
Explain this and also whole arterial supply
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching Images
abdominal aorta branches celiac SMA IMA arterial supply GI tract
Reading File
Reading File
Reading File
Loading Image
Here is a full explanation of everything shown in your textbook image, plus the complete arterial supply of the GI tract.
What Your Textbook Page Shows
1. Abdominal Aorta and Branches Diagram (top)
The diagram illustrates the three unpaired anterior branches of the abdominal aorta that supply the GI tract:
| Artery | Embryonic Origin | Territory Supplied |
|---|---|---|
| Celiac trunk | Foregut | Lower esophagus → proximal duodenum (D1, D2 proximal half) + liver, gallbladder, spleen, pancreas |
| Superior Mesenteric Artery (SMA) | Midgut | Distal duodenum → proximal 2/3 of transverse colon |
| Inferior Mesenteric Artery (IMA) | Hindgut | Distal 1/3 transverse colon → upper rectum |
The key rule shown on your page:
- GI arteries branch anteriorly (toward the gut)
- Non-GI arteries (renal, gonadal, etc.) branch laterally or posteriorly
2. Watershed Areas (Highlighted Boxes)
Two zones in the colon receive dual blood supply from the distal ends of two arterial territories — these "watershed" zones have the least collateral flow and are most vulnerable to ischemia:
Splenic Flexure (Griffith's Point) — SMA meets IMA
- The left branch of the middle colic artery (SMA) meets the ascending branch of the left colic artery (IMA)
- This is the most clinically important watershed — susceptible to ischemic colitis in shock, emboli, or atherosclerosis
Rectosigmoid Junction (Sudeck's Point) — IMA meets Internal Iliac
- The last sigmoid artery (IMA branch) meets the superior rectal artery (IMA) and middle/inferior rectal arteries (internal iliac = hypogastric artery)
- Vulnerable after IMA ligation in aortic aneurysm repair
These areas become ischemic first in states of hypoperfusion, thromboembolism, or atherosclerosis — the mucosa sloughs, risking perforation and sepsis.
3. Nutcracker Syndrome (middle panel)
Compression of the left renal vein between the SMA (anteriorly) and the aorta (posteriorly) — like a nutcracker.
Consequences:
- Left renal vein becomes dilated/hypertensive
- Gross hematuria (rupture of thin-walled renal varicosities into the collecting system)
- Abdominal/flank pain
- Left-sided varicocele (because the left testicular/ovarian vein drains into the left renal vein, not directly into the IVC — so raised pressure backs up)
4. Superior Mesenteric Artery (SMA) Syndrome (bottom panel)
SMA and aorta compress the transverse (3rd) portion of the duodenum — the duodenum passes between these two structures.
Causes: Loss of the mesenteric fat pad that normally cushions this angle:
- Rapid weight loss
- Malnutrition
- Gastric bypass surgery
- Low body weight
Symptoms: Intermittent postprandial abdominal pain, nausea, vomiting — classic intermittent intestinal obstruction pattern.
Complete Arterial Supply of the GI Tract
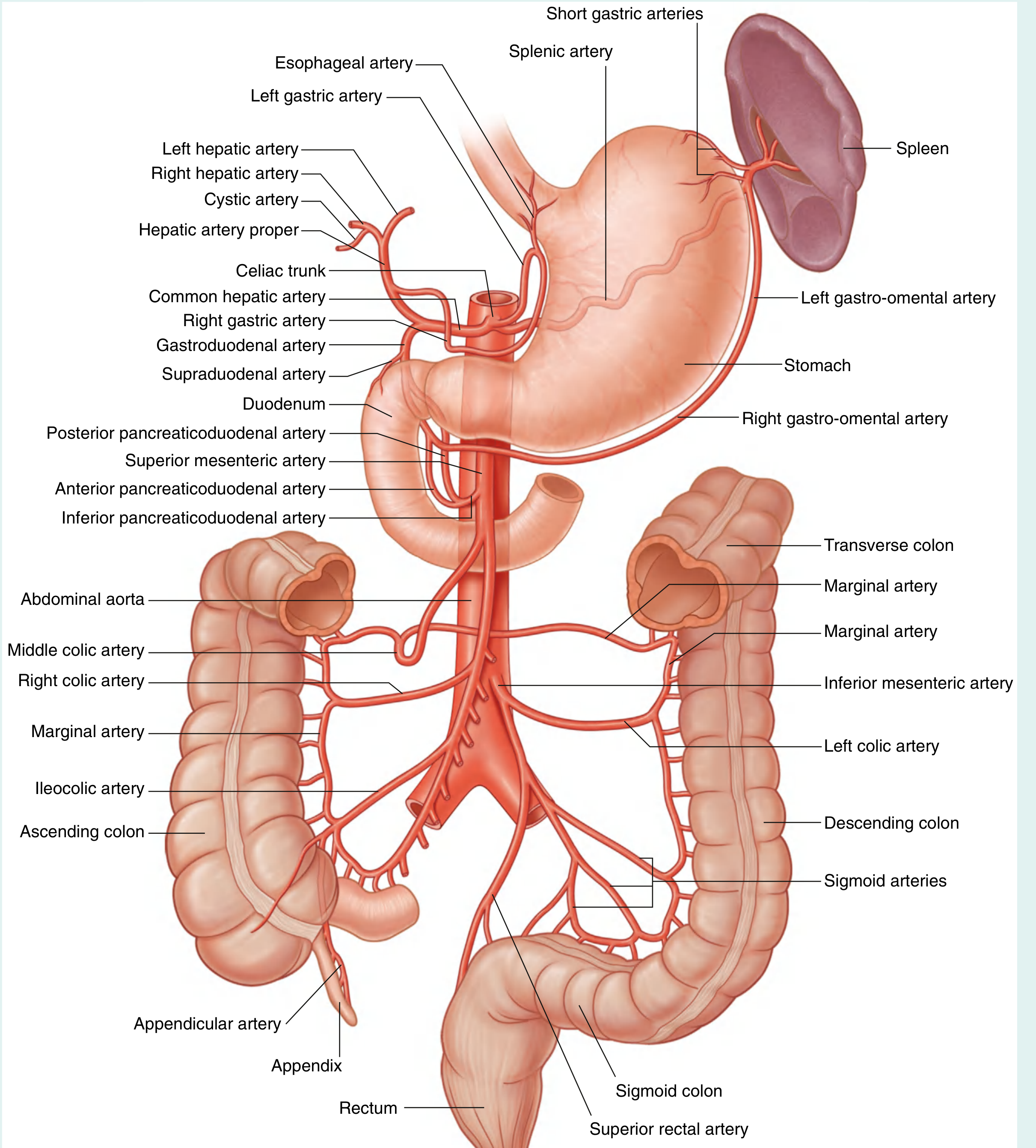
