Cardiac temponde
Reading File
Finding Sources
Finding Sources
Searching PubMed
"cardiac tamponade" management
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive, well-illustrated content from multiple major textbooks. Here is the full clinical overview:
Cardiac Tamponade
Definition
Cardiac tamponade is a life-threatening condition in which elevated intrapericardial pressure (from fluid, blood, pus, or gas accumulating in the pericardial space) compresses the cardiac chambers, impairs diastolic filling, and reduces cardiac output. It exists on a hemodynamic continuum - from subclinical to frank cardiovascular collapse.
- ROSEN's Emergency Medicine, p. 1125
- Fuster and Hurst's The Heart, 15th Ed, p. 1693
Etiology
| Category | Causes |
|---|---|
| Malignancy (32%) | Lung, breast, lymphoma, GI cancers |
| Infection (24%) | Staphylococcus, Streptococcus, TB, HIV |
| Idiopathic (16%) | - |
| Iatrogenic (15%) | Post-cardiac catheterization, post-cardiac surgery, anticoagulants |
| Post-MI (7%) | Cardiac wall rupture (44% of cases) |
| Uremic (4%) | Uremic pericarditis |
- ROSEN's Emergency Medicine, p. 1125
Pathophysiology
The core mechanism is a rise in intrapericardial pressure that exceeds intracardiac filling pressures.
Key concepts:
-
Rate of accumulation matters most: As little as 150 mL of rapidly accumulating fluid (e.g., aortic dissection, iatrogenic perforation) can cause acute tamponade. Conversely, liters of fluid can accumulate slowly (e.g., in uremia) with minimal hemodynamic impact because the pericardium stretches over time.
-
Transmural filling pressure: Normally, low intrapericardial pressure maintains a positive transmural pressure that favors chamber filling. As intrapericardial pressure rises, it must be offset by rising intracardiac pressures. Eventually, transmural pressure becomes negative - chambers collapse during diastole.
-
Equalization of diastolic pressures: Diastolic pressures in all four chambers equalize - a hallmark finding on cardiac catheterization.
-
Ventricular interdependence (the origin of pulsus paradoxus): The total intrapericardial volume is fixed at near-maximum. When the RV fills more with inspiration (increased venous return), it physically crowds the LV, reducing LV stroke volume. This respiratory oscillation in LV output causes pulsus paradoxus.
-
Compensatory tachycardia: The heart initially increases heart rate to maintain cardiac output. This compensation holds until late in the course, followed by rapid decompensation.
- Fuster and Hurst's The Heart, pp. 1693-1694
Clinical Features
Beck's Triad (Classic)
- Hypotension
- Distended neck veins (elevated JVP)
- Muffled heart sounds
Note: The full triad may be absent, especially with rapidly developing tamponade.
Other Signs
-
Dyspnea (most common symptom)
-
Chest pain, cough
-
Pulsus paradoxus: A drop in systolic BP >10 mmHg with inspiration - pathognomonic when >10 mmHg
-
Tachycardia
-
Kussmaul's sign is typically absent (distinguishes tamponade from constrictive pericarditis, where it is present)
-
ROSEN's Emergency Medicine, p. 1125
Investigations
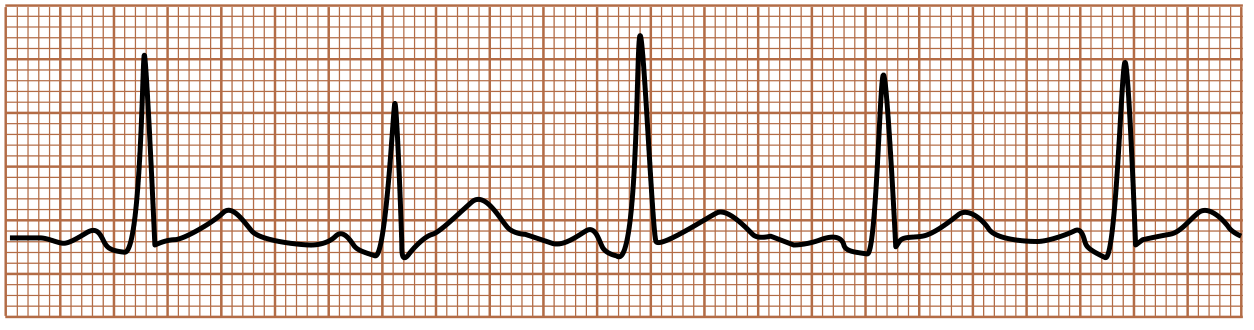
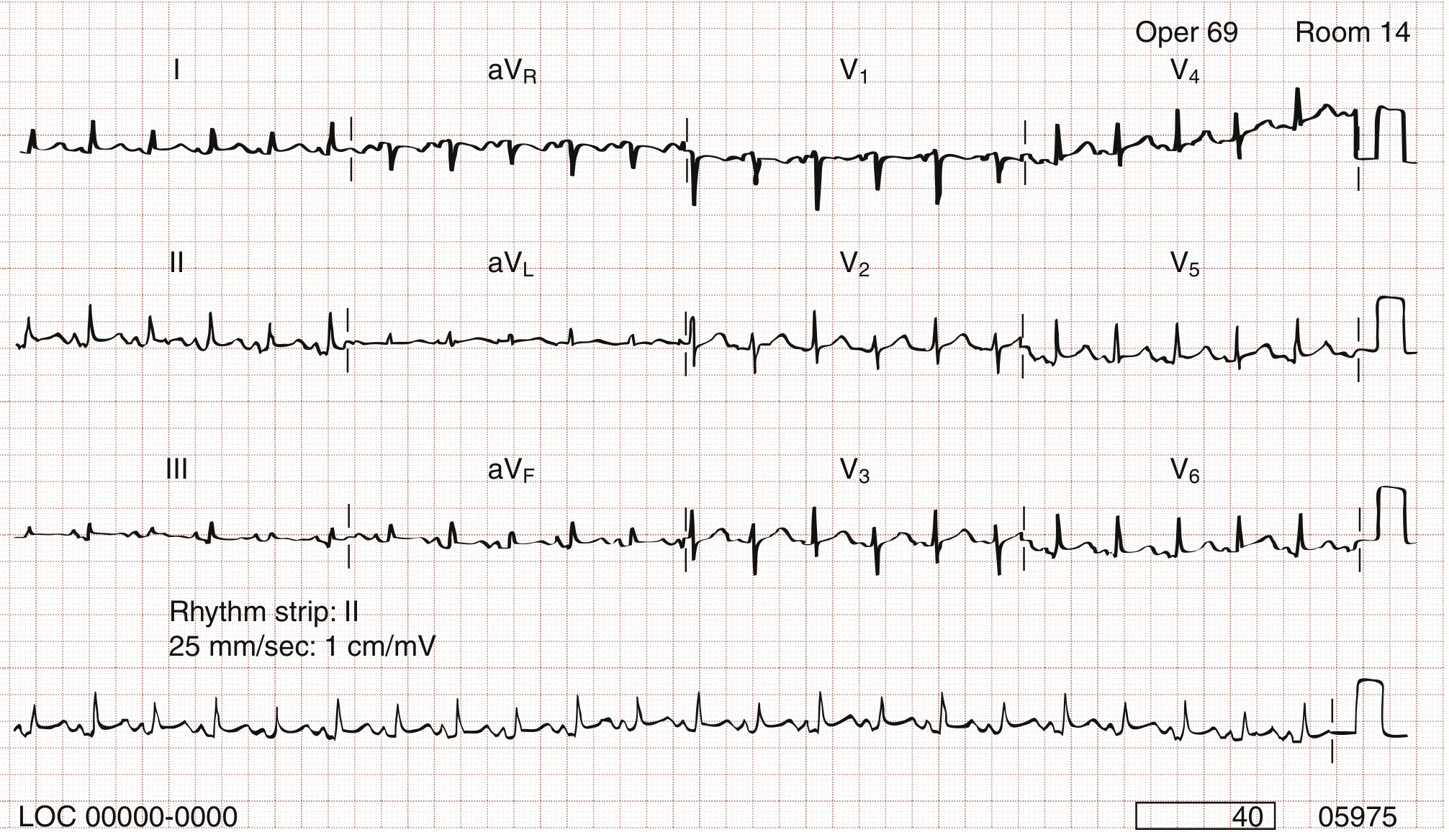
ECG
Two key findings:
1. Low voltage - generalized decrease in QRS amplitude from fluid attenuating electrical signals.
2. Electrical alternans - beat-to-beat alternation in QRS axis and amplitude due to the heart swinging back and forth within the pericardial fluid. Highly specific for tamponade.
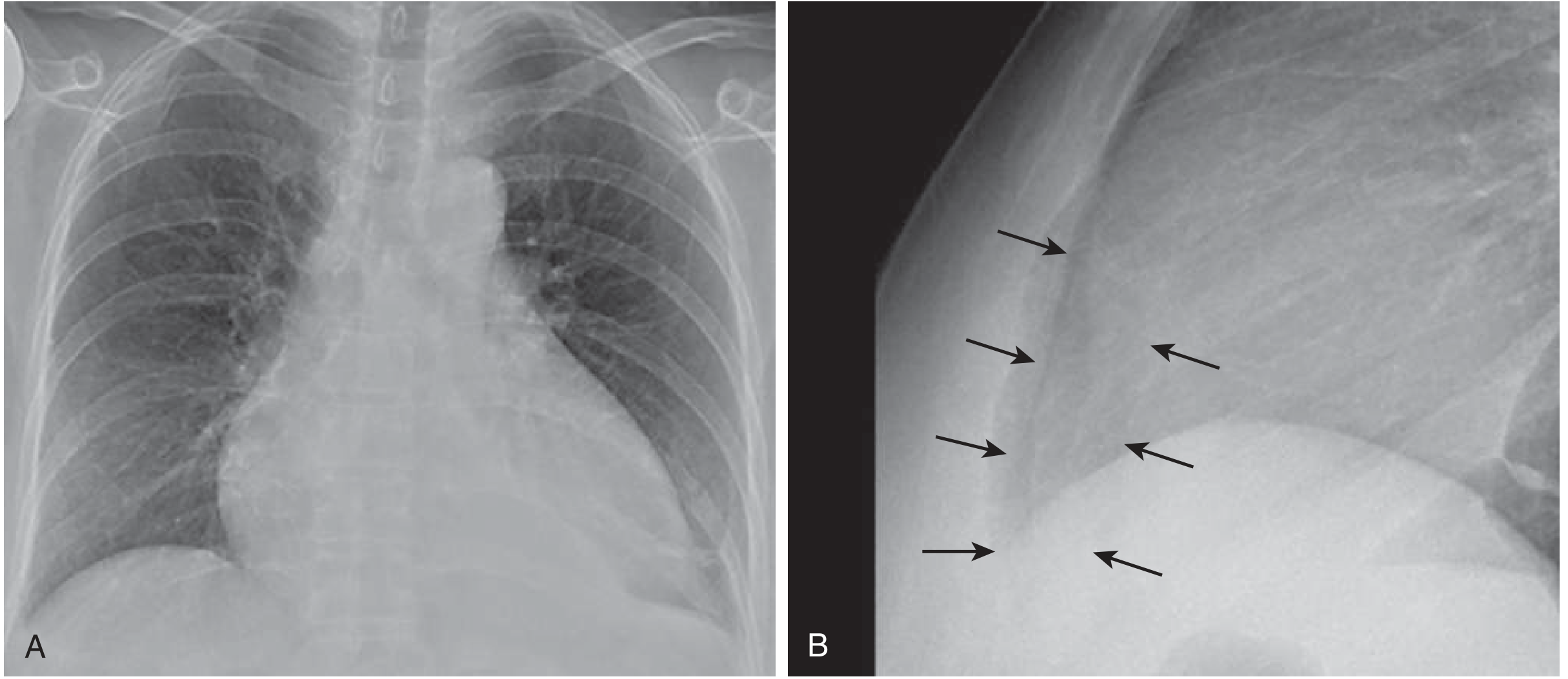
Chest X-Ray
- Cardiomegaly only if >250 mL of pericardial fluid is present
- Classic "water bottle" or "flask-shaped" cardiac silhouette on PA view
- Lateral view: separation between pericardial and epicardial fat stripes
Echocardiography (POCUS) - Gold Standard
Confirms diagnosis by showing:
| Finding | Timing | Sensitivity | Specificity |
|---|---|---|---|
| Right atrial collapse (systolic inversion) | Early | 50-100% | 33-100% (nonspecific) |
| RV diastolic collapse | Later | 48-60% | 75-90% |
| LA/LV collapse | Late | - | High |
| IVC plethora (no respiratory collapse) | - | - | Supports diagnosis |
| Respiratory variation in mitral/tricuspid inflow | - | - | Supports diagnosis |
RA collapse lasting >1/3 of the cardiac cycle improves specificity. RV collapse is more specific than RA collapse.
- Miller's Anesthesia, 10e, p. 5026
Cardiac Catheterization
- Equalization of all four diastolic pressures (RVEDP = LVEDP = mean RA pressure = mean pulmonary capillary wedge pressure)
Management
Temporizing Measures
- IV fluids: Bolus to increase right-sided filling pressure and partially overcome pericardial compression. Useful as a bridge, especially in hypovolemic tamponade.
- Avoid positive pressure ventilation if at all possible: PPV increases intrathoracic pressure, further impairs cardiac filling, and can precipitate cardiovascular collapse.
- Avoid inotropes: There is already maximal endogenous adrenergic stimulation - these are usually ineffective.
- Maintain heart rate: Bradycardia is poorly tolerated; avoid agents that slow heart rate.
Definitive Treatment: Pericardial Drainage
| Method | Indication |
|---|---|
| Echocardiography-guided pericardiocentesis | First-line for most cases; ≥1 cm of fluid anterior to RV free wall throughout diastole. Catheter left in place for continued drainage to minimize recurrence. |
| Surgical drainage / Pericardial window | Effusions <1 cm, organized/multiloculated/focal effusions; recurrent effusions; bacterial pericarditis; when tissue diagnosis needed. Window drains into pleural space to prevent recurrence. |
| Pericardiectomy | Recurrent effusions unresponsive to other drainage methods |
| ED thoracotomy | Penetrating cardiac trauma with instability |
Pericardial fluid analysis should include: LDH, protein, cell count, cytology, PCR for TB, bacterial and TB culture.
- Goldman-Cecil Medicine, p. 718-719
- ROSEN's Emergency Medicine, p. 1125
Special Situations
- Malignant effusions: Frequently recur; pericardial window or percutaneous balloon pericardiotomy is preferred. In-hospital mortality <10%, but subsequent mortality ~75% with malignant cause vs. 3-5%/year for non-malignant causes.
- Post-cardiac surgery tamponade: Echo findings may be atypical (loculated clot, focal compression). Classic respiratory variation findings are unreliable due to PPV.
- Pulmonary hypertension: Right-sided chamber collapse may be absent despite tamponade because baseline right-sided pressures are already elevated.
- "Low-pressure" tamponade: Occurs in volume-depleted states where normal filling pressures are already low; tamponade can occur with relatively small effusions and no classic signs.
Differential Diagnosis
- Constrictive pericarditis (similar hemodynamics, but Kussmaul's sign present, pericardial knock on auscultation, calcification on imaging)
- Cardiogenic shock
- Tension pneumothorax
- Pulmonary embolism (obstructive shock)
- Superior vena cava syndrome
- Dilated cardiomyopathy
Prognosis
-
In-hospital mortality: <10% with prompt drainage
-
Long-term prognosis depends entirely on the underlying cause:
- Malignant effusion: ~75% subsequent mortality
- Non-malignant causes: ~3-5% annual mortality
-
Goldman-Cecil Medicine, p. 719
Recent evidence note: A 2024 systematic review (PMID 39210274) specifically addresses cardiac tamponade in HIV-positive patients, noting TB and opportunistic infections as major causes in that population. A 2025 meta-analysis (PMID 40603759) confirms that point-of-care ultrasound (POCUS) has high diagnostic accuracy for tamponade in shock settings - supporting echo as the gold standard diagnostic tool.
This is a shared conversation. Sign in to Orris to start your own chat.