17-23 | Endocrine (DM types, thyroid disorders, adrenal) |
| Week 3-post | July 24-30 | Female reproductive + Breast pathology |
| Week 4-post | July 31-Aug 6 | CNS pathology + Bone tumors |
| Week 5-post | Aug 7-15 | CVRS/Respiratory full revision + Practical pathology (slides, blood films) |
AUGUST 16 - SEPTEMBER 1: Final Exam Revision Sprint
- Week 1: Revise ALL General Pathology (notes only, no rereading)
- Week 2: Revise ALL Systemic Pathology with past papers
- Week 3: Mock self-tests, writing practice, important diagrams
- Final 3-4 days: Only flashcard-style revision of key facts
PHASE 4 - HOW TO ACTUALLY STUDY EACH TOPIC
This is the most important part - the method that builds concepts, not just rote learning.
The 4-Step System for Every Topic
Step 1 - Watch first (15-20 min)
Before opening any book, watch the Pathoma/YouTube video on that topic. It activates your interest and gives a framework. Recommended channels: Pathoma (Husain Sattar), Armando Hasudungan, Ninja Nerd Pathology.
Step 2 - Read once actively (45-60 min)
Open Harsh Mohan. Read the chapter. As you read, UNDERLINE only definitions and mechanisms. Do NOT highlight everything. Write in the margin: "Why does this happen?" and try to answer it.
Step 3 - Make a flowchart or table (15-20 min)
Right after reading, close the book and draw a flowchart from memory. For example, after reading acute inflammation, draw the full vascular + cellular events as a cascade. This single habit separates toppers from average students.
Step 4 - Write 5 key points (5 min)
Write 5 facts you must not forget. Keep these in a small notebook. Review this notebook every Sunday.
PHASE 5 - CONCEPT-BUILDING SHORTCUTS
Most Important Concepts for KNRUHS Exams (these come every year):
- Cell injury cascade - draw it until you can do it in 2 minutes
- Virchow's triad - always comes with clinical scenarios
- Types of necrosis - with examples, very high yield
- Granuloma - definition + draw a labeled granuloma (TB vs sarcoid)
- Apoptosis pathway - intrinsic vs extrinsic with caspases
- Hypersensitivity types - table with examples (comes EVERY year)
- TP53 and cell cycle - for neoplasia understanding
- Blood film descriptions - for practical exams
- Comparison tables - always: Crohn vs UC, Hodgkin vs NHL, Nephrotic vs Nephritic, Type 1 vs Type 2 DM
Diagrams you MUST be able to draw:
- Granuloma (labeled)
- Wound healing (primary + secondary intention)
- Coagulation cascade (connects with hemodynamics)
- Leukemia classification tree
- Portal hypertension consequences
PHASE 6 - PHARMACOLOGY + MICROBIOLOGY PARALLEL PLAN
Since you only have 1 hour for Pharma and 45 min for Micro per day, here is how to prioritize:
Pharmacology (1 hour/day, 5 PM - 6 PM):
Follow the same weekly cycle but cover system-by-system matching patho:
- When studying cardiovascular patho → study anti-hypertensives, anti-anginals
- When studying respiratory patho → study bronchodilators, steroids
- When studying hematology → study iron, B12, folate, anticoagulants This creates cross-linking between subjects, which is the fastest way to learn.
Microbiology (45 min/day, 9 PM):
Follow organ-system matching too:
- Respiratory week in patho → study TB, pneumococcal pneumonia, influenza in micro
- Liver week in patho → study Hepatitis viruses (A, B, C, E) in micro
- GIT week in patho → study H. pylori, Salmonella, Shigella in micro
PHASE 7 - PRACTICAL PATHOLOGY
Your practical exam will test:
- Histology slides - know the basic 10 slides (TB, carcinoma, hepatitis, fibroadenoma, etc.)
