Mitral valve regurgitation long question
Reading File
Finding Sources
Searching PubMed
"mitral regurgitation"[MeSH Terms] AND management
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the necessary content to write a comprehensive long answer on Mitral Valve Regurgitation. Let me compose it.
Mitral Valve Regurgitation (MR) - Comprehensive Review
1. Definition and Epidemiology
Mitral regurgitation (MR) is the systolic backflow of blood from the left ventricle (LV) into the left atrium (LA) due to incomplete closure of the mitral valve. It is, together with aortic stenosis, the most frequent valvular heart disease in the general population, with an estimated prevalence of approximately 20% when mild forms are included.
-
In the OxVALVE Population Cohort Study (n = 2,500 patients aged ≥65 years), 19.8% had mild MR and 2.3% had moderate-to-severe MR.
-
Prevalence is strongly age-related: >10% of individuals aged ≥75 years have at least moderate MR.
-
MR prevalence is expected to double before 2050 as the population ages.
-
5-year survival in untreated significant MR: 66 ± 3% in primary MR and 46 ± 3% in secondary MR.
-
Fuster and Hurst's The Heart, 15th Ed.
2. Anatomy of the Mitral Valve Apparatus
The mitral valve is a complex structure with five components, each of which can contribute to MR if dysfunctional:
| Component | Description |
|---|---|
| Mitral annulus | Fibrous ring; saddle-shaped; contracts ~25% during systole to aid coaptation |
| Anterior leaflet | Larger; 3 scallops: A1 (lateral), A2 (central), A3 (medial) |
| Posterior leaflet | Smaller; 3 scallops: P1 (lateral), P2 (central), P3 (medial) |
| Chordae tendineae | Primary (leaflet tips), secondary (mid leaflet), tertiary (leaflet base) |
| Papillary muscles | Anterolateral and posteromedial - insert directly into the LV wall |
The two commissures are the anterolateral and posteromedial commissures. Unlike the aortic valve, dysfunction of ANY component of this apparatus can produce MR, which explains the heterogeneity of causes.
- Fuster and Hurst's The Heart, 15th Ed.
3. Classification
MR is classified by two main systems: etiology and chronicity.
3a. By Etiology
Primary (Organic/Degenerative) MR
- Caused by intrinsic abnormalities of the valve leaflets or subvalvular apparatus
- Leaflets are the primary site of pathology
Secondary (Functional) MR
- Valve leaflets are structurally normal
- MR results from LV or LA geometric distortion causing poor leaflet coaptation
- Two subtypes:
- Ventricular secondary MR: LV dilatation/dysfunction (ischemic cardiomyopathy, dilated cardiomyopathy) causes apical displacement of papillary muscles, tethering the leaflets apically
- Atrial secondary MR: LA enlargement causes annular dilatation without LV involvement
3b. By Chronicity
- Acute MR: Sudden onset, poorly tolerated; hemodynamically catastrophic
- Chronic MR: Develops slowly; allows cardiac compensation for prolonged periods
3c. Carpentier Functional Classification (Mechanism-based)
| Type | Leaflet Motion | Mechanism |
|---|---|---|
| Type I | Normal | Annular dilatation or leaflet perforation |
| Type II | Excessive (prolapse/flail) | Chordal elongation/rupture, papillary muscle elongation/rupture |
| Type IIIa | Restricted (systole + diastole) | Rheumatic disease, calcification |
| Type IIIb | Restricted (systole only) | Ischemic/dilated cardiomyopathy (papillary muscle tethering) |
4. Etiology / Causes
Bailey and Love's table of causes:
| Category | Specific Causes |
|---|---|
| Degenerative | Barlow's disease (myxomatous degeneration), fibromuscular dysplasia, Marfan syndrome, Ehlers-Danlos syndrome, mitral valve prolapse, annular/leaflet calcification |
| Ventricular | Papillary muscle rupture post-MI, transient ischemia, cardiomyopathy with annular dilatation |
| Autoimmune/Infective | Rheumatic heart disease (post-streptococcal), infective endocarditis |
| Other | Trauma, congenital (isolated mitral cleft), ergotamine-containing drugs, radiotherapy |
Most common cause overall: Myxomatous degeneration (in developed countries)
In older adults (age ≥75), myxomatous degeneration remains the most frequent structural cause; functional MR due to chronic LV/annular dilation or ischemic papillary muscle dysfunction is also very common.