🔴 CELIAC TRUNK (T12 level) — Foregut
Arises from the aorta at T12/L1, trifurcates immediately:
A. Left Gastric Artery
- Supplies the lesser curvature of the stomach + lower esophagus
- Anastomoses with the right gastric artery
B. Splenic Artery
- Tortuous course along the upper border of the pancreas → spleen
- Gives off: short gastric arteries (to fundus), left gastro-omental artery (to greater curvature)
- Also gives pancreatic branches (dorsal pancreatic, pancreatica magna)
C. Common Hepatic Artery → divides into:
- Hepatic artery proper → right & left hepatic arteries → liver + cystic artery (to gallbladder)
- Right gastric artery → lesser curvature of stomach, anastomoses with left gastric
- Gastroduodenal artery → divides into:
- Superior pancreaticoduodenal artery (anterior + posterior) → head of pancreas + duodenum D1/D2
- Right gastro-omental artery → greater curvature of stomach, anastomoses with left gastro-omental
🔴 SUPERIOR MESENTERIC ARTERY (L1) — Midgut
Arises just below the celiac trunk, passes behind the neck of the pancreas and over the 3rd part of the duodenum.
First branch: Inferior pancreaticoduodenal artery → anastomoses with superior pancreaticoduodenal (from celiac) — supplies head of pancreas and distal duodenum
Left-side branches (small bowel):
- Jejunal arteries (4–6): form 1–2 arcades, long vasa recta
- Ileal arteries (9–13): form 3–5 arcades, short vasa recta
- → These form the arterial arcades → vasa recta (straight terminal vessels to gut wall)
Right-side branches (large bowel):
- Middle colic artery → transverse colon (right + left branches)
- Right colic artery (sometimes absent) → ascending colon
- Ileocolic artery → terminal ileum, cecum, appendix (via appendicular artery), proximal ascending colon
🔴 INFERIOR MESENTERIC ARTERY (L3) — Hindgut
Smallest of the three. Arises at L3, descends to the left.
- Left colic artery → descending colon; ascending branch anastomoses with middle colic (SMA) at splenic flexure
- Sigmoid arteries (2–4) → sigmoid colon, lowest descending colon
- Superior rectal artery → upper and middle rectum; anastomoses with middle rectal (internal iliac) and inferior rectal (internal pudendal) arteries at the rectosigmoid junction
Collateral Connections — Clinically Critical
| Anastomosis | Between | Location |
|---|---|---|
| Pancreaticoduodenal arcade | Celiac ↔ SMA | Head of pancreas / duodenum |
| Marginal artery of Drummond | SMA ↔ IMA | Along entire colon wall |
| Arc of Riolan (meandering mesenteric) | SMA ↔ IMA | Central/medial route via middle + left colic |
| Rectal anastomosis | IMA ↔ Internal iliac | Rectum |
The marginal artery of Drummond runs continuously along the mesenteric border of the entire colon and is the key collateral route when the IMA is occluded (e.g., in aortic aneurysm repair).
Key rule for exams: GI supply follows embryonic gut origin — Celiac = Foregut, SMA = Midgut, IMA = Hindgut. The watershed zones (splenic flexure and rectosigmoid junction) mark the borders between these territories and are the first to suffer ischemia.
