Uterine Prolapse
Reading File
Finding Sources
Finding Sources
Searching PubMed
"uterine prolapse" management
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive content from both Berek & Novak's Gynecology and Campbell Walsh Wein Urology. Let me compile the full, detailed answer.
Uterine Prolapse
Definition
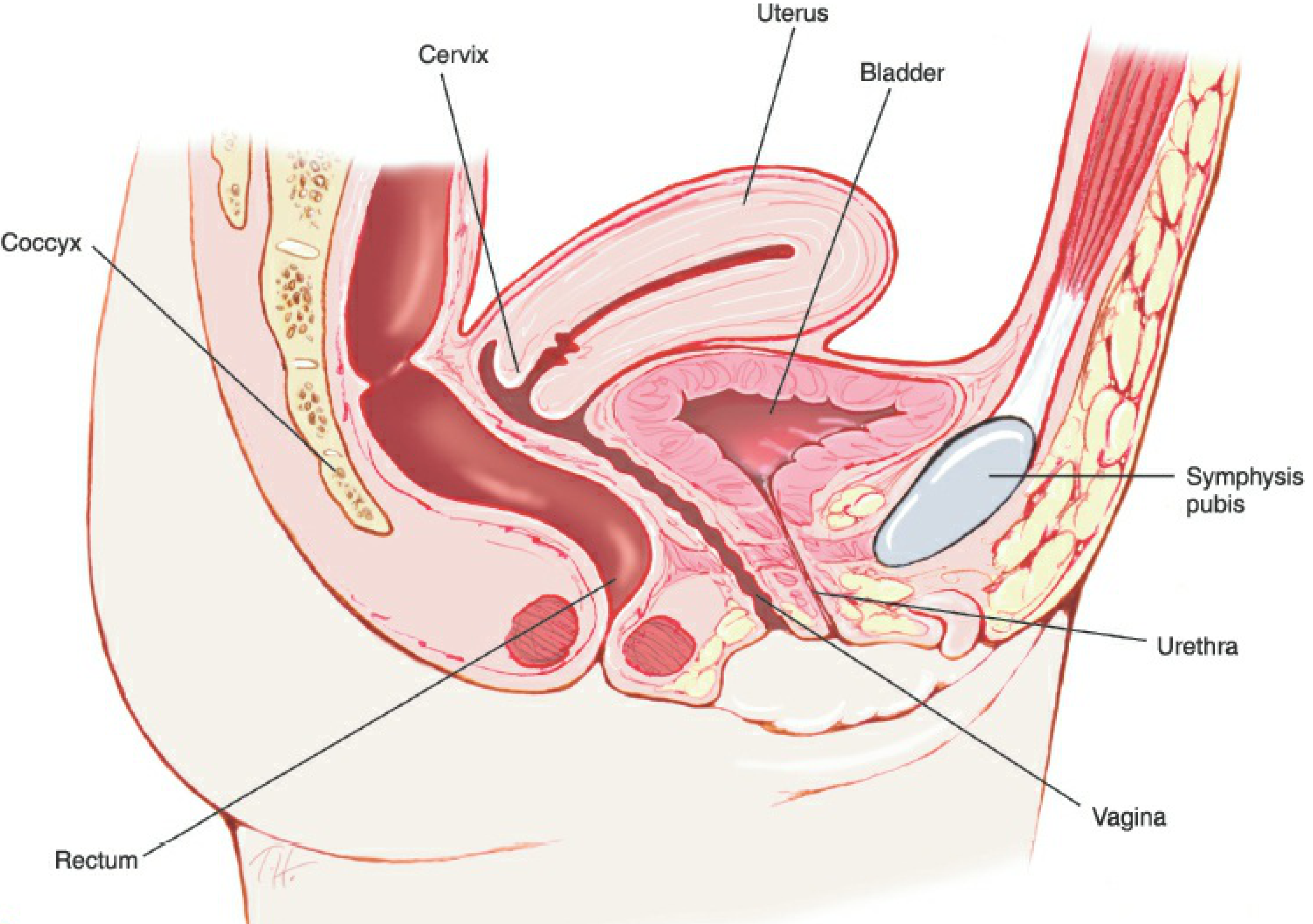
Pelvic organ prolapse (POP) is the "descent of one or more of the anterior vaginal wall, posterior vaginal wall, the uterus (cervix), or the apex of the vagina (vaginal vault or cuff scar after hysterectomy)," correlated with symptoms. Uterine prolapse specifically refers to the descent of the uterus through the urogenital diaphragm into or beyond the vaginal canal, caused by failure of the supportive cardinal-uterosacral ligament complex.