- Bailey and Love's Surgery, 28th Ed.; Braunwald's Heart Disease
5. Pathophysiology
The pathophysiology is best understood by dividing it into acute and chronic (compensated → decompensated) phases.
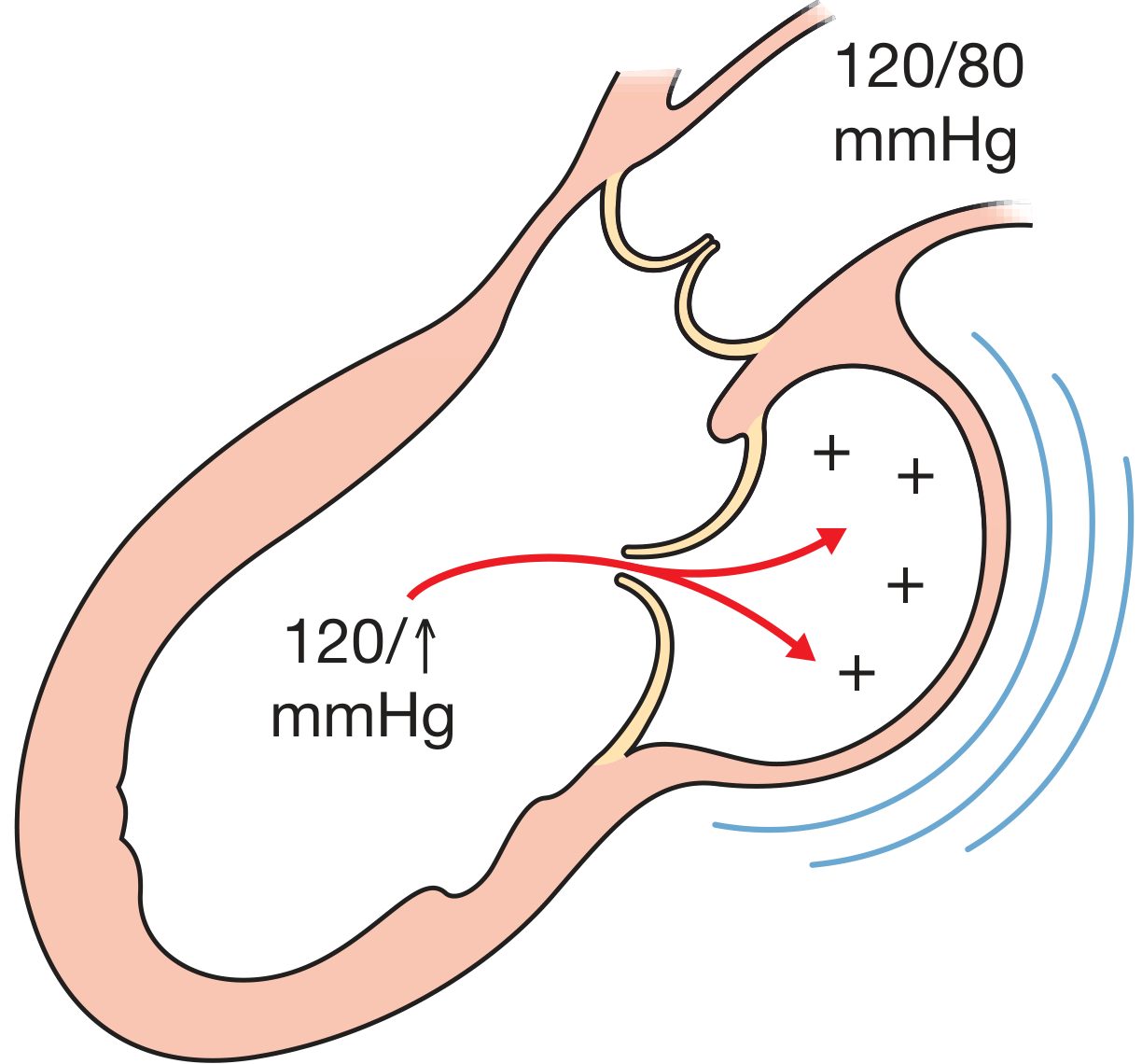
Phase 1: Acute MR
- Sudden regurgitation into a small, non-compliant LA creates abrupt rise in LA pressure
- LV is volume overloaded; Frank-Starling mechanism is maximized
- LV end-diastolic volume (EDV) increases; end-systolic volume (ESV) decreases
- Total stroke volume rises but forward stroke volume is subnormal (large fraction regurgitates)
- Result: Pulmonary edema + low cardiac output despite preserved or hyperdynamic LV function
- EF is often elevated (>70%) due to reduced afterload - does NOT indicate normal LV function
- Clinical emergency: papillary muscle rupture, acute endocarditis, ruptured chordae
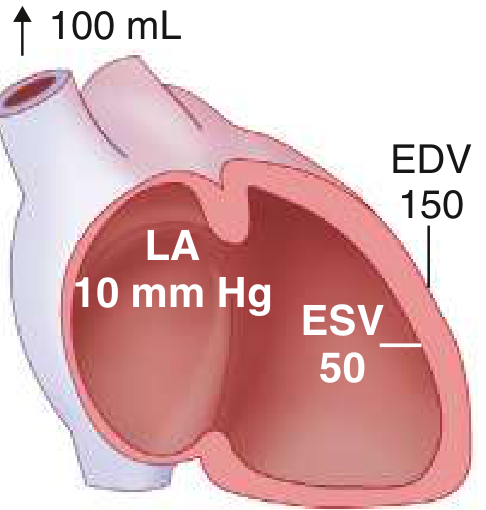
Phase 2: Chronic Compensated MR
- Eccentric LV hypertrophy (sarcomere replication in series) + LA enlargement allow accommodation
- LV EDV is markedly increased; EF remains normal to elevated
- Forward stroke volume normalizes
- Patient may remain asymptomatic for years to decades
- LA enlargement reduces LA pressure despite large regurgitant volume
Phase 3: Chronic Decompensated MR
-
Progressive LV dysfunction (sarcomere dysfunction, wall stress normalization fails)
-
EF falls below normal; end-systolic dimensions increase
-
Symptoms emerge: dyspnea, fatigue, orthopnea
-
Key insight: In MR, EF is artificially elevated due to the low-impedance regurgitant pathway. An EF of 55-60% may represent significant myocardial dysfunction in this context.
-
Pulmonary hypertension (secondary PH) develops, progressing to right heart failure
-
Goldman-Cecil Medicine; Braunwald's Heart Disease; Bailey and Love's Surgery
6. Clinical Features
Symptoms
| Type | Symptoms |
|---|---|
| Acute MR | Sudden dyspnea, orthopnea, pulmonary edema, cardiogenic shock |
| Chronic compensated | Often asymptomatic for years; exercise intolerance may develop |
| Chronic decompensated | Dyspnea on exertion, orthopnea, paroxysmal nocturnal dyspnea, fatigue, palpitations (AF), peripheral edema (right heart failure) |
Signs - Physical Examination
| Finding | Description |
|---|---|
| Apex beat | Displaced, laterally displaced hyperdynamic apical impulse; LV enlargement |
| S1 | Soft or absent (incomplete mitral closure) |
| S3 gallop | Present in significant MR (volume overload) |
| P2 | Loud if pulmonary hypertension develops |
| Murmur | Holosystolic (pansystolic), best heard at the apex, radiates to the axilla (posterior leaflet prolapse) or to the left sternal border (anterior leaflet prolapse) |
| Character | Blowing, high-pitched |
| Effect of Valsalva | Decreases (unlike MVP click-murmur which moves earlier) |
| Effect of squatting | Increases (increased preload) |
Mitral Valve Prolapse murmur specifics: Mid-systolic click followed by a late systolic murmur. The click moves:
- Earlier with Valsalva, standing (reduced preload, smaller LV)
- Later with squatting, leg raising (increased preload, larger LV)
7. Investigations
Electrocardiography
- P-mitrale (broad, notched P-wave) - LA enlargement
- Atrial fibrillation (very common in chronic MR)