— Gray's Anatomy for Students, p. 413–416

Explain this along with whole arterial and nerve supply
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Searching Images
nerve supply GI tract autonomic innervation enteric nervous system diagram
Reading File
Reading File
Loading Image
Loading Image
Loading Image
This is the same page as before (page 370 from First Aid / a step-1 style review book), now with your handwritten annotations highlighting key features. Here is the full explanation plus the complete arterial and nerve supply.
Your Textbook Page — What's Highlighted
Your annotations circle/underline three things on Nutcracker syndrome: abdominal (flank) pain, hematuria, and varicocele — these are the classic triad. The SMA syndrome box underlines postprandial pain as the key symptom. These were covered in our previous session — see below for the same explanations plus the nerve supply you've now asked for.
PART 1: Arterial Supply of the GI Tract
(Already covered in detail — summary here for completeness)
Three Unpaired Anterior Branches of the Abdominal Aorta
| Artery | Level | Embryonic Territory | Structures Supplied |
|---|---|---|---|
| Celiac Trunk | T12 | Foregut | Lower esophagus → proximal D2; liver, gallbladder, spleen, pancreas |
| SMA | L1 | Midgut | Distal D2 → proximal 2/3 transverse colon |
| IMA | L3 | Hindgut | Distal 1/3 transverse colon → upper rectum |
Key rule: GI arteries branch anteriorly; non-GI arteries (renal, gonadal, lumbar) branch laterally/posteriorly.
Celiac Trunk Branches
- Left gastric → lesser curvature of stomach + lower esophagus
- Splenic artery → spleen, short gastric arteries (fundus), left gastro-omental (greater curvature)
- Common hepatic → hepatic artery proper (liver, cystic artery), right gastric, gastroduodenal artery → superior pancreaticoduodenal + right gastro-omental
SMA Branches
- Inferior pancreaticoduodenal → pancreatic head + distal duodenum (anastomoses with celiac territory)
- Jejunal & ileal arteries → arcades → vasa recta
- Middle colic → transverse colon
- Right colic → ascending colon
