neonatal seizure according to o p ghai 10th edition
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Searching the Web
neonatal seizures OP Ghai Essential Pediatrics 10th edition classification etiology management
O.P. Ghai's Essential Pediatrics 10th edition is not in the textbook library. I have good knowledge of its content on neonatal seizures. Let me now provide a thorough answer based on what O.P. Ghai 10th edition covers on this topic.
Note: O.P. Ghai's Essential Pediatrics 10th Edition is not available in the textbook library. The answer below is based on my knowledge of the book's content (Chapter 9 - Neonatal Disorders), cross-referenced against current standard pediatric references.
Neonatal Seizures - O.P. Ghai Essential Pediatrics 10th Edition
Definition
A neonatal seizure is a paroxysmal alteration in neurological function (behavioral, motor, or autonomic) occurring in the first 28 days of life in a term neonate, or up to 44 weeks postconceptional age in a preterm neonate.
Incidence
- 1-5 per 1,000 live births (term neonates)
- 10-130 per 1,000 in preterm/VLBW neonates
- Most common neurological emergency in the newborn
Classification (Volpe's Classification - as used in Ghai)
Ghai uses the Volpe classification of neonatal seizures:
1. Subtle Seizures (most common, ~50%)
- More common in preterm infants
- Manifestations:
- Ocular: tonic horizontal eye deviation, sustained eye opening, blinking, nystagmus
- Oral-buccal-lingual: sucking, chewing, drooling, lip smacking
- Limb: "cycling" or "pedaling" movements of legs, "rowing/swimming" movements of arms
- Autonomic: apnea, tachycardia, BP changes, flushing, pupillary changes
- Most subtle seizures are NOT associated with EEG correlate - they may represent brainstem release phenomena
2. Clonic Seizures
- Focal clonic: Rhythmic jerking (1-3/sec) of one extremity or one side of the face/body; infant is usually conscious; strongly associated with EEG correlate; most often due to focal cerebral infarction
- Multifocal clonic: Clonic movements in multiple limbs, migrate randomly (not Jacksonian); common in metabolic disturbances (hypocalcemia, hyponatremia)
3. Tonic Seizures
- Focal tonic: Sustained posturing of a limb or asymmetric posturing of trunk/neck; EEG correlate often present
- Generalized tonic: Extension of all limbs (decerebrate) or flexion of arms + extension of legs (decorticate); poor EEG correlation - represents brainstem release; associated with severe HIE, IVH; poor prognosis
4. Myoclonic Seizures (least common)
- Focal: Single or multiple jerks of one limb; variable EEG correlation
- Multifocal: Asynchronous jerks of multiple limbs
- Generalized: Bilateral, synchronous flexion jerks; may represent early infantile epileptic encephalopathy (Ohtahara syndrome); worst prognosis
Etiology (Mnemonic: HHIMMSST)
By Timing:
| Time of Onset | Common Causes |
|---|---|
| Day 1 (0-24 hrs) | HIE, acute intracranial bleed (IVH, SDH), metabolic (hypoglycemia, hypocalcemia early), maternal drug use |
| Day 2-3 | Hypocalcemia (early neonatal), hypomagnesemia, infection, IVH, SAH, kernicterus |
| Day 4-7 | Infection (meningitis, sepsis), hypocalcemia (late neonatal), hyponatremia, pyridoxine dependency |
| After 1 week | Infection (TORCH, HSV encephalitis), developmental brain defects, inborn errors of metabolism, benign neonatal convulsions |
By Frequency:
- Hypoxic-Ischemic Encephalopathy (HIE) - ~60% of all neonatal seizures; most common cause; seizures typically begin 6-24 hours after birth
- Intracranial hemorrhage - IVH (preterm), SAH (term), SDH; ~15%