- Left ventricular hypertrophy (tall R waves, lateral strain pattern)
- Broad QRS if concomitant LBBB
Chest X-Ray
- Cardiomegaly (LA + LV enlargement)
- Double shadow of enlarged LA on PA view
- Splaying of carina (LA enlargement pushes left main bronchus upward)
- Pulmonary vascular congestion or frank pulmonary edema in decompensated MR
Echocardiography (Gold Standard)
Transthoracic Echocardiography (TTE) is the primary tool:
- 2D echo: Identifies leaflet anatomy, mechanism, LV/LA dimensions, EF
- Color flow Doppler: Visualizes regurgitant jet (direction, extent in LA)
- Proximal Isovelocity Surface Area (PISA) method: Calculates effective regurgitant orifice area (EROA) and regurgitant volume
- 3D echo: More accurate EROA, especially for secondary/crescentic orifice MR
Grading Severity of MR:
| Parameter | Mild | Moderate | Severe |
|---|---|---|---|
| Jet area (% LA area) | <20% | 20-40% | >40% |
| Vena contracta width | <0.3 cm | 0.3-0.69 cm | ≥0.7 cm |
| EROA (primary MR) | <0.2 cm² | 0.2-0.39 cm² | ≥0.4 cm² |
| Regurgitant volume | <30 mL | 30-59 mL | ≥60 mL |
| Regurgitant fraction | <30% | 30-49% | ≥50% |
Secondary MR caveat: EROA ≥0.3 cm² (not 0.4 cm²) can denote severe MR due to the crescent-shaped orifice underestimated by PISA. Regurgitant volume ≥45 mL/beat may indicate severe secondary MR in low-flow states.
Transesophageal Echocardiography (TEE): Mandatory before surgical or transcatheter intervention; provides precise leaflet anatomy for repair planning.
Cardiac MRI (CMR)
- Ideal for quantification of regurgitant volume when echo is suboptimal
- Directly measures regurgitant volume or calculates it as difference between LV stroke volume and aortic forward flow
Cardiac CT
-
Used when transcatheter mitral valve repair/replacement is being considered
-
Provides detailed annular anatomy, annular calcification burden, and access route planning
-
Fuster and Hurst's The Heart, 15th Ed.; Harrison's Principles of Internal Medicine, 22E
8. Management
8a. Medical Therapy
Acute MR:
- Emergency stabilization: IV vasodilators (sodium nitroprusside) to reduce afterload and regurgitant fraction
- Intra-aortic balloon pump (IABP) in cardiogenic shock (reduces afterload, increases forward output)
- Emergency surgery for papillary muscle rupture
Chronic Primary MR:
- No proven benefit of vasodilators (ACE inhibitors, ARBs) in asymptomatic patients with normal LV function - unlike aortic regurgitation
- ACE inhibitors/ARBs and beta-blockers are used if AF or hypertension co-exists
- Diuretics for symptom relief in decompensated disease
- Rate/rhythm control for atrial fibrillation; anticoagulation for AF
Chronic Secondary MR:
- Treat underlying cause (heart failure management: ACEi/ARB/ARNI, beta-blockers, mineralocorticoid antagonists, SGLT2 inhibitors per GDMT)
- Cardiac resynchronization therapy (CRT/CRT-D) when indicated - can significantly reduce functional MR
- Diuretics for congestion
8b. Surgical Indications (Primary MR - ACC/AHA 2020/2021 Guidelines)
| Indication | Recommendation |
|---|---|
| Symptomatic severe MR with preserved LV function | Class I (surgery recommended) |
| Asymptomatic severe MR + LVEF ≤60% | Class I |
| Asymptomatic severe MR + LVESD ≥40 mm | Class I |