- Ileocolic → terminal ileum, cecum, appendix (appendicular artery)
IMA Branches
- Left colic → descending colon; anastomoses with middle colic at splenic flexure
- Sigmoid arteries (2–4) → sigmoid colon
- Superior rectal → upper rectum; anastomoses with middle/inferior rectal (internal iliac) at rectosigmoid junction
Watershed (Ischemia-Prone) Zones
| Zone | Meeting Arteries | Vulnerability |
|---|---|---|
| Splenic flexure (Griffith's point) | SMA ↔ IMA | Most vulnerable — first to infarct in shock |
| Rectosigmoid junction (Sudeck's point) | IMA ↔ Internal iliac (hypogastric) | Vulnerable after IMA ligation |
PART 2: Nerve Supply of the GI Tract
The gut has three layers of neural control working together:
Layer 1 — Enteric Nervous System (ENS) = "The Little Brain of the Gut"
The ENS is intrinsic — it can function completely independently of the CNS. It contains ~100 million neurons (as many as the spinal cord).
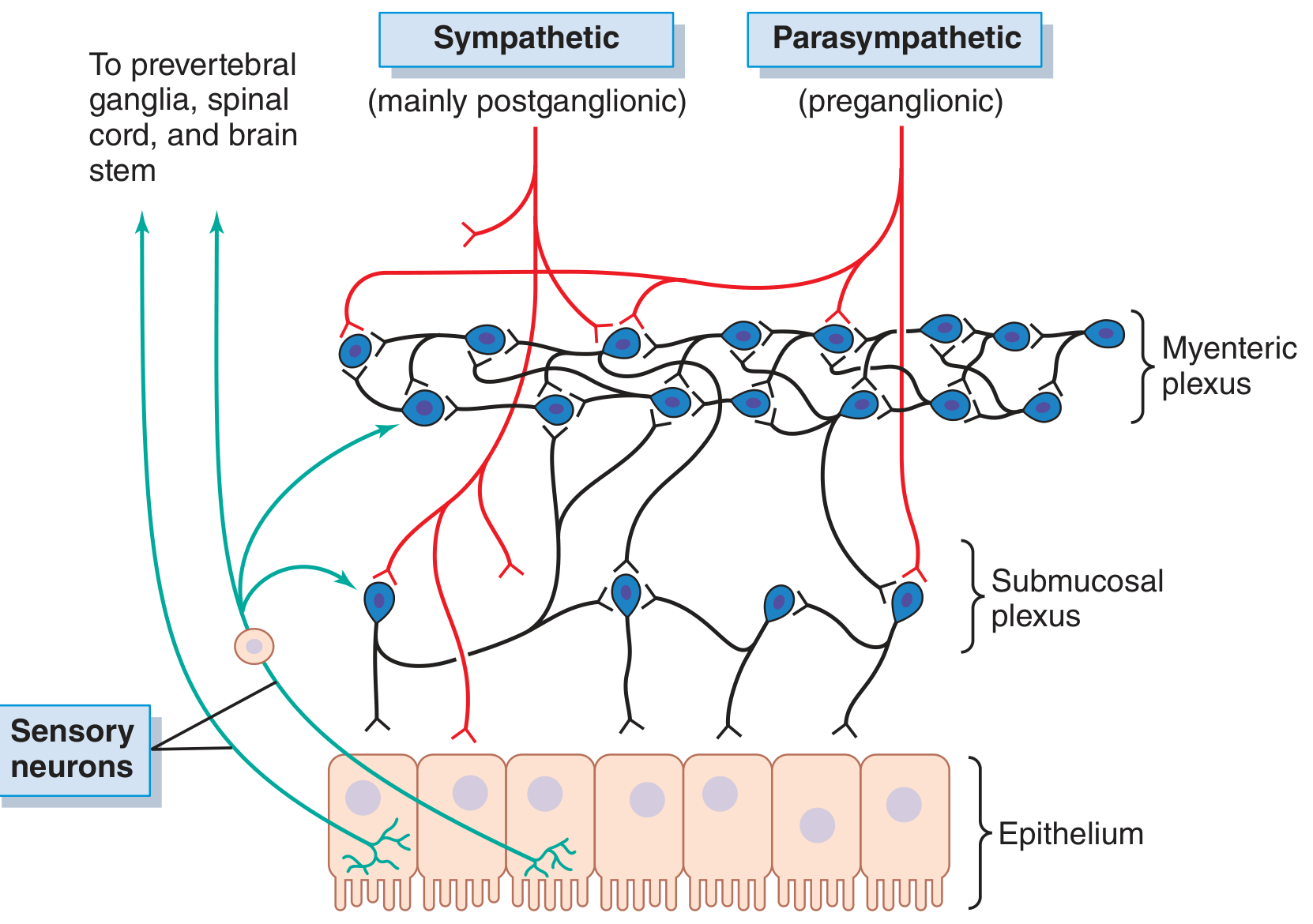
Two Plexuses:
| Plexus | Location | Function |
|---|---|---|
| Myenteric (Auerbach) plexus | Between longitudinal and circular muscle layers | Controls motility (peristalsis, tone, rate of contractions) |
| Submucosal (Meissner) plexus | In the submucosa | Controls secretion, absorption, mucosal blood flow |
Neurotransmitters:
- Excitatory: Acetylcholine, Substance P, Glutamate
- Inhibitory: Nitric oxide (NO), VIP (vasoactive intestinal peptide), Somatostatin, ATP
The ENS also has pacemaker cells — Interstitial Cells of Cajal (ICC) — which generate intrinsic electrical rhythms (slow waves) that coordinate smooth muscle contraction.
Layer 2 — Parasympathetic Supply (Excitatory — "rest and digest")
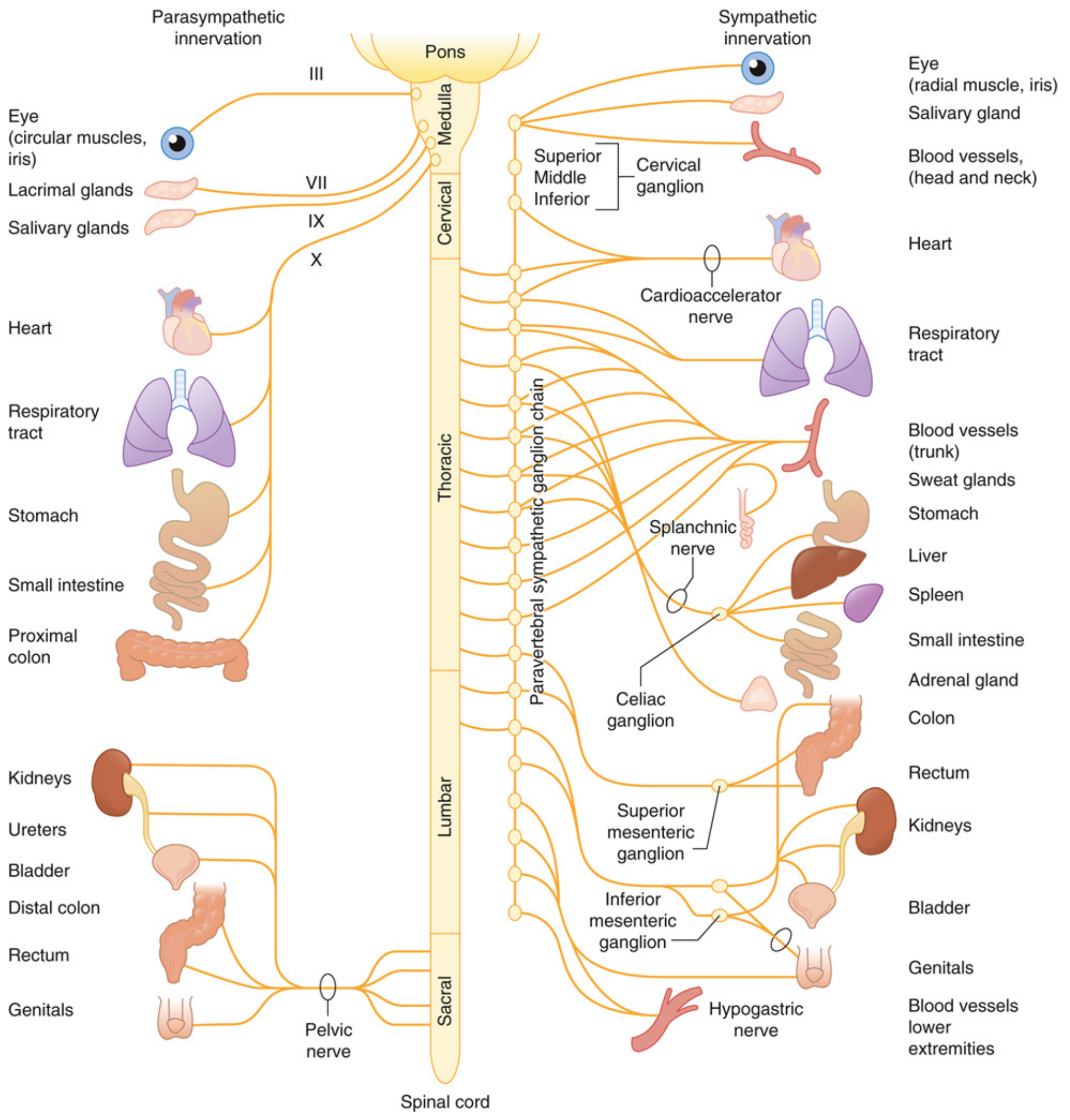
Cranial part — Vagus nerve (CN X):
- Supplies: esophagus → proximal 2/3 of transverse colon (foregut + midgut)
- Preganglionic fibers synapse in the myenteric and submucosal plexuses (ganglia in the gut wall)
- Effects: ↑ peristalsis, ↑ secretion, sphincter relaxation
Sacral part — Pelvic splanchnic nerves (S2–S4):
- Supplies: distal 1/3 transverse colon → rectum (hindgut)
- Also called nervi erigentes