- Blood films - IDA (hypochromic microcytic), megaloblastic (macro-ovalocytes, hypersegmented neutrophils), sickle cell, malaria
- Urine analysis - RBC casts (GN), granular casts, bilirubin
- Spot specimens - Kidney (hydronephrosis, stones), liver (cirrhosis, nutmeg), spleen, lung
Practical study: During college practical hours (9-5), pay 100% attention. Draw slides in your practical record book with proper labels. This is often neglected by students but the practical mark adds directly to your final score.
QUICK REFERENCE - TIMELINE SUMMARY
May 29 → June 7 : General Pathology Block 1 (Cell injury, Death, Adaptations)
June 8 → June 14 : General Pathology Block 2 (Inflammation, Healing)
June 15 → June 21 : General Pathology Block 3 (Hemodynamics, Neoplasia)
June 22 → June 30 : Immunopathology + Hematology + High-yield Systemic
July 1st week : PRE-FINAL EXAM
July 10 → Aug 15 : Complete Systemic Pathology
Aug 16 → Sept 1 : Final Exam Revision Sprint
Sept 1st week : FINAL EXAM
FINAL TIPS SPECIFICALLY FOR YOU
-
Do NOT try to read Robbins cover to cover. Use Harsh Mohan as your primary text. Use Robbins only when you need to understand a mechanism better.
-
Sunday is your power day. No college = use it for 4-5 hours. This one day every week can cover 2 normal days of content.
-
Write, do not just read. Every important mechanism should be written out as a flowchart at least once. Writing creates stronger memory than reading.
-
Past papers are gold. After July, solve the last 5 years of KNRUHS Pathology papers. Most questions repeat. The pattern will become obvious.
-
The morning 30-min slot is sacred. Every morning, just rewrite yesterday's 5-point notes without looking at them. This is spaced repetition and it dramatically reduces forgetting.
-
Do not skip practical classes. In Indian universities, the practical viva and internal marks make up a significant portion. Every slide you observe properly in college saves you 30 minutes of studying at home.
-
For concept clarity: Pathoma videos by Husain Sattar (available on YouTube) are the single best free resource for building pathology concepts. They are specifically designed to explain mechanisms, not just list facts. Watch the video before you read the chapter.
If you want, I can go deeper on any specific topic (like cell injury, inflammation, or neoplasia), build detailed notes for a particular chapter, or create a shorter "cheat sheet" for high-yield exam facts. Just ask!