| Asymptomatic severe MR + new onset AF or resting PASP >50 mmHg | Class IIa |
| Asymptomatic severe MR + normal LV function + high likelihood of durable repair | Class IIa |
Repair vs. Replacement:
- Mitral valve repair is preferred over replacement whenever technically feasible
- Repair preserves annulopapillary continuity, maintains LV geometry, and avoids prosthesis-related complications
- Operative mortality: ~1-3% for repair at experienced centers vs. ~5-10% for replacement
8c. Surgical Techniques
Annuloplasty - core of virtually every repair:
- Prosthetic ring restores normal saddle shape; prevents progressive annular dilatation
- Sized based on anterior leaflet surface area
Additional repair techniques (for primary MR):
- Chordal replacement (PTFE neochords or "loops")
- Chordal transfer
- Triangular or quadrangular leaflet resection
- Cleft closure
- Leaflet augmentation with pericardial patches
- Focal calcium resection
- Commissural plication (edge-to-edge sutures)
Mitral Valve Replacement (MVR):
-
Required when leaflets are heavily calcified, fused, or fibrotic (Carpentier Type IIIa)
-
Bioprosthetic valves: No anticoagulation needed (after 3 months); degenerate over time (10-15 years); preferred in elderly
-
Mechanical valves: Lifelong anticoagulation required; more durable
-
Fuster and Hurst's The Heart, 15th Ed.; Goldman-Cecil Medicine; Braunwald's Heart Disease
9. Transcatheter Interventions
Transcatheter Edge-to-Edge Repair (TEER) - MitraClip / PASCAL
- Replicates the Alfieri stitch: clips the mid-scallops of the anterior (A2) and posterior (P2) leaflets together, creating a double-orifice mitral valve
- Performed via transseptal approach from the right femoral vein using a 24F sheath under TEE guidance
- FDA-approved for:
- Primary MR in patients with prohibitive surgical risk (EVEREST I/II trials)
- Secondary MR in heart failure patients with LV dysfunction despite optimal GDMT (COAPT trial)
COAPT trial (Stone CW, 2018): Transcatheter MV repair in HF patients with secondary MR resulted in lower HF hospitalization and all-cause mortality over 24 months vs. medical therapy alone.
MITRA-FR trial (Obadia JF, 2018): No significant benefit of TEER over medical therapy in secondary MR - differences between the two trials related to patient selection (COAPT selected patients where MR was "proportionate" with reduced LV dysfunction, MITRA-FR selected "disproportionate" MR patients with more severe LV dysfunction).
Advantages: Less invasive; suitable for high-risk/inoperable patients; improvement in NYHA class and QOL
Limitations: Single-structure repair; not suitable for all valve anatomies
Other Transcatheter Approaches
-
Annuloplasty devices (direct or indirect)
-
Transcatheter Mitral Valve Replacement (TMVR): Emerging; for patients unsuitable for repair
-
Braunwald's Heart Disease; Fuster and Hurst's The Heart, 15th Ed.
10. Complications of Untreated MR
| Complication | Mechanism |
|---|---|
| Atrial fibrillation | LA dilatation; very common; worsens prognosis |
| Heart failure | Progressive LV dysfunction |
| Pulmonary hypertension | Chronic elevation of pulmonary venous pressure |
| Right heart failure | Secondary to PH |
| Thromboembolism | Stasis in dilated LA, especially with AF |