- Synapse in the wall of the organ itself (very short postganglionic fibers)
The transition from vagal to sacral parasympathetic supply corresponds roughly to the splenic flexure — the same watershed zone for arterial supply.
Layer 3 — Sympathetic Supply (Inhibitory — "fight or flight")
Origin: Thoracolumbar spinal cord (T5–L3)
Preganglionic fibers → travel via splanchnic nerves → synapse in prevertebral ganglia
| Prevertebral Ganglion | Spinal Level | Splanchnic Nerve | Organs Supplied |
|---|---|---|---|
| Celiac ganglion | T5–T9 | Greater splanchnic | Stomach, liver, pancreas, small bowel, proximal colon |
| Superior mesenteric ganglion | T9–T12 | Lesser splanchnic | Small bowel + proximal colon (with celiac) |
| Inferior mesenteric ganglion | T11–L1 | Lumbar splanchnic | Distal colon, sigmoid, rectum |
Postganglionic fibers travel along blood vessels (periarteriolar plexuses) to reach the gut wall.
Sympathetic effects on the gut:
- ↓ peristalsis and secretion
- ↑ sphincter tone (closes gut down)
- Vasoconstriction of gut blood vessels
- Transmits visceral pain (via sympathetic afferents → DRG → spinal cord)
This is why visceral pain is diffuse and poorly localized — afferent fibers travel with sympathetic nerves through multiple spinal levels.
Visceral Innervation Summary Table
(From Miller's Anesthesia)
| Organ | Sympathetic (Pain) | Parasympathetic |
|---|---|---|
| Stomach | T7–T9 via Celiac plexus | Vagus nerve |
| Liver & biliary tract | T5–T10 via Celiac plexus | Vagus nerve |
| Pancreas | T6–T10 via Celiac plexus | Vagus nerve |
| Small bowel | T9–L1 via Celiac plexus | Vagus nerve |
| Cecum + ascending/transverse colon | T9–L1 via Celiac plexus | Vagus nerve |
| Descending colon | T9–T12 via Celiac plexus | S2–S4 pelvic nerves |
| Sigmoid + Rectum | T11–L1 via Inferior hypogastric plexus | S2–S4 pelvic nerves |
The Gut–Brain Axis (Afferent Pathways)
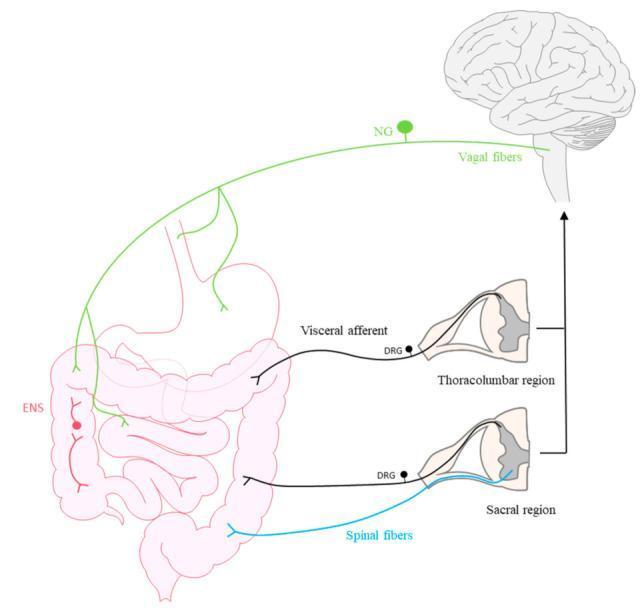
- Vagal afferents (green): cell bodies in nodose ganglion → nucleus tractus solitarius in brainstem → transmit satiety, nausea, distension (not pain)
- Thoracolumbar visceral afferents (black): via DRG → spinal cord → transmit visceral pain (poorly localized, referred)