Let's start pathology now
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is your complete Day 1 lesson, taught just like a teacher would - with concepts, images, and notes directly from Robbins Basic Pathology.
📚 DAY 1 - PATHOLOGY LESSON
Introduction to Pathology + Cell Injury
Tonight's goal: Read this fully, draw the flowchart at the end, and write your 5 key points in your notebook.
PART 1 - WHAT IS PATHOLOGY?
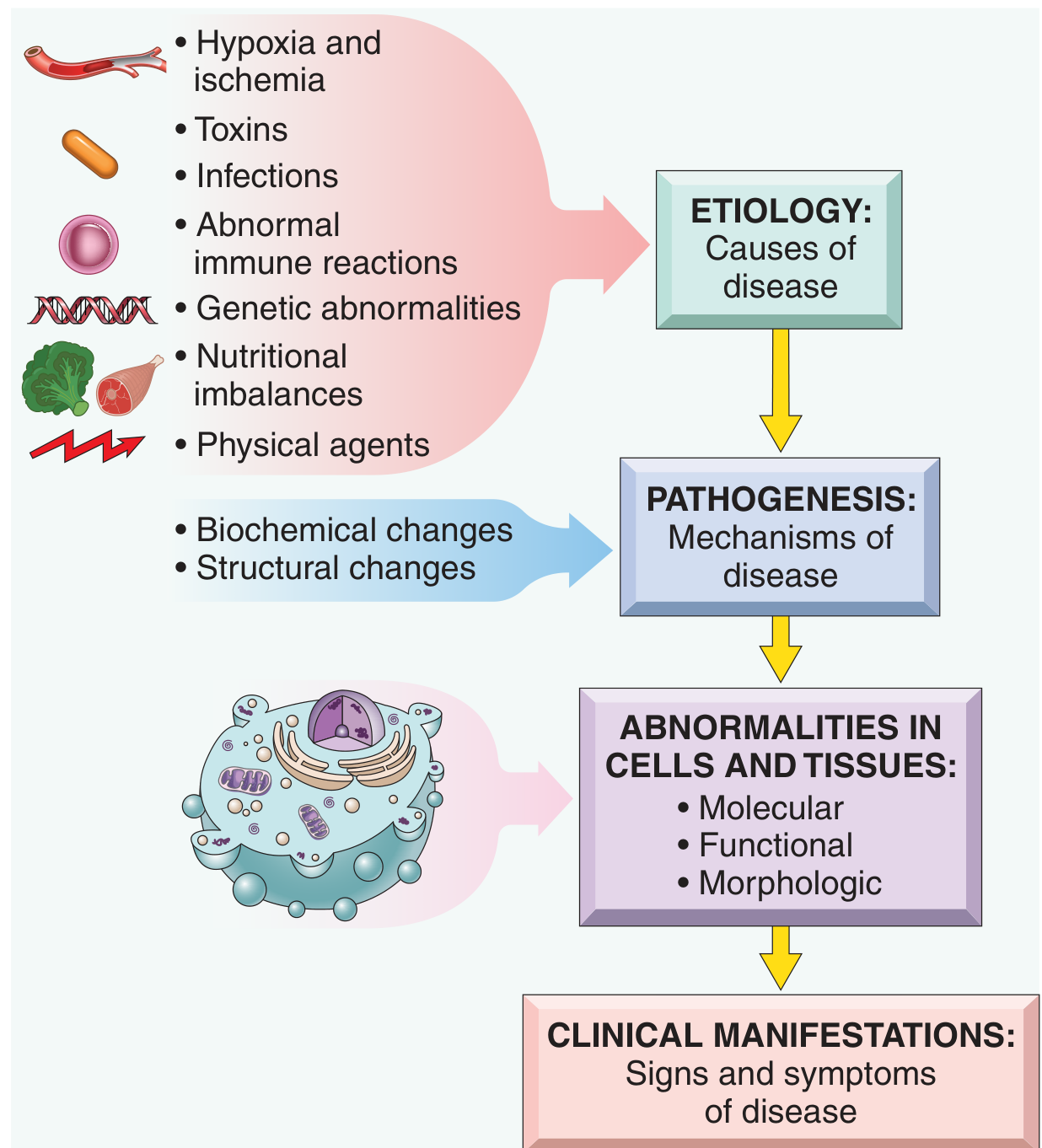
Pathology is the scientific study of the causes and mechanisms of disease - specifically the changes in cells, tissues, and organs that arise as diseases develop.
There are two words you must know perfectly because examiners love them:
| Term | Definition | Memory trick |
|---|---|---|
| Etiology | The cause (origin) of disease - what triggers it | Etiology = "E" for "Elicit/cause" |
| Pathogenesis | The mechanism - how disease develops step by step after the trigger | Patho = disease, genesis = origin/development |
Here is the classic Robbins diagram showing how disease goes from cause to clinical symptoms:
Example to make this concrete:
- Etiology of TB = Mycobacterium tuberculosis (the bacteria is the CAUSE)
- Pathogenesis of TB = bacteria enters lung → macrophages engulf it → granuloma forms → caseous necrosis → cavitation (this is the HOW)
- Clinical manifestations = cough, hemoptysis, weight loss, fever
The 4 aspects of disease that pathology studies:
- Etiology - cause
- Pathogenesis - mechanism of development
- Morphologic changes - structural changes in cells/tissues (what you see under microscope)
- Clinical significance - functional consequences (signs and symptoms)
PART 2 - OVERVIEW OF CELLULAR RESPONSES TO STRESS
This is the foundation of ALL pathology. Before a cell dies or gets injured, it first tries to survive. Here is the spectrum of cellular responses:
Normal Cell
|
↓ Stress/Stimulus
|
├──── ADAPTATION (cell survives, adjusts)
| Examples: hypertrophy, hyperplasia, atrophy, metaplasia
|
├──── REVERSIBLE INJURY (cell is damaged but can recover)
| If stress is removed → cell recovers
|
└──── IRREVERSIBLE INJURY → CELL DEATH
Two main types:
├── NECROSIS (pathological death)
└── APOPTOSIS (programmed death)
Key concept: The outcome depends on TWO things - the severity of the stress AND the duration of the stress.