| Infective endocarditis | Abnormal leaflets provide nidus for infection |
| Sudden cardiac death | Rare; more common in MVP with specific high-risk features |
11. Prognosis and Surveillance
- Untreated severe symptomatic MR: poor prognosis with 5-year mortality ~50%
- Successful valve repair before LV dysfunction: near-normal life expectancy
- Key thresholds for surgery: LVEF ≤60% and/or LVESD ≥40 mm - identify the "point of no return"
- Asymptomatic severe MR with normal LV function: yearly history, physical examination, and echocardiography
- BNP/NT-proBNP elevation and deterioration of global longitudinal strain (GLS) on echo are additional early markers suggesting earlier intervention
12. Special Situations
Acute MR from Papillary Muscle Rupture (Post-MI)
- Occurs in 1% of MIs; typically posteromedial papillary muscle (single blood supply from RCA)
- Presents 2-7 days after MI with acute pulmonary edema and cardiogenic shock
- Physical exam: new, loud holosystolic murmur (may be soft if output very low)
- Emergent surgical MVR with resection of damaged muscle and infarct zone is treatment of choice
Mitral Valve Prolapse (MVP)
- Most common cause of primary MR in developed countries
- Myxomatous degeneration causing leaflet billowing >2 mm behind mitral annular plane into LA
- More common in women (younger presentation); balanced sex distribution in older adults
- Auscultation: mid-systolic click + late systolic murmur; click moves with preload changes
- High-risk MVP features: bileaflet prolapse, mitral annular disjunction, T-wave inversion in inferior leads, complex ventricular ectopy - associated with sudden cardiac death risk
Rheumatic MR
- Results from fusion and thickening of leaflet tips with commissural fusion (Type IIIa)
- Often coexists with mitral stenosis
- Prevalent in developing countries; rare in developed nations
Summary Table
| Feature | Acute MR | Chronic Compensated | Chronic Decompensated |
|---|---|---|---|
| LV EDV | Slightly increased | Markedly increased | Markedly increased |
| LV ESV | Decreased | Normal | Increased |
| LV EF | Increased | Normal-increased | Decreased (<60%) |
| LA pressure | Markedly elevated | Normal/mildly elevated | Elevated |
| LA size | Normal | Enlarged | Enlarged |
| Symptoms | Pulmonary edema, shock | Asymptomatic | Dyspnea, fatigue, HF |
| Management | Emergency surgery/stabilize | Watchful waiting | Surgery indicated |
Sources:
- Fuster and Hurst's The Heart, 15th Ed. - Chapter 30 (primary and secondary MR, epidemiology, guidelines)
- Goldman-Cecil Medicine - Chapter 60 (pathophysiology phases, surgical indications)
- Braunwald's Heart Disease - Chapters 76, 78 (transcatheter therapy, management)
- Bailey and Love's Short Practice of Surgery, 28th Ed. - Chapter 59 (causes table, pathophysiology)
- Harrison's Principles of Internal Medicine, 22E - Chapter 248 (echocardiographic assessment)
Books medicine pdf
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Here is the complete list of 135+ medical textbooks available in the library across all specialities. These are integrated into the system and used to answer your medical questions - they are not available for download as PDF files, but I can search and reference any of them to answer your questions in depth.