- Sacral spinal fibers (blue): from distal colon/rectum → transmit pelvic visceral sensation
Clinical Applications of Nerve Supply
| Condition | Nerve Involved | Mechanism |
|---|---|---|
| Hirschsprung disease | ENS absent (no ENS ganglia in distal colon) | No peristalsis → functional obstruction |
| Vagotomy side effects | Vagus CN X | Gastroparesis, gallstones (gallbladder paralysis) |
| Celiac plexus block | Celiac ganglion | Used for intractable pancreatic cancer pain |
| Referred pain (appendicitis) | T10 sympathetic afferents → periumbilical at first | Visceral pain before peritoneal irritation localizes it |
| Nutcracker syndrome pain | T9–L1 renal/retroperitoneal afferents | Flank/abdominal pain from venous congestion |
Sources: Guyton & Hall Medical Physiology, p. 778–780 | Miller's Anesthesia, p. 1464–1470 | Goldman-Cecil Medicine, p. 1405–1406 | Gray's Anatomy for Students, p. 413–416

Explain this
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Finding Sources
Reading File
Searching Images
portosystemic anastomoses portal hypertension esophageal varices caput medusae diagram
Loading Image
Loading Image
Here is a complete explanation of everything on this page — Portosystemic Anastomoses.
The Big Picture: What Is a Portosystemic Anastomosis?
The portal venous system collects blood from the entire GI tract, spleen, and pancreas and delivers it to the liver for processing (detoxification, nutrient metabolism). This blood normally flows: gut → portal vein → liver → hepatic veins → IVC.
At certain anatomical sites, small connections (anastomoses) exist between the portal venous system and the systemic venous system. Under normal conditions these are tiny and clinically silent.
In portal hypertension (usually from liver cirrhosis), pressure backs up in the portal vein. Blood is forced through these small connections, which dilate massively into varices — this is the pathologic reversal of flow shown by the red arrows in your diagram.
The Portal Venous System (Normal Anatomy)
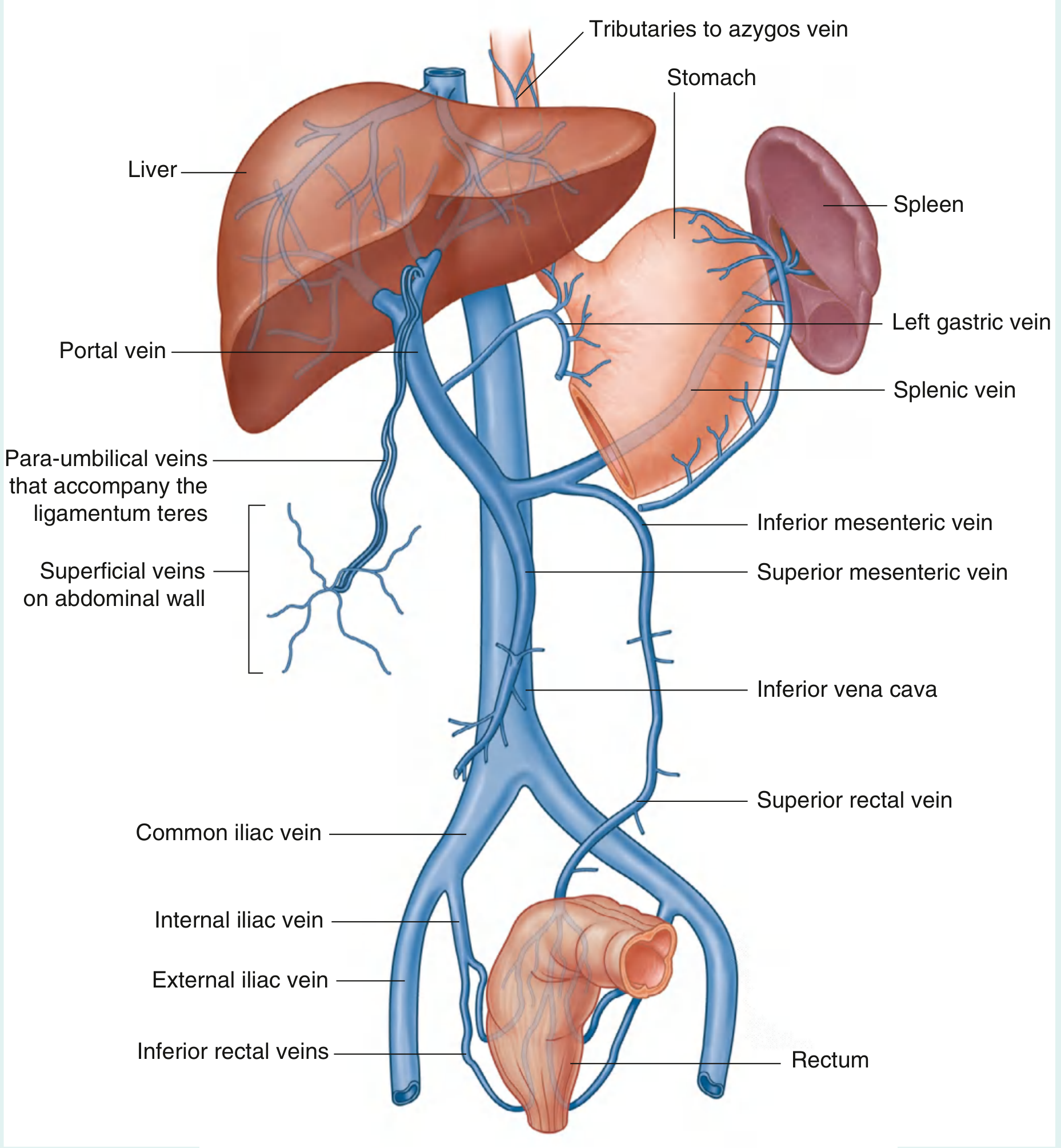