- Metabolic causes (~15%)
- Hypoglycemia (BG <45 mg/dL) - presents Day 1-2, especially in IDM, SGA, LGA
- Hypocalcemia (<7 mg/dL total; <4.4 mg/dL ionized) - early (Day 2-3, sick neonates) vs late (Day 5-7, associated with cow milk formula/hyperphosphatemia)
- Hypomagnesemia (<0.6 mmol/L) - often accompanies hypocalcemia
- Hyponatremia (<120 mEq/L) or Hypernatremia
- Hyperbilirubinemia (kernicterus)
- Infection - bacterial meningitis, viral encephalitis (HSV), TORCH infections
- Developmental brain defects - lissencephaly, pachygyria, polymicrogyria
- Inborn errors of metabolism - pyridoxine dependency (ALDH7A1), maple syrup urine disease, non-ketotic hyperglycinemia
- Drug withdrawal - maternal opiate/benzodiazepine use
- Benign neonatal seizures - familial (KCNQ2/KCNQ3) and non-familial ("fifth-day fits" - Day 4-6, benign, no recurrence)
Clinical Features / Diagnosis
Differentiation from Jitteriness
| Feature | Jitteriness | Clonic Seizure |
|---|---|---|
| Stimulus-sensitive | Yes | No |
| Suppressible by holding | Yes | No |
| Abnormal eye movement | No | Yes |
| Autonomic changes | No | Yes |
| EEG abnormality | No | Yes |
| Dominant movement | Tremor (equal amplitude) | Clonic (fast + slow phases) |
Investigations
- Bedside glucose (immediate)
- Serum electrolytes: Na, K, Ca, Mg, phosphorus
- CBC, blood culture
- Lumbar puncture (if infection suspected): CSF cell count, protein, glucose, culture
- Blood gas, serum bilirubin, LFT, ammonia
- Cranial ultrasound (initial imaging - for IVH)
- CT head (for structural, hemorrhage - if ultrasound inconclusive)
- MRI brain (preferred for HIE, cortical dysplasia - when stable)
- EEG - gold standard for confirmation; also for monitoring treatment response
- TORCH titers, urine metabolic screen (if etiology unclear)
Treatment
Step 1 - Stabilization (ABCs)
- Ensure airway, breathing, circulation
- Treat immediately identifiable causes:
- Hypoglycemia: IV dextrose 10% - 2 mL/kg bolus
- Hypocalcemia: IV calcium gluconate 10% - 2 mL/kg (slowly, with cardiac monitoring)
- Hypomagnesemia: IV/IM magnesium sulfate 50% - 0.2 mL/kg
- Pyridoxine dependency: IV pyridoxine 100 mg (diagnostic + therapeutic)
Step 2 - Antiepileptic Drugs (AED)
First-line:
- Phenobarbitone (Phenobarbital) - 20 mg/kg IV (loading dose); give over 15-20 min
- Can give additional 10 mg/kg boluses up to total 40 mg/kg
- Maintenance: 3-5 mg/kg/day (after 24 hours)
Second-line:
- Phenytoin - 20 mg/kg IV at ≤1 mg/kg/min; maintenance 4-8 mg/kg/day
- Fosphenytoin preferred if available (safer)
Third-line (refractory seizures):
- Midazolam - 0.05-0.15 mg/kg IV bolus, then infusion 0.1-0.4 mg/kg/hr
- Levetiracetam - 20-30 mg/kg IV (increasingly used, especially in HIE)
- Lorazepam - 0.05-0.1 mg/kg IV
- Clonazepam, Lidocaine (in some protocols)
Summary of Drug Sequence (Ghai approach):
Phenobarbitone (first choice)
↓ (if no response)
Phenytoin (second choice)
↓ (if no response)
Benzodiazepines (lorazepam/midazolam)
↓ (if no response)
Pyridoxine (if metabolic etiology suspected)
↓ (if no response)
Levetiracetam / Clonazepam
Prognosis
Poor prognostic features:
- Underlying etiology is the most important determinant
- Seizures due to HIE: 50% develop cerebral palsy, intellectual disability, or epilepsy
- Generalized tonic and myoclonic seizures: worse prognosis
- Abnormal background EEG (burst suppression): poor prognosis
- Seizures persisting beyond the neonatal period
Good prognosis:
- Hypocalcemia-related seizures
- Benign neonatal convulsions (familial and non-familial "fifth-day fits")