📚 Medical Textbook Library — Full Catalogue
🫀 Anatomy (8 books)
- Color Atlas of Ultrasound Anatomy, 3e
- Color Atlas of Human Anatomy Vol. 1, 2, 3
- General Anatomy and Musculoskeletal System (THIEME Atlas)
- Gray's Anatomy for Students
- Imaging Anatomy Text and Atlas Vol. 3 (Bones, Joints, Vessels, Nerves)
- Netter's Atlas of Human Anatomy
💉 Anesthesiology (3 books)
- Barash, Cullen & Stoelting's Clinical Anesthesia, 9e
- Miller's Anesthesia, 2-Volume Set, 10e
- Morgan & Mikhail's Clinical Anesthesiology, 7e
🧪 Biochemistry (3 books)
- Basic Medical Biochemistry - A Clinical Approach, 6e
- Biochemistry (Lippincott Illustrated Reviews), 8e
- Harper's Illustrated Biochemistry, 32e
❤️ Cardiology (3 books)
- Braunwald's Heart Disease, 2-Volume Set
- Fuster and Hurst's The Heart, 15th Edition
- Textbook of Clinical Echocardiography
🌍 Community Medicine (1 book)
- Park's Textbook of Preventive and Social Medicine
🧴 Dermatology (4 books)
- Andrews' Diseases of the Skin Clinical Atlas, 2e
- Andrews' Diseases of the Skin - Clinical Dermatology
- Dermatology, 2-Volume Set, 5e
- Fitzpatrick's Dermatology, Volumes 1 & 2
🧬 Embryology (2 books)
- Langman's Medical Embryology
- The Developing Human - Clinically Oriented Embryology
🚨 Emergency Medicine (3 books)
- Rosen's Emergency Medicine - Concepts and Clinical Practice
- Roberts and Hedges' Clinical Procedures in Emergency
- Tintinalli's Emergency Medicine - A Comprehensive Study
👂 ENT / Otolaryngology (6 books)
- Cummings Otolaryngology Head and Neck Surgery
- K. J. Lee's Essential Otolaryngology
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery (Vol. 1 & 2)
- Shambaugh Surgery of the Ear
🏥 Family Medicine (3 books)
- Pfenninger and Fowler's Procedures for Primary Care, 3e
- Swanson's Family Medicine Review
- Textbook of Family Medicine, 9e
🔍 Forensic Medicine (6 books)
- Brogdon's Forensic Radiology
- DiMaio's Forensic Pathology, 3e
- Forensic Anthropology - A Comprehensive Introduction, 2e
- P. C. Dikshit Textbook of Forensic Medicine and Toxicology
- Parikh's Textbook of Medical Jurisprudence, Forensic Medicine & Toxicology
- The Essentials of Forensic Medicine and Toxicology, 36e (2026)
🫁 Gastroenterology (3 books)
- Clinical Gastrointestinal Endoscopy, 3e
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease
- Yamada's Textbook of Gastroenterology, 3-Volume Set, 7e
🔪 General Surgery (9 books)
- Bailey and Love's Short Practice of Surgery, 28e
- Current Surgical Therapy, 14e
- Fischer's Mastery of Surgery, 8e
- Maingot's Abdominal Operations
- Mulholland and Greenfield's Surgery, 7e
- Pye's Surgical Handicraft, 22e
- S. Das A Manual on Clinical Surgery, 13e
- Schwartz's Principles of Surgery, 2-Volume Set, 11e
- Sabiston Textbook of Surgery, Biological Basis of Modern Surgical Practice
🧬 Genetics (2 books)
- Emery's Elements of Medical Genetics and Genomics
- Thompson & Thompson Genetics and Genomics in Medicine, 9e
🔬 Histology (2 books)
- Histology: A Text and Atlas (with Cell and Molecular Biology)
- Junqueira's Basic Histology, Text and Atlas, 17e
🛡️ Immunology (3 books)
- Cellular and Molecular Immunology
- Janeway's Immunobiology, 10e
- Roitt's Essential Immunology