PART 3 - CAUSES OF CELL INJURY
The major causes grouped into 6 categories (memorize this list - it appears in every exam):
| # | Cause | Examples |
|---|---|---|
| 1 | Hypoxia & Ischemia | Most common cause! Block in artery, anemia, lung disease |
| 2 | Toxins | Alcohol, carbon monoxide, drugs, insecticides, asbestos |
| 3 | Infectious agents | Bacteria (toxins), viruses, fungi, parasites |
| 4 | Immunologic reactions | Autoimmune, allergic, chronic immune responses |
| 5 | Genetic abnormalities | Down syndrome, sickle cell disease, enzyme deficiencies |
| 6 | Nutritional imbalances | Protein-calorie malnutrition, vitamin deficiencies, obesity |
| 7 | Physical agents | Trauma, heat, cold, radiation, electric shock |
Exam tip: "Hypoxia is the most common cause of cell injury." This line gets marks in every short answer.
Difference: Hypoxia vs Ischemia
- Hypoxia = oxygen deficiency only (supply of nutrients is maintained)
- Ischemia = reduced blood supply (so BOTH oxygen AND nutrients are lost)
- Therefore, ischemia causes injury faster and more severely than pure hypoxia
PART 4 - SEQUENCE OF EVENTS IN CELL INJURY
When a cell is injured, events happen in a specific sequence:
Step 1 - Reversible Cell Injury (the cell can still recover)
When injury first occurs, you see these changes under the microscope:
- Cellular swelling (most common and earliest change) - Na+/K+ pump fails → Na+ enters → water follows → cell swells
- Fatty change - lipids accumulate in cytoplasm (especially liver and heart cells)
- Under light microscope: cytoplasm looks pale and granular, vacuoles may appear
Why does swelling happen?
Injury → ATP decreases → Na+/K+-ATPase pump fails → Na+ accumulates inside cell → water enters by osmosis → cell swells. This is called hydropic change or cloudy swelling.
Step 2 - Point of No Return (Irreversible Injury)
Two main events mark the point where injury becomes irreversible:
- Severe mitochondrial damage (mitochondrial permeability transition pore opens) - no more ATP can be made
- Massive membrane damage - lysosomal contents leak out, digesting the cell from inside
Once these two events happen, the cell cannot recover regardless of removing the injury.