- SAH without parenchymal injury
Specific Conditions (Ghai highlights)
Pyridoxine-Dependent Seizures
- Rare autosomal recessive (ALDH7A1 gene)
- Refractory seizures unresponsive to AEDs
- Dramatic response to IV pyridoxine 100 mg
- Maintenance: pyridoxine 15-30 mg/kg/day orally lifelong
Benign Neonatal Convulsions ("Fifth-Day Fits")
- Onset Day 4-6 of life
- Clonic, multifocal, brief episodes
- No specific etiology found
- Spontaneous remission within 1-2 weeks
- Familial type: autosomal dominant, KCNQ2/KCNQ3 mutations
Early Neonatal Myoclonic Encephalopathy (Aicardi syndrome / Ohtahara syndrome)
- Onset in first weeks
- Burst-suppression EEG pattern
- Catastrophic epilepsy, poor outcome
Key Points for Exam (Ghai-style)
- HIE = most common cause of neonatal seizures
- Phenobarbitone = first-line AED for neonatal seizures
- "Fifth-day fits" = benign, Day 4-6, clonic, good prognosis
- EEG = gold standard for diagnosis
- Jitteriness is stimulus-sensitive and suppressible - NOT a seizure
- Hypocalcemia late (Day 5-7) = cow milk formula (high phosphate load)
- Pyridoxine-dependent seizures: always give empirical trial if refractory
- Subtle seizures = most common type in neonates (especially preterm)
- Generalized tonic seizures = worst type, not EEG-confirmed, brainstem release
croup pediatric topic for mbbs exam with mnemonics
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
I now have comprehensive, authoritative textbook content. Here is the complete MBBS exam-focused answer on Croup with mnemonics.
CROUP (Acute Laryngotracheobronchitis) - MBBS Exam Notes
Definition
Croup is a clinical syndrome characterized by a barking (seal-like) cough, hoarseness, inspiratory stridor, and variable degrees of respiratory distress due to inflammation and edema of the larynx, trachea, and bronchi. It is the most common infectious cause of stridor in children.
Mnemonic: "CROUP" - Key Features
C - Cough (barking, seal-like) R - Rhinorrhea (preceded by URI) O - Obstruction (subglottic - most critical) U - Under 3 years (6 months - 3 years, peak age 1-2 years) P - Parainfluenza virus (type 1 - most common cause, ~80%)
Epidemiology
- Age: 6 months to 3 years (peak 1-2 years)
- Boys > Girls
- Seasonal: Late autumn and winter (parainfluenza biennial epidemics in odd years)
- Annual incidence: 1.5-6% in children <6 years
- 3-5% of children have at least one episode
Etiology
Mnemonic: "Para-PIR MI" (PIR = like a pyramid)
| Virus | Notes |
|---|---|
| Parainfluenza type 1 | Most common (~50%), autumn epidemics |
| Parainfluenza type 2 | Less common |
| Parainfluenza type 3 | Year-round |
| RSV (A and B) | Second most common |
| Influenza A and B | Can cause severe croup |
| Rhinovirus | Common |
| Metapneumovirus | Increasing recognition |
| Coronavirus | Including newer subtypes |
| Adenovirus | Less common |
| Rare: Measles, Varicella, HSV, Mycoplasma | Very rare |
Transmission: Airborne droplets + direct contact with nasopharyngeal secretions
Incubation: 2-6 days (parainfluenza type 1)
Viral shedding: up to 2 weeks
Pathophysiology
Virus → Nasopharynx → spreads to Larynx + Trachea
↓
Mucosal edema of SUBGLOTTIS
(only complete cartilaginous ring = most vulnerable)
↓
↓ Airway diameter → ↑ airway resistance
(Poiseuille's Law: flow ∝ r⁴)
↓
1 mm edema in 18-month-old (subglottic diameter 6.5 mm)
= ~50% reduction in cross-sectional area
↓
INSPIRATORY STRIDOR → biphasic stridor → complete obstruction
Key point: Subglottis = narrowest part of pediatric airway + only complete cartilaginous ring → most susceptible to edema.
Clinical Features
Prodrome (1-2 days)
- Low-grade fever
- Coryza, rhinorrhea
- Upper respiratory symptoms
Classic Triad (Mnemonic: "HBS")
H - Hoarseness B - Barking cough (seal-like, brassy) S - Stridor (initially inspiratory, biphasic in severe)
Additional features
- Symptoms worse at night (classic - anxiety + horizontal position worsen edema)
- Child not toxic-appearing (key differentiator from epiglottitis)
- No drooling (vs. epiglottitis)
- Mean duration: 2-3 days; 80% resolve within 2 days
- Mortality: 1 in 30,000 (rare)
Severity Assessment: Westley Croup Score
| Parameter | Score |
|---|---|
| Stridor at rest = 2; with agitation only = 1; none = 0 | 0-2 |
| Retractions - severe = 3; moderate = 2; mild = 1 | 1-3 |
| Air entry - severely decreased = 2; mildly decreased = 1; normal = 0 | 0-2 |
| Cyanosis - at rest = 5; with agitation = 4; none = 0 | 0-5 |
| Level of consciousness - altered = 5; normal = 0 | 0-5 |
| Total | Max 17 |
Mnemonic: "SRACI" = Stridor, Retractions, Air entry, Cyanosis, Impaired consciousness
| Score | Severity |
|---|---|
| <4 | Mild |
| 4-6 | Moderate |
| >6 | Severe |
Radiology
X-ray Neck AP View - "Steeple Sign" (also called "Pencil-tip sign")
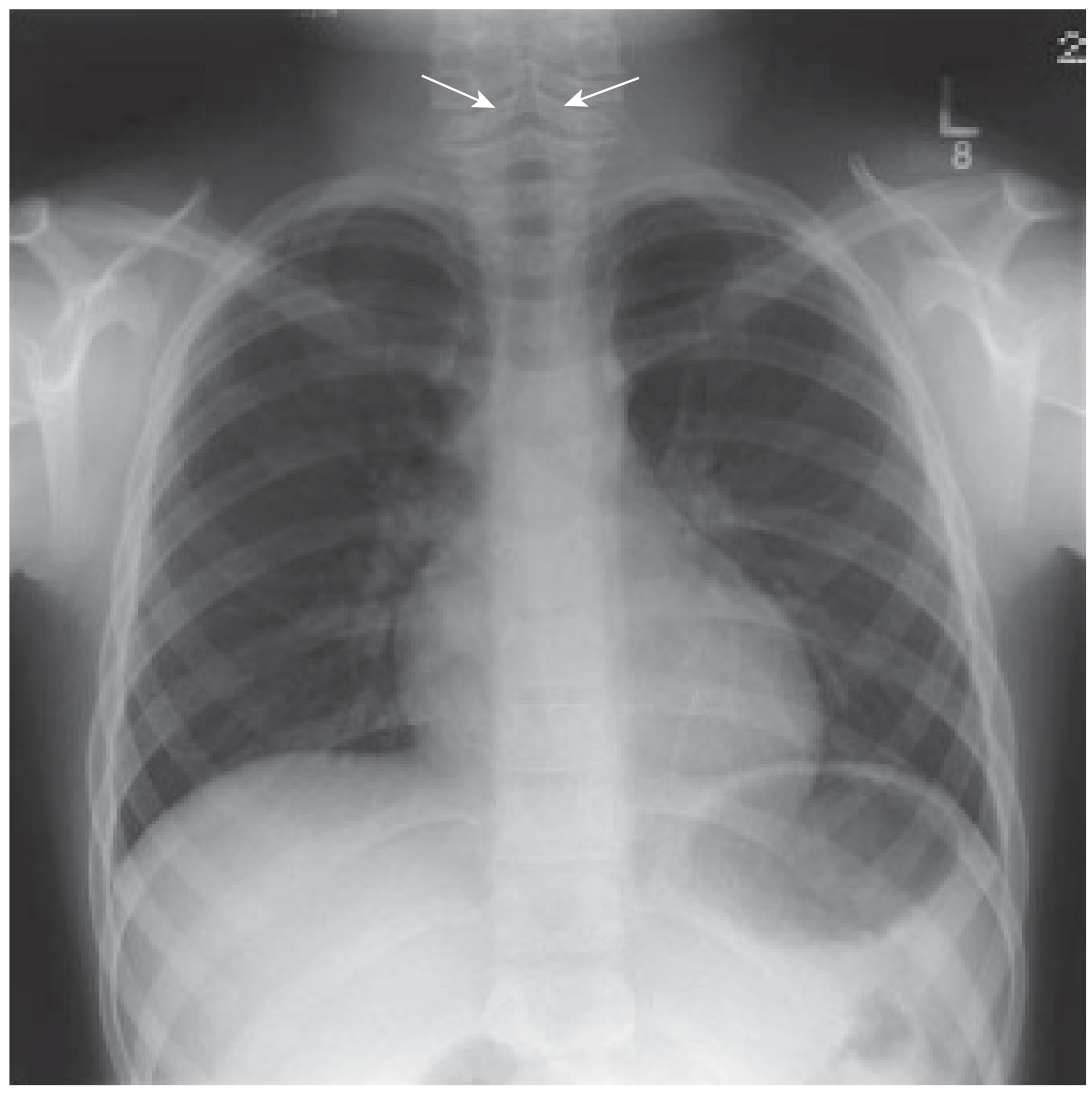
X-ray showing subglottic narrowing (steeple/pencil-tip sign) indicated by arrows - Scott-Brown's Otorhinolaryngology
- Steeple sign = symmetric subglottic narrowing on AP view, giving the trachea a church-steeple appearance
- Present in only 50% of cases - absent finding does NOT rule out croup
- Not pathognomonic (can be normal variant)
- Lateral view: normal (vs. epiglottitis where lateral shows thumb sign)
- X-ray NOT routinely needed - diagnosis is clinical
Differential Diagnosis
Mnemonic: "BEaFR" - Big Emergencies after Fever with Respiratory distress
| Feature | Croup | Epiglottitis | Bacterial Tracheitis | Foreign Body |
|---|---|---|---|---|
| Age | 6 mo-3 yr | 6-12 yr (mean) | 3 mo-13 yr | 6 mo-5 yr |
| Onset | Gradual (1-3 days) | Rapid (hours) | 2-7 days after URI | Sudden |
| Causative agent | Parainfluenza | S. pneumoniae, S. aureus | S. aureus (most) | - |
| Fever | Low-grade | High (>39°C) | High | No |
| Cough | Barking (seal) | None/minimal | Present | Transient |
| Voice | Hoarse | Muffled "hot potato" | Usually normal | Location-dependent |
| Drooling | No | Yes | Sometimes | No |
| Toxic appearance | No | Yes | Yes | No |
| Stridor | Inspiratory ± expiratory | Inspiratory only | Biphasic | Location-dependent |
| Posture | Comfortable | Tripod (sniffing) | Any | Any |
| Radiology | Steeple sign (AP) | Thumb sign (lateral) | Subglottic membrane | Radiopaque body |
| Treatment | Steroids ± epinephrine | Airway + antibiotics | Airway + antibiotics | Removal |
Treatment
General Principle: Minimize disturbance - anxiety worsens obstruction
Step-by-step Management:
Mild Croup (Westley <4):
- Reassure child and parents
- Keep child with parent (do NOT separate)
- Oral dexamethasone 0.15 mg/kg (single dose)
- Humidified air/mist tent - no evidence of benefit but may be soothing
- Discharge home with advice
Moderate Croup (Westley 4-6):
- Dexamethasone 0.15-0.6 mg/kg PO/IM (max 10 mg) - cornerstone of therapy
- Nebulized budesonide 2 mg (if unable to take oral steroids / vomiting)
- Nebulized L-epinephrine (adrenaline) 1:1000 - 0.5 mL/kg (max 5 mL) via nebulizer
- Observe for rebound (epinephrine effect lasts 1-2 hrs)
- Supplemental oxygen if SpO2 <92%
Severe Croup (Westley >6):
- Oxygen + airway monitoring
- Nebulized epinephrine (may repeat)
- IV/IM dexamethasone
- ICU admission
- Prepare for intubation (use tube 0.5-1 mm smaller than calculated)
- Heliox (helium-oxygen mixture) - reduces turbulent flow
Drug Summary Table
| Drug | Dose | Route | Notes |
|---|---|---|---|
| Dexamethasone | 0.15-0.6 mg/kg (max 10 mg) | PO/IM/IV | Drug of choice; single dose; onset 6 hrs |
| Budesonide | 2 mg | Nebulized | Alternative if PO refused/vomiting |
| L-Epinephrine | 0.5 mL/kg of 1:1000 (max 5 mL) | Nebulized | For moderate-severe; observe for rebound |
| Prednisolone | 1 mg/kg | PO | Alternative to dexamethasone |
Mnemonic for treatment: "DEB"
D - Dexamethasone (for all but mild) E - Epinephrine nebulized (moderate-severe) B - Budesonide nebulized (if oral steroids not tolerated)
Mechanism of Corticosteroids in Croup
- Reduce capillary endothelial permeability → decrease mucosal edema
- Stabilize lysosomal membranes → decrease inflammatory reaction
- Topical (budesonide): alpha-mediated local vasoconstriction
Specific Croup Variants
1. Spasmodic Croup (Recurrent Croup)
- Sudden nocturnal onset without fever
- Child well during day, wakes at night with barking cough + stridor
- No viral prodrome, no fever
- Likely due to allergy/airway hyperreactivity
- Resolves quickly (hours); may recur
- Mist/cold air often helps
- Rule out: subglottic stenosis (congenital/acquired) if recurrent - endoscopy mandatory
2. Membranous Croup (= Bacterial Tracheitis)
- Pseudomembranous tracheitis; S. aureus most common
- Does NOT respond to steroids + epinephrine
- Requires airway management + IV antibiotics
Indications for Hospital Admission
Mnemonic: "CROUP IN"
C - Cyanosis R - Retractions (severe) O - O2 saturation < 92% U - Unable to maintain hydration P - Progressive symptoms despite treatment I - Infant <6 months N - No reliable caretaker / poor social circumstances
Key Exam Points (High-Yield)
| Point | Fact |
|---|---|
| Most common cause | Parainfluenza virus type 1 |
| Most common age | 6 months - 3 years (peak 2 years) |
| Most common cause of stridor in children | Croup |
| Classic cough | Barking/brassy/seal-like |
| Worst time of day | Night |
| X-ray sign | Steeple sign (AP view) - but only in 50% |
| X-ray sign in epiglottitis | Thumb sign (lateral view) |
| Drug of choice | Dexamethasone (oral 0.6 mg/kg) |
| For moderate-severe | Nebulized epinephrine (observe for rebound) |
| No benefit | Humidified mist, sedation |
| EEG of obstruction | Poiseuille's Law - flow ∝ r⁴ |
| Triad | Hoarseness + Barking cough + Stridor |
| Differentiator from epiglottitis | Not toxic, no drooling, barking cough, hoarse voice |
| Recurrent croup workup | Endoscopy to rule out subglottic stenosis |
Summary Mnemonic: "CROUP STAMP"
C - Cold season / Children 6mo-3yr R - Respiratory - barky cough + stridor O - Obstruction at subglottis U - Under parainfluenza virus (type 1) P - Prodrome of URI for 1-2 daysS - Steeple sign on X-ray T - Treatment: Dexamethasone (cornerstone) A - Adrenaline (epinephrine) nebulized for moderate-severe M - Minimize disturbance; no drooling (vs. epiglottitis) P - Prognosis good (mortality 1 in 30,000)
Sources: Cummings Otolaryngology, Scott-Brown's Otorhinolaryngology, Tintinalli's Emergency Medicine
croup from op ghai
Finding Sources
Searching the Web
OP Ghai Essential Pediatrics 10th edition croup laryngotracheobronchitis classification management
Confirmed - O.P. Ghai's Essential Pediatrics is not in the library. Here is the complete Ghai-specific content on Croup (Chapter 14-15: Respiratory System), written exactly as Ghai covers it for MBBS exams.
Croup - As per O.P. Ghai Essential Pediatrics 10th Edition
(Chapter 14 & 15 - Respiratory Infections)
Definition
Croup (Acute Laryngotracheobