Dupuytren fracture dislocation what's this mechanism of injury associated injury classification signs and symptoms investigation and treatment explain in detail with appropriate illustrative diagrams and images
Reading File
Finding Sources
Finding Sources
Searching the Web
Dupuytren fracture dislocation ankle mechanism classification treatment
Reading File
Finding Sources
Searching the Web
Dupuytren fracture dislocation ankle Lauge-Hansen pronation external rotation mechanism signs symptoms X-ray
Searching PubMed
Dupuytren fracture dislocation ankle treatment
Reading File
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC9398172
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Finding Sources
I now have comprehensive information. Let me compile the detailed answer.
Dupuytren Fracture-Dislocation of the Ankle
Historical Note
Guillaume Dupuytren first described this injury in 1819, publishing his observations on fractures of the lower fibula with dislocation of the foot. The injury was later detailed more formally in his 1847 work On the Injuries and Diseases of Bones. It is sometimes confused with Dupuytren's contracture (a palmar fibromatosis) - these are completely separate entities, both named after the same French surgeon.
Definition
A Dupuytren fracture-dislocation is a specific injury pattern of the ankle characterized by:
- A fracture of the lower end (distal shaft) of the fibula at or above the level of the tibiofibular syndesmosis (suprasyndesmotic)
- Associated complete disruption of the syndesmotic ligament complex
- Medial-sided injury (deltoid ligament rupture or medial malleolus fracture)
- Lateral or posterolateral dislocation of the talus from the ankle mortise
- It is essentially a high-energy variant of the Pronation-External Rotation (PER) pattern in the Lauge-Hansen classification
It is closely related to - but distinct from - the Maisonneuve fracture (where the fibular fracture is very proximal near the fibular neck). In Dupuytren's injury, the fibular fracture is in the distal third/at the level of the syndesmosis.
Anatomy Relevant to This Injury
The ankle mortise is stabilized by three key complexes:
| Structure | Composition | Function |
|---|---|---|
| Medial (deltoid) ligament | Superficial + deep layers | Resists eversion, external rotation of talus |
| Lateral ligament complex | ATFL, CFL, PTFL | Resists inversion |
| Tibiofibular syndesmosis | AITFL, PITFL, interosseous membrane, interosseous ligament | Binds fibula to tibia; maintains mortise width |
The fibula carries approximately 17% of body-weight loading and is the key lateral buttress of the mortise. When it fractures above the syndesmosis, the talus is no longer constrained laterally.
Mechanism of Injury
The Dupuytren fracture-dislocation results from a pronation-external rotation (PER) mechanism, applied with high energy.
Step-by-Step Sequence (Lauge-Hansen PER Stages)
The foot is in pronation (eversion/abduction) at the time of injury. An external rotational force is then applied, or the body rotates internally over a planted, pronated foot.
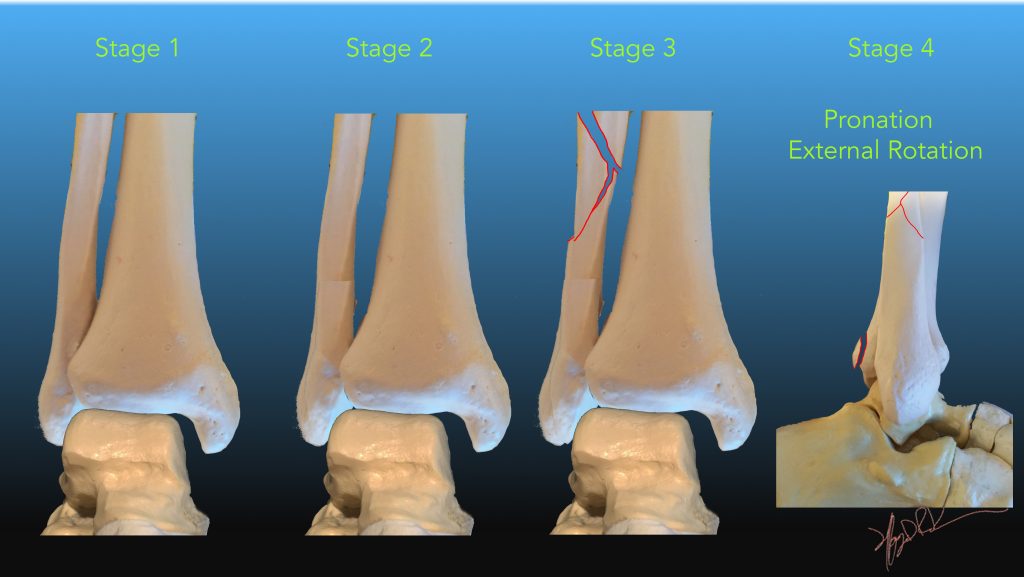
| Stage | Injury | Radiographic Correlate |
|---|---|---|
| Stage I | Transverse fracture of medial malleolus or rupture of the deltoid ligament | Medial malleolus fracture or mortise widening |
| Stage II | Rupture of the AITFL (anterior inferior tibiofibular ligament) or avulsion of the anterior lip of the tibial plafond | Widening of syndesmosis; Chaput tubercle avulsion |
| Stage III | Oblique or spiral fracture of the fibula above the level of the syndesmosis - this is the defining fibular fracture | Suprasyndesmotic fibular fracture (Weber C / AO 44-C) |
| Stage IV | Rupture of PITFL or avulsion of the posterior malleolus | Posterior tibial fragment; further widening |
In Dupuytren's original description, the fibular fracture sits just above the syndesmosis (lower fibular shaft), whereas in Maisonneuve the fracture extends to the fibular neck. Both represent PER injuries of differing energy.
Common Mechanisms in Clinical Practice
- Twisting falls with foot planted in eversion - sports injuries (football, rugby, skiing)
- Road traffic accidents - passenger or pedestrian with externally rotated, pronated foot
- Falls from height with foot landing in eversion
- Industrial injuries - machinery catching the foot
The pronated foot position places the medial structures under maximal tension first, which is why medial injury (deltoid ligament or medial malleolus) occurs before the lateral fibular fracture - the opposite sequence to supination injuries.
Associated Injuries
Because this is a high-energy, completely unstable injury, the following associated injuries must be actively sought:
Bony Injuries
- Posterior malleolus fracture (trimalleolar equivalent) - present in ~30-50% of cases
- Medial malleolus fracture (or isolated deltoid ligament rupture)
- Proximal fibula fracture (full Maisonneuve pattern)
- Osteochondral injury to the talar dome (articular cartilage shearing during dislocation)
- Calcaneal fractures in high-energy falls
Ligamentous Injuries
- Complete syndesmotic disruption (AITFL + interosseous ligament + PITFL)
- Deltoid ligament rupture (deep and superficial)
- Lateral ligament complex injury (if foot supinated secondarily)
Soft Tissue & Neurovascular Injuries
- Peroneal tendon injury or dislocation
- Skin compromise - skin tenting over the lateral malleolus is a surgical emergency requiring urgent reduction
- Posterior tibial artery / peroneal artery injury with vascular compromise
- Superficial peroneal nerve injury (dorsal foot numbness)
- Sural nerve injury
- Compartment syndrome of the leg (rare but must be excluded in high-energy cases)
Classification Systems
Three systems are used in clinical practice, all applicable to Dupuytren fracture-dislocation:
1. Lauge-Hansen Classification (Mechanism-Based)
This injury falls under Pronation-External Rotation (PER) Stage III or IV:
- PER Stage III - Medial injury + syndesmotic disruption + suprasyndesmotic fibular fracture
- PER Stage IV - Above + posterior malleolus fracture/PITFL rupture
This is the most important classification for planning closed reduction because the reduction maneuver reverses the mechanism (supinate + internally rotate the foot).
2. Danis-Weber / AO-OTA Classification (Radiographic)
Based on the level of fibular fracture relative to the syndesmosis:
| Type | Location | Stability | Treatment |
|---|---|---|---|
| Weber A (AO 44-A) | Below syndesmosis | Stable | Usually non-operative |
| Weber B (AO 44-B) | At syndesmosis | Variable - stress test required | Depends on stability |
| Weber C (AO 44-C) | Above syndesmosis | Inherently unstable | Operative |
Dupuytren fracture-dislocation is always Weber C / AO 44-C - inherently unstable requiring operative intervention.
3. Number of Malleoli Involved (Descriptive)
Used commonly in emergency medicine:
- Bimalleolar fracture - fibula fracture + medial malleolus fracture
- Bimalleolar equivalent - fibula fracture + deltoid ligament rupture (medial malleolus intact but medial side disrupted)
- Trimalleolar fracture - bimalleolar + posterior malleolus fracture
Signs and Symptoms
History
- High-energy twisting or rotational injury
- Foot typically in eversion/pronation at time of impact
- Immediate inability to bear weight
- Immediate severe pain and swelling
Symptoms
- Severe pain around the ankle and lower leg
- Inability to weight-bear
- Sensation of something "giving way" or a "crack/snap" heard at time of injury
- Paresthesia or numbness in the foot (nerve injury)
- Coolness or pallor of foot (vascular compromise, if present)
Signs on Examination
Look:
- Gross swelling of the entire ankle and lower leg
- Obvious deformity - lateral or posterolateral displacement of the foot relative to the leg
- Skin tenting or puckering over the medial malleolus or laterally (indicates impending skin necrosis - URGENT)
- Bruising extending up the leg
- Open wound in open fracture-dislocations
- Foot held in eversion and external rotation
Feel:
- Point tenderness along the fibula above the ankle (suprasyndesmotic region)
- Tenderness over the medial malleolus or deltoid ligament
- Tenderness over the entire syndesmotic region
- Crepitus on palpation
- Capillary refill, peripheral pulses (dorsalis pedis, posterior tibial) - assess vascular status
- Sensation testing of foot dorsum (superficial peroneal nerve) and sole
Move:
- Range of motion severely restricted or impossible due to pain/deformity
- Do NOT attempt active or passive movement if dislocation is suspected until imaging
Special Tests (only if no obvious dislocation):
- External rotation stress test - external rotation of the foot with knee at 90° - pain/widening indicates syndesmotic disruption
- Cotton test - lateral stress on the talus
- Squeeze test (Hopkin's test) - compressing fibula against tibia at mid-calf - pain at the ankle indicates syndesmotic injury
Investigations
Plain Radiographs (First Line)
Standard views: AP, lateral, and mortise (15-20° internal rotation AP)

Radiographic findings to look for:
| Finding | Significance |
|---|---|
| Oblique/spiral fibular fracture above the syndesmosis | Defining feature of Dupuytren/PER pattern |
| Medial clear space widening >4 mm | Medial instability (deltoid rupture or medial malleolus fracture) |
| Tibiofibular clear space >6 mm | Syndesmotic disruption |
| Tibiofibular overlap <10 mm (AP) or <1 mm (mortise) | Syndesmotic diastasis |
| Lateral talar shift | Ankle mortise disruption |
| Posterior malleolus fragment | Stage IV / trimalleolar injury |
| Talar dislocation | Completely displaced injury |

Stress Radiographs:
- If no obvious dislocation but syndesmotic disruption suspected - gravity stress view or externally applied stress view
- Widening of medial clear space confirms instability
CT Scan (Second Line)
Indications:
- Preoperative planning for all operative cases
- Assessment of posterior malleolus fracture size and displacement
- Assessment of articular comminution
- Identification of associated injuries (osteochondral lesions, small avulsion fragments)
- Equivocal plain radiographs
MRI
Indications:
- Suspected occult ligamentous injury when radiographs appear normal
- Assessment of syndesmotic ligament integrity
- Osteochondral lesion characterization
- Not routine in acute severe injuries
Vascular Studies (if needed)
- If diminished pulses or abnormal capillary refill: urgent Doppler ultrasound or CT angiography
- Ankle-Brachial Index (ABI) if ischemia suspected
Treatment
Immediate/Emergency Management
ABCDE approach first in polytrauma.