PART 5 - THE 4 MAIN MECHANISMS OF CELL INJURY
This is the most concept-heavy part. Here is the Robbins diagram explaining it:
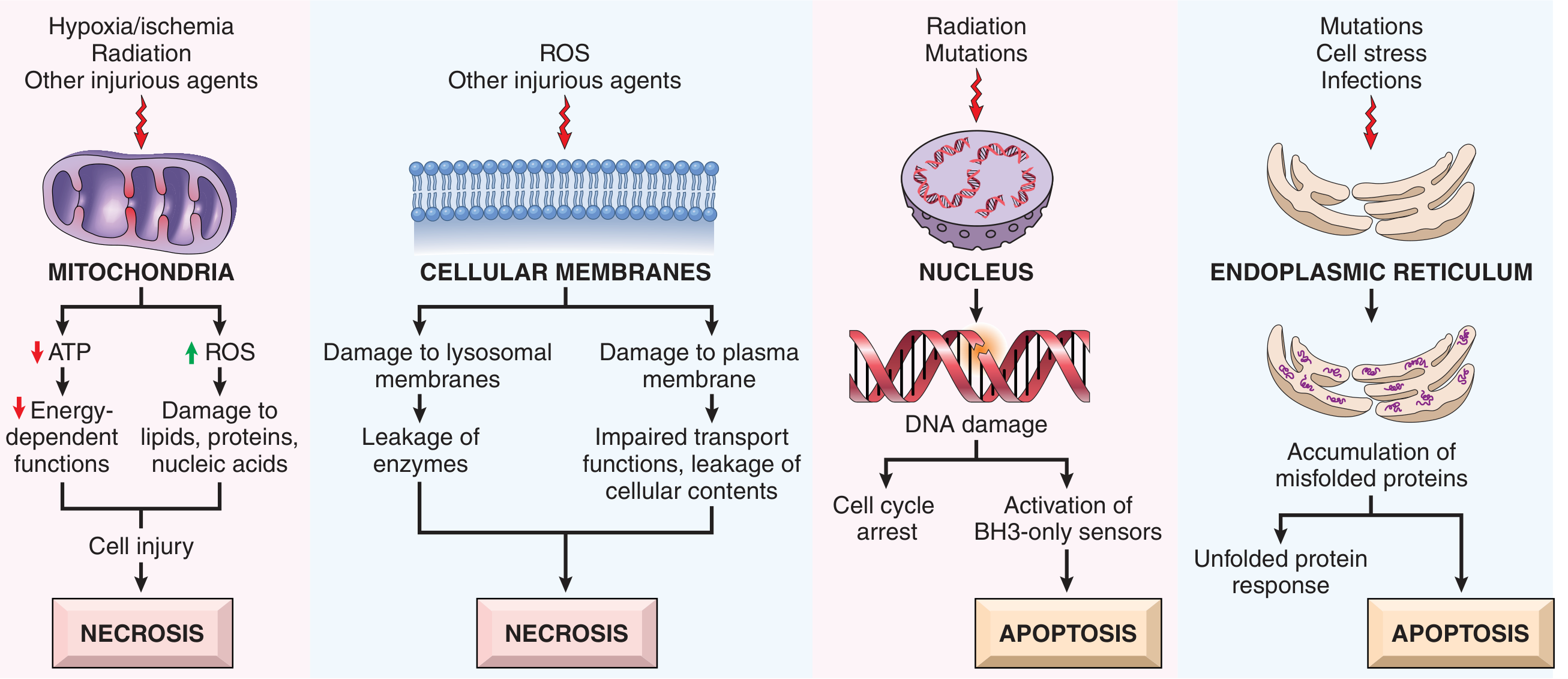
Mechanism 1 - Mitochondrial Dysfunction
- Injury → mitochondria damaged → ATP falls
- Without ATP: Na+/K+ pump fails → cell swells; Ca2+ builds up; cell membrane fails
- Also: damaged mitochondria generate Reactive Oxygen Species (ROS) - free radicals that damage everything
- Mitochondrial permeability transition pore opens → membrane potential lost → complete energy failure → NECROSIS
Mechanism 2 - Membrane Damage
- Damage to plasma membrane → cells cannot maintain ion gradients → swelling and death
- Damage to lysosomal membrane → lysosomal enzymes (acid hydrolases) leak → digest the cell from inside → NECROSIS
Mechanism 3 - DNA Damage
- Radiation, mutations, free radicals damage DNA
- Cell detects DNA damage → tries to repair → if too severe → apoptosis pathway activated
- Key molecule: p53 protein - the "guardian of the genome" - detects DNA damage and triggers apoptosis
Mechanism 4 - Endoplasmic Reticulum (ER) Stress
- Mutations, infections, cell stress → misfolded proteins accumulate in ER
- ER activates the unfolded protein response (UPR)
- If overwhelmed → triggers APOPTOSIS
PART 6 - REACTIVE OXYGEN SPECIES (ROS) / FREE RADICALS
This topic comes every year in theory and viva.
What are free radicals?
Molecules with an unpaired electron in the outer orbital. This makes them extremely reactive - they attack lipids, proteins, and DNA.
The 3 main ROS and how they form:
O₂ + incomplete reduction
↓
Superoxide (O₂⁻) ← most common initial ROS
↓ [superoxide dismutase = SOD]
Hydrogen peroxide (H₂O₂) ← can cross membranes
↓ [Fe²⁺ via Fenton reaction]
Hydroxyl radical (•OH) ← MOST DANGEROUS
How does the body neutralize ROS?
| Antioxidant mechanism | What it does |
|---|---|
| Superoxide dismutase (SOD) | Converts O₂⁻ → H₂O₂ |
| Catalase | Converts H₂O₂ → H₂O + O₂ |
| Glutathione peroxidase | Destroys H₂O₂ and lipid peroxides |
| Vitamin C | Scavenges free radicals |
| Vitamin E | Protects lipid membranes from oxidation |
When are ROS produced in excess?
- Reperfusion injury (when blood returns after ischemia - paradoxically causes MORE damage)
- Inflammation (neutrophils deliberately make ROS to kill bacteria)
- Radiation
- Aging
- Toxins (CCl₄ - carbon tetrachloride, paracetamol overdose)
PART 7 - CALCIUM AND CELL INJURY
Calcium is a silent killer in injured cells:
- Normal: cytosol Ca²⁺ is very LOW (kept in ER and mitochondria)
- Injury → Ca²⁺ floods cytosol
- Excess Ca²⁺ activates destructive enzymes:
- Phospholipases → destroy membranes
- Proteases → degrade proteins
- ATPases → deplete energy
- Endonucleases → cut DNA
QUICK SUMMARY - YOUR 5 KEY POINTS TO WRITE IN YOUR NOTEBOOK TONIGHT
Copy these exactly into your notebook:
- Pathology = Etiology (WHY) + Pathogenesis (HOW) + Morphology (WHAT) + Clinical significance (WHAT HAPPENS)
- Earliest change in reversible injury = Cellular swelling (due to Na+/K+-ATPase failure from ATP depletion)
- Point of no return = severe mitochondrial damage + massive membrane damage (lysosomal enzyme leak)
- 4 mechanisms of cell injury: Mitochondrial dysfunction, Membrane damage, DNA damage, ER stress
- Most common cause of cell injury = Hypoxia/Ischemia. Most dangerous ROS = Hydroxyl radical (•OH)
SELF-TEST QUESTIONS (do these after reading - close your notes and answer)
- What is the difference between etiology and pathogenesis? Give an example.
- What is the FIRST and EARLIEST morphologic change in reversible cell injury?
- Why does calcium accumulation lead to cell death? Name 4 enzymes activated.
- Name the 3 main ROS in order of formation. Which enzyme converts O₂⁻ to H₂O₂?
- Why does ischemia cause faster injury than pure hypoxia?
TOMORROW (Day 2) - CELL DEATH: Necrosis + Apoptosis
You will learn:
- The 6 types of necrosis with their classic examples
- What necrotic cells look like under the microscope (pyknosis, karyorrhexis, karyolysis)
- Apoptosis - what it is, when it happens, and how it differs from necrosis
Source: Robbins & Kumar Basic Pathology (Robbins Pathology), Chapter 1
Great start! You've covered the entire conceptual foundation for all of pathology. Draw the cell injury cascade flowchart (normal cell → stress → adaptation/reversible injury/irreversible injury → necrosis/apoptosis) on paper before sleeping. That one diagram ties everything together.
Ready for Day 2 tomorrow, or want me to go deeper into any part of today's lesson?
This is a shared conversation. Sign in to Orris to start your own chat.