The portal vein (formed by splenic vein + superior mesenteric vein behind the neck of the pancreas) receives:
- Splenic vein — from spleen + left gastric vein + inferior mesenteric vein
- Superior mesenteric vein — from small bowel, cecum, ascending/transverse colon
- Inferior mesenteric vein → drains into splenic vein — from descending colon, sigmoid, upper rectum
The Four Portosystemic Anastomotic Sites
❶ Esophagus — Clinical Sign: Esophageal Varices
| Portal side | Systemic side |
|---|---|
| Left gastric vein (= coronary vein) | Esophageal veins → azygos vein → SVC → IVC |
Mechanism: The left gastric vein is a direct tributary of the portal vein. At the lower esophagus it anastomoses with submucosal esophageal veins draining into the azygos system. When portal pressure rises, blood flows retrograde through this connection → the submucosal veins of the lower esophagus dilate into esophageal varices.
Clinical significance — most dangerous of all sites:
- Varices lie in the submucosa → directly exposed to trauma from food
- Can rupture → torrential, life-threatening hemorrhage (mortality 20–30% per bleed)
- Treatment: endoscopic band ligation, sclerotherapy, vasopressin, balloon tamponade (Sengstaken-Blakemore tube), TIPS
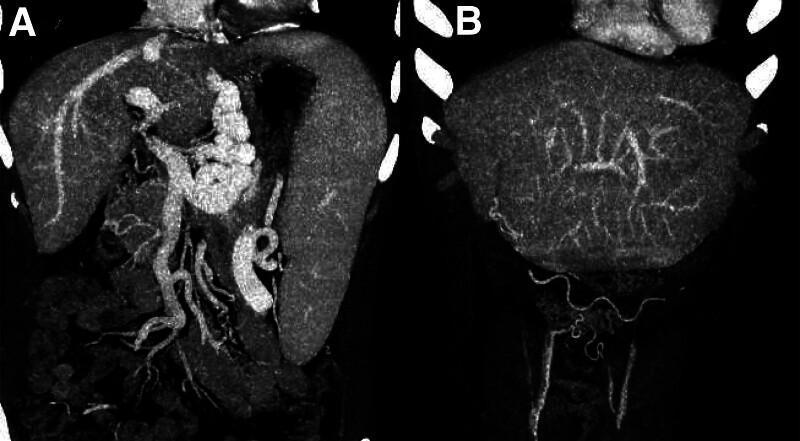
CT imaging showing esophageal varices and splenic enlargement in portal hypertension:
❷ Umbilicus — Clinical Sign: Caput Medusae
| Portal side | Systemic side |
|---|---|
| Paraumbilical veins (travel in falciform ligament alongside ligamentum teres) | Superficial epigastric veins + inferior/superior epigastric veins → IVC and SVC |
Mechanism: The ligamentum teres (round ligament of the liver) is the obliterated remnant of the fetal umbilical vein. Small paraumbilical veins still run alongside it in the falciform ligament. When portal pressure rises, these reopen/dilate and blood fans out through the anterior abdominal wall veins at the umbilicus.
Clinical sign: "Caput Medusae" (Latin: head of Medusa) — tortuous, dilated veins radiating outward from the umbilicus like snakes, resembling the mythological Gorgon's head.