🏥 Internal Medicine (7 books)
- Firestein & Kelley's Textbook of Rheumatology, 2-Volume Set
- Frameworks for Internal Medicine
- Goldman-Cecil Medicine, International Edition, 2-Volume Set
- Harrison's Principles of Internal Medicine, 22e (2025)
- Rheumatology, 2-Volume Set (2022, Elsevier)
- Symptom to Diagnosis - An Evidence-Based Guide, 4e
- The Washington Manual of Medical Therapeutics
🧫 Laboratory Medicine (3 books)
- Henry's Clinical Diagnosis and Management by Laboratory Methods
- Quick Compendium of Clinical Pathology, 5e
- Tietz Textbook of Laboratory Medicine, 7e
🦠 Microbiology (3 books)
- Jawetz, Melnick & Adelberg's Medical Microbiology, 28e
- Medical Microbiology, 9e
- Sherris & Ryan's Medical Microbiology, 8e
🫘 Nephrology (3 books)
- Brenner and Rector's The Kidney, 2-Volume Set
- Comprehensive Clinical Nephrology, 7e
- National Kidney Foundation Primer on Kidney Diseases, 8e
🧠 Neurology (4 books)
- Adams and Victor's Principles of Neurology, 12e
- Bradley and Daroff's Neurology in Clinical Practice
- Localization in Clinical Neurology, 8e
- Plum and Posner's Diagnosis and Treatment of Stupor and Coma
🧠 Neuroscience (3 books)
- Eric Kandel's Principles of Neural Science, 6e
- Neuroanatomy Through Clinical Cases, 3e
- Neuroscience: Exploring the Brain, 5e
🤰 Obstetrics & Gynaecology (2 books)
- Berek & Novak's Gynecology
- Creasy & Resnik's Maternal-Fetal Medicine - Principles and Practice
👁️ Ophthalmology (2 books)
- Kanski's Clinical Ophthalmology, 10e
- The Wills Eye Manual, Office and Emergency Room Diagnosis
🦴 Orthopaedics (3 books)
- Campbell's Operative Orthopaedics, 15e (2026)
- Miller's Review of Orthopaedics, 9e
- Rockwood and Green's Fractures in Adults, 10e (2025)
🦠 Pathology (2 books)
- Robbins & Kumar Basic Pathology (Robbins Pathology)
- Robbins, Cotran & Kumar Pathologic Basis of Disease
👶 Paediatrics (2 books)
- Red Book 2021 - Report of the Committee on Infectious Diseases
- The Harriet Lane Handbook (Johns Hopkins Hospital), 23e
💊 Pharmacology (3 books)
- Goodman & Gilman's The Pharmacological Basis of Therapeutics
- Katzung's Basic and Clinical Pharmacology, 16e
- Lippincott Illustrated Reviews: Pharmacology
⚡ Physiology (4 books)
- Costanzo Physiology, 7e
- Ganong's Review of Medical Physiology, 26e
- Guyton and Hall Textbook of Medical Physiology
- Medical Physiology
🧠 Psychiatry (6 books)
- Kaplan & Sadock's Comprehensive Textbook of Psychiatry
- Kaplan and Sadock's Synopsis of Psychiatry
- Stahl's Essential Psychopharmacology
- The Clozapine Handbook
- The Maudsley Deprescribing Guidelines
- The Maudsley Prescribing Guidelines in Psychiatry, 15e
🫁 Pulmonology (2 books)
- Fishman's Pulmonary Diseases and Disorders, 2-Volume Set
- Murray & Nadel's Textbook of Respiratory Medicine, 2-Volume Set
🩻 Radiology (1 book)
- Grainger & Allison's Diagnostic Radiology
🫀 Urology (3 books)
- Campbell Walsh Wein Urology, 3-Volume Set
- Hinman's Atlas of Urologic Surgery
- Smith and Tanagho's General Urology, 19e
How to use the library: Just ask me any medical question - I search across all these books simultaneously and pull the most relevant content to give you a detailed, textbook-referenced answer. Ask about any topic, drug, disease, procedure, or clinical scenario!
Manthappa medicine
Searching the Web
Manthappa medicine textbook India medical students
"Manthappa Medicine" refers to the Manipal Prep Manual of Medicine by Dr. M. Manthappa, a very popular exam-oriented medicine textbook among Indian MBBS students. It is nicknamed "Manthappa" after its author.
About the Book
| Detail | Info |
|---|---|
| Full Title | Manipal Prep Manual of Medicine |
| Author | Dr. M. Manthappa |
| Publisher | CBS Publishers and Distributors |
| Latest Edition | 4th Edition (2026) |
| Format | Q&A / concise exam-focused |
| Also available | Dental students' edition |
What Makes It Popular
- Written in a concise Q&A format, ideal for exam preparation (final MBBS, PG entrance exams like NEET-PG, USMLE-style)
- Covers all major topics in internal medicine in an easy-to-read, actionable style
- Widely used across Indian medical colleges, especially Manipal and affiliated institutions
- Good for quick revision rather than deep conceptual reading
Is It in This Library?
Unfortunately, Manipal Prep Manual of Medicine (Manthappa) is not currently in this textbook library. The library does, however, contain several major internal medicine references that cover the same topics in greater depth:
| Book | Best For |
|---|---|
| Harrison's Principles of Internal Medicine, 22e (2025) | Comprehensive concepts, mechanisms |
| Goldman-Cecil Medicine (2-Vol) | Clinical, exam-relevant |
| The Washington Manual of Medical Therapeutics | Concise, practical management |
| Symptom to Diagnosis (4e) | Evidence-based clinical reasoning |
| Frameworks for Internal Medicine | Structured approach |
If you have a specific topic or question from Manthappa Medicine you'd like answered, I can look it up across all available textbooks and give you a detailed answer. Just ask!
Books pdf
I'm not able to provide PDF downloads of books. The textbooks in this library are licensed for reading and referencing only - I can search them and answer your questions, but cannot distribute the full text or PDF files.
If you're looking for legitimate access to medical textbooks, here are some options:
Legal Ways to Access Medical Books
Free / Open Access
- NCBI Bookshelf - Many free medical textbooks (StatPearls, etc.)
- OpenStax - Free anatomy, biology, and some medical titles
- WHO IRIS - WHO guidelines and health publications
- Internet Archive - Older editions of many textbooks (legally)
Paid / Institutional Access
- Elsevier ClinicalKey - Large collection of medical textbooks
- AccessMedicine (McGraw-Hill) - Harrison's, Goodman & Gilman, etc.
- Thieme MedOne - Anatomy, surgery, neuroscience
- Your university/college library - Most medical schools provide free access to major titles
Affordable Options
- Google Play Books / Kindle - Digital editions at lower cost than print
- Doody's / VitalSource - Medical ebook platforms
What I Can Do Instead
Ask me any medical question and I'll search across 130+ premium textbooks (Harrison's, Braunwald's, Goldman-Cecil, Robbins, Guyton, etc.) and give you a detailed, cited answer - which is often better than flipping through a PDF yourself.
This is a shared conversation. Sign in to Orris to start your own chat.