1. Neurovascular Assessment
- Document dorsalis pedis and posterior tibial pulses
- Document sensation (dorsal foot = superficial peroneal; medial/lateral sole = tibial branches)
- ABI if pulses are diminished
2. Analgesia
- IV opioids + regional nerve block (popliteal sciatic block, if available)
- Procedural sedation for reduction
3. Urgent Closed Reduction (emergency - before definitive imaging if skin compromise)
If there is frank dislocation with skin tenting - immediate reduction is mandatory regardless of imaging status to prevent skin necrosis.
Reduction Technique (reversing the PER mechanism):
- Adequate analgesia or procedural sedation
- Flex the knee to relax the gastrocnemius
- Apply longitudinal traction on the heel
- Supinate and internally rotate the foot (reversing the pronation-external rotation mechanism)
- Push the talus back medially under the tibial plafond
- Apply a well-padded backslab (posterior + U-slab) in neutral position
Post-reduction:
- Repeat neurovascular assessment
- Repeat radiographs to confirm reduction
- Elevation of the limb
Definitive Treatment
Non-Operative Treatment
Indications (very limited for Dupuytren/PER injuries):
- Non-displaced, stable injuries only (virtually never a Dupuytren fracture-dislocation)
- Medically unfit patients where surgical risk exceeds benefit
Protocol if used:
- Short leg cast with ankle in neutral position
- Non-weight-bearing for 6-8 weeks
- Serial radiographs at 1, 2, and 6 weeks to monitor for redisplacement
- Progressive weight-bearing in boot after bony union confirmed
- Physiotherapy
Non-operative treatment of a true Dupuytren fracture-dislocation carries a very high failure rate due to inherent instability. Secondary displacement and malunion rates have been reported as high as 73%.
Operative Treatment (Standard of Care)
Timing of surgery:
- Emergency (within hours): irreducible dislocation, open fractures, vascular injury, progressive neurological deficit, skin compromised
- Urgent (within 24-48 hours): reducible dislocation with intact skin - wait for swelling to subside to a point where the skin wrinkles
- Semi-elective (5-10 days): after soft tissue swelling resolves - optimal soft tissue condition reduces wound complication risk
General principle: Restore anatomical alignment of the fibula, then assess and address the syndesmosis and medial side.
Surgical Techniques
Step 1: Fibula ORIF (Open Reduction Internal Fixation)
This is the cornerstone of treatment for the suprasyndesmotic fibular fracture.
- Approach: Direct lateral (or posterolateral) approach to the fibula
- Fixation options:
- Plate and screws (most common) - lateral neutralization plate or posterior antiglide plate with 3.5 mm screws; minimally invasive plating in osteoporotic bone
- Intramedullary nail (Rush rod, fibular nail) - useful for very distal fractures or osteoporotic bone
- Lag screws alone - only for long oblique/spiral fractures with sufficient cortical purchase

Step 2: Syndesmotic Stabilization
After fibular fixation, the syndesmosis must always be tested with an intraoperative Cotton test (or Knot test). In Dupuytren/PER injuries, the syndesmosis is virtually always disrupted and requires stabilization.
Options:
| Method | Details | Pros/Cons |
|---|---|---|
| Syndesmotic screw(s) (position screw) | One or two 3.5/4.5 mm cortical screws, 2-3 cortices, 2-3 cm above the plafond, parallel to joint line | Gold standard; requires removal or breakage before weight-bearing |
| Suture button (TightRope) | Flexible fixation allowing physiological micromotion | Does not need removal; higher cost; may allow more motion |
| Syndesmotic staple | Less common | Alternative to screw |
Step 3: Medial Side
After fibula and syndesmosis fixation, reassess the medial side:
- Medial malleolus fracture: ORIF with 2 parallel cannulated screws (tension band wire in very small fragments)
- Deltoid ligament rupture: if medial clear space remains wide after fibula fixation - explore and repair the deltoid ligament (primary repair with suture anchor)
Step 4: Posterior Malleolus
If posterior malleolus fragment is:
- <25% of articular surface and <2 mm displaced - treat conservatively once fibula and syndesmosis fixed
- >25% articular surface or >2 mm displaced - ORIF via posterolateral approach (antiglide plate or cannulated lag screws from anterior-to-posterior)
Posterior malleolus fixation restores approximately 70% of syndesmotic stability and may negate the need for a separate syndesmotic screw.
Post-Operative Care
| Timeframe | Protocol |
|---|---|
| 0-2 weeks | Splint/backslab; leg elevated; wound check; non-weight-bearing |
| 2-6 weeks | Short leg cast or removable boot; non-weight-bearing; suture removal at 2 weeks |
| 6 weeks | Repeat radiographs - if bone healing progressing, initiate partial weight-bearing in boot |
| 10-12 weeks | Progress to full weight-bearing; begin physiotherapy (ROM, proprioception) |
| 3-4 months | Syndesmotic screw removal (if fixed screw used - though this is controversial) before full weight-bearing activities |
| 6-12 months | Return to sport/heavy activities when strength and proprioception restored |
Complications
Early
- Wound dehiscence / infection - especially if surgery performed through swollen skin
- Neurovascular injury during reduction or surgery (sural nerve, superficial peroneal nerve)
- Compartment syndrome - monitor post-reduction
- Skin necrosis from delayed reduction or tenting
- Malreduction - especially of the fibula (rotation, shortening) and syndesmosis
Late
- Posttraumatic arthritis - most common long-term complication; cartilage injury at time of dislocation predisposes. Risk increases with age.
- Malunion - usually from inadequate fixation or non-compliance
- Syndesmotic diastasis (chronic) - missed or inadequately treated syndesmotic injury
- Reflex sympathetic dystrophy (Complex Regional Pain Syndrome) - higher risk in ankle fracture-dislocations than simple fractures
- Stiffness - particularly plantarflexion/dorsiflexion limitation
- Hardware failure or screw breakage - syndesmotic screws commonly break at the screw-plate junction; this is actually expected and does not necessarily require removal if asymptomatic
- Sural nerve entrapment or neuroma - from lateral approach
Comparison with Related Injuries
| Feature | Dupuytren | Maisonneuve | Bosworth |
|---|---|---|---|
| Fibular fracture level | Distal third/suprasyndesmotic | Proximal fibula (fibular neck) | Distal fibula |
| Mechanism | PER | PER (higher energy) | External rotation |
| Syndesmosis | Disrupted | Disrupted | Intact but fibula trapped behind tibia |
| Talus | Laterally dislocated | May or may not dislocate | Not reduced by closed means |
| Treatment | ORIF fibula + syndesmosis | Syndesmosis fixation ± fibular fixation | Mandatory open reduction |
Summary Flowchart
SUSPECTED DUPUYTREN FRACTURE-DISLOCATION
↓
Neurovascular check → Skin tenting? → YES → IMMEDIATE closed reduction
↓
Plain X-ray (AP, Lateral, Mortise)
↓
Suprasyndesmotic fibular fracture + medial disruption confirmed (Weber C)
↓
CT scan for preoperative planning
↓
Is there dislocation? → YES → urgent reduction + backslab, elevate
↓
Wait for soft tissue recovery (skin wrinkling sign)
↓
ORIF: Fibula → Syndesmotic fixation → Medial side → Posterior malleolus
↓
Non-weight-bearing → Progressive rehabilitation → Return to activity
Sources: Miller's Review of Orthopaedics 9th Ed. (p.628); Rockwood & Green's Fractures in Adults 10th Ed. 2025; Rosen's Emergency Medicine; Lauge-Hansen classification review (PMC4562928); Systematic review of ankle fracture-dislocations (PMC9398172); Radiopaedia - Weber/Lauge-Hansen classification.
This is a shared conversation. Sign in to Orris to start your own chat.