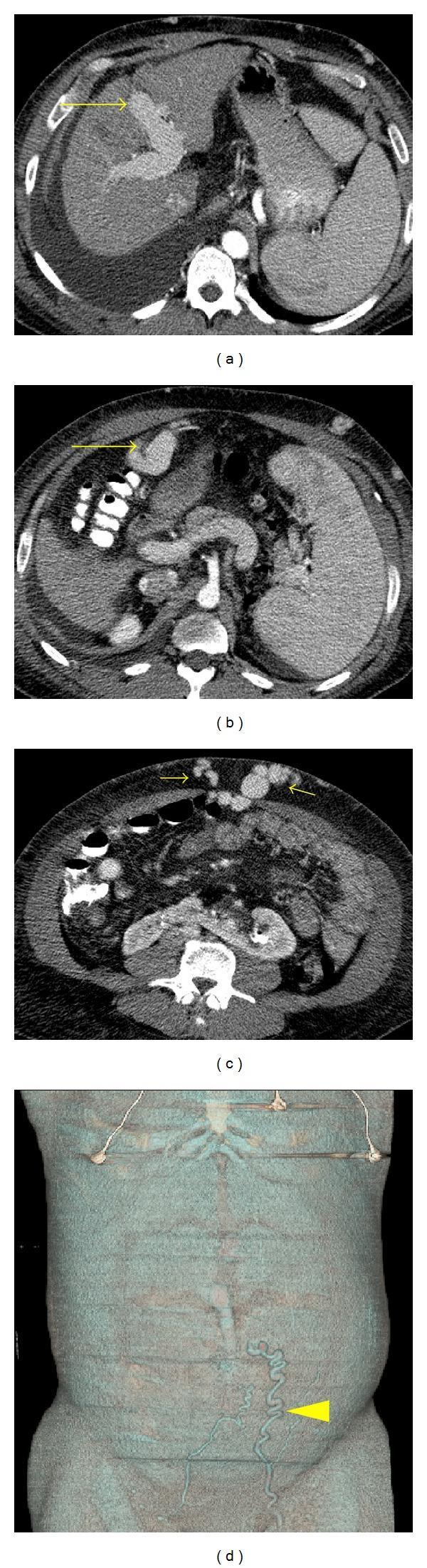
CT showing recanalized paraumbilical vein and caput medusae on abdominal wall:
Distinguishing from IVC obstruction: In caput medusae (portal hypertension), blood flows away from the umbilicus in all directions. In IVC obstruction, superficial abdominal veins dilate to carry blood upward (bypassing the IVC) — flow is upward in both upper and lower abdominal veins.
❸ Rectum — Clinical Sign: Anorectal Varices
| Portal side | Systemic side |
|---|---|
| Superior rectal vein (IMA tributary → portal) | Middle and inferior rectal veins → internal iliac → IVC |
Mechanism: The superior rectal vein is the terminal branch of the inferior mesenteric vein (portal system). It anastomoses with middle and inferior rectal veins (which drain into the internal iliac = hypogastric vein → systemic). Portal hypertension forces blood retrograde → anorectal varices develop in the submucosal venous plexus of the rectum.
Important: Anorectal varices ≠ haemorrhoids. Haemorrhoids are a separate condition (dilatation of normal internal/external haemorrhoidal cushions). But portal hypertension can worsen both.
❹ Portosystemic Shunt (TIPS) — Shown in the Diagram
This is not a natural anastomosis — it is a therapeutic shunt created to treat portal hypertension.
TIPS = Transjugular Intrahepatic Portosystemic Shunt
How it's done:
- A catheter is introduced via the right internal jugular vein
- Guided down through SVC → right atrium → IVC → right hepatic vein
- A needle is advanced through the liver parenchyma into the right branch of the portal vein
- The tract is dilated and a metallic stent is placed to keep it open
- This creates a direct channel: portal vein → hepatic vein → IVC, bypassing the liver sinusoids
Effect: Drops portal pressure immediately, decompressing all varices simultaneously.
Major complication:
- Hepatic encephalopathy — because the liver is bypassed, ammonia and other toxins from gut metabolism are not cleared → enter systemic circulation → cross blood-brain barrier → delirium/confusion/coma
- Less effective at improving overall survival vs. transplant
Summary Table
| Site | Portal Vessel | Systemic Vessel | Clinical Sign | Most Dangerous? |
|---|---|---|---|---|
| ❶ Esophagus | Left gastric vein | Esophageal veins → azygos | Esophageal varices | YES — life-threatening bleeds |
| ❷ Umbilicus | Paraumbilical veins | Superficial epigastric veins | Caput medusae | Less dangerous |
| ❸ Rectum | Superior rectal vein | Middle + inferior rectal veins | Anorectal varices | Moderate risk |
| ❹ TIPS (therapeutic) | Portal vein | Hepatic vein | Relieves all of the above | Risk of encephalopathy |
Mnemonic: "Gut, Butt, and Caput" (as your textbook states)
- Gut = esophageal varices
- Butt = anorectal varices
- Caput = caput medusae
These three are the classic signs of portal hypertension seen at the three natural portosystemic anastomotic sites.
Sources: Gray's Anatomy for Students, p. 418–420 | Medical Physiology (Boron & Boulpaep), p. 3829–3830 | Miller's Anesthesia
This is a shared conversation. Sign in to Orris to start your own chat.