Normal pelvic anatomy (sagittal view):
Epidemiology
- In the United States, 11% of women up to age 80 have surgery for POP or urinary incontinence; nearly one-third are repeat procedures.
- Uterine prolapse accounts for 14.3% of POP in Women's Health Initiative data.
- Women with at least one vaginal delivery are twice as likely to develop POP as nulliparous women.
- Berek & Novak's Gynecology, p. 1595
Anatomy & Pathophysiology
The uterus is supported by three levels of pelvic support:
| Level | Structure | Function |
|---|---|---|
| Level I | Cardinal/uterosacral ligament complex | Suspends vaginal apex, maintains vaginal length and axis |
| Level II | Paravaginal attachments to arcus tendineus and levator fascia | Maintains midline position of vagina |
| Level III | Muscles and connective tissue around distal vagina and perineum | Supports vaginal introitus |
The uterosacral ligaments originate at sacral vertebrae S2-S4 and insert at the upper vagina and cervix. The broad ligament does not provide significant support. When the cardinal-uterosacral complex attenuates (via tears, neuromuscular dysfunction, or both), uterine prolapse results.
Birth-induced injury to the pubococcygeal portion of the levator ani is seen in 55% of women with prolapse vs. 16% of women with normal support.
- Berek & Novak's Gynecology, p. 1596; Campbell Walsh Wein Urology, p. 3713
Risk Factors
Obstetric:
- Vaginal delivery (strongest risk factor)
- High parity
- Prolonged labor, instrumental delivery
Non-obstetric:
- Increasing age
- Obesity
- Constipation (chronic straining)
- Chronic obstructive pulmonary disease (raised intra-abdominal pressure)
- Prior hysterectomy
- History of previous prolapse operations
- Race (higher prevalence in White women than Black women)
- Berek & Novak's Gynecology, p. 1595
Classification / Staging (POP-Q System)
The Pelvic Organ Prolapse Quantification (POP-Q) system is approved by the International Continence Society. It identifies 9 anatomical locations in the vagina and vulva, measured in centimeters relative to the hymen.
| Stage | Description |
|---|---|
| Stage 0 | No prolapse |
| Stage I | Most distal portion >1 cm above the hymen |
| Stage II | Most distal portion between 1 cm above and 1 cm below the hymen |
| Stage III | Most distal portion >1 cm below the hymen but protrudes less than total vaginal length minus 2 cm |
| Stage IV | Complete eversion/procidentia |
Older grading (still used clinically):
- 1st degree: cervix descends into vaginal canal but not to introitus
- 2nd degree: cervix reaches introitus
- 3rd degree: cervix protrudes beyond introitus
- 4th degree (procidentia): entire uterus and vaginal walls are everted
- Berek & Novak's Gynecology, p. 1609-1610
Clinical Features
Symptoms
- Vaginal bulge - most specific symptom; vaginal descensus 0.5 cm distal to the hymen predicts bulge symptoms with 69% sensitivity, 97% specificity
- Pelvic pressure or heaviness, worsened by prolonged standing
- Lower urinary tract symptoms: urinary incontinence, urgency/frequency, obstructive voiding, retention
- Women with more advanced prolapse are less likely to report stress incontinence and more likely to manually reduce the prolapse to void
- Bowel symptoms: constipation, obstructed defecation, fecal incontinence
- Low back and flank pain
- Dyspareunia
Physical Examination
- Examine in lithotomy position; encourage Valsalva maneuver to demonstrate full extent of prolapse
- Use Graves speculum (apical), Sims or univalve speculum (anterior/posterior compartments)
- Rectovaginal exam to distinguish posterior wall defect from enterocele
- Standing straining exam if supine findings inconsistent with symptoms
- Berek & Novak's Gynecology, p. 1609
Treatment
1. Conservative / Non-surgical
Lifestyle modifications:
- Weight reduction
- Treat chronic constipation
- Avoid heavy lifting
Pelvic floor muscle training (Kegel exercises):
- Strengthens levator ani and puborectalis
- Appropriate for mild-to-moderate prolapse
Pessaries (mechanical devices):
- First-line non-surgical option for symptomatic prolapse in women who desire to avoid surgery or are poor surgical candidates
- Provide mechanical support without addressing the underlying defect
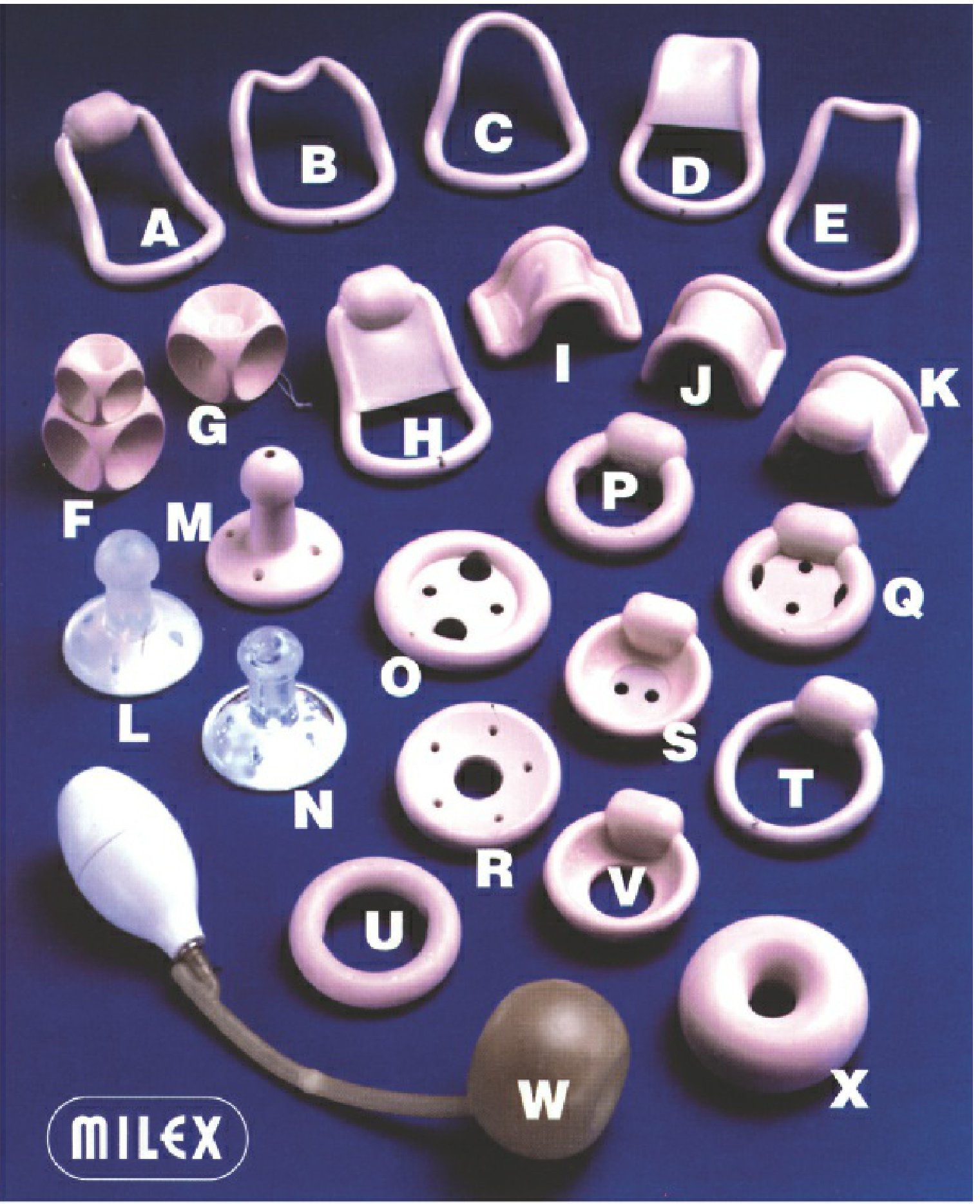
Pessary types and uses:
| Type | Notes |
|---|---|
| Ring with/without support | Most commonly used; easiest to insert/remove; 1st and 2nd degree prolapse |
| Gellhorn | Moderate-severe prolapse; stays in 6-8 weeks; harder to self-manage |
| Cube | Held by suction and space occupation; must be removed daily |
| Donut | Space-filling; for large vault prolapse / procidentia with reduced perineal support |
| Continence ring/dish | When stress incontinence coexists |
Fitting protocol:
- Digital exam to estimate size; ring forceps to reduce prolapse
- Patient stands, performs Valsalva, and coughs - pessary must be retained
- Proper fit: index finger sweeps between pessary and vaginal wall
- Patient must void before leaving office
- Follow-up at 1-2 weeks, then 4-6 weeks, then every 6-12 months
- Monitor for vaginal ulceration, pressure sores, infection
- Berek & Novak's Gynecology, p. 1615-1619
2. Surgical Management
Surgery is indicated when symptoms are bothersome and not controlled by conservative measures. Treatment is individualized based on: compartment(s) involved, desire for future fertility, uterine preservation preference, health status, and whether obliterative or reconstructive approach is preferred.
Vaginal Procedures
Vaginal hysterectomy + apical suspension:
- Standard for uterine prolapse in women not desiring fertility preservation
- Vaginal hysterectomy alone is not adequate - apex must be suspended to prevent recurrent POP
- McCall culdoplasty is the minimum addition: closes the peritoneal cul-de-sac, prevents enterocele, and provides apical fixation
- Uterosacral ligament suspension (USLS) and sacrospinous ligament fixation (SSLF) are additional apical suspension techniques
Uterine-preserving procedures (Hysteropexy):
- For women who desire fertility preservation or prefer uterine conservation
- Manchester-Fothergill procedure: amputation of cervix + cardinal ligament plication
- Sacrospinous hysteropexy
- Comparable durability to hysterectomy-based repair in selected patients
Abdominal / Minimally Invasive Procedures
Abdominal/laparoscopic/robotic sacrocolpopexy:
- Mesh attached from vaginal apex to sacral promontory
- Considered the most durable repair for apical prolapse
- Associated with lower prolapse recurrence rates vs. vaginal repairs in comparative trials
Uterosacral ligament suspension (USLS) - abdominal approach:
- Native tissue repair; avoids mesh-related complications
Obliterative Procedures
Colpocleisis (Le Fort or total):
- Partial or total closure of the vaginal canal
- Reserved for elderly, frail patients who are sexually inactive and poor surgical candidates for reconstructive procedures
- Very high success rates with low recurrence
- During colpocleisis, at least 1.5 cm of the distal anterior vaginal wall adjacent to the urethral meatus should be preserved to avoid unmasking stress urinary incontinence
- Campbell Walsh Wein Urology, p. 3713; Berek & Novak's Gynecology, p. 1618-1625
Associated Conditions
Uterine prolapse frequently coexists with:
- Cystocele (anterior vaginal wall prolapse) - most common associated defect
- Rectocele (posterior vaginal wall prolapse)
- Enterocele (small bowel herniation into posterior cul-de-sac)
- Stress urinary incontinence (may be occult when prolapse is severe)
Any concomitant compartment defects should be addressed at the same surgical setting.
Special Considerations
- Occult SUI: Women undergoing prolapse repair should be screened preoperatively; a concomitant anti-incontinence procedure may be offered
- Mesh use: Transvaginal mesh for prolapse carries FDA safety concerns; abdominal sacrocolpopexy (where mesh is used abdominally) has a better safety profile than transvaginal mesh
- Pregnancy: Uterine prolapse can complicate pregnancy; cervical prolapse is a known complication
- Contraindications to vaginal hysterectomy: Endometriosis of unknown extent, obliterated cul-de-sac, large fibroids, pelvic/adnexal tumors, uterine/ovarian malignancy
Sources:
- Berek & Novak's Gynecology, Chapter 30 (Pelvic Organ Prolapse), pp. 1593-1630
- Campbell Walsh Wein Urology, Chapter 124 (Vaginal Reconstructive Surgery), pp. 3710-3715
This is a shared conversation. Sign in to Orris to start your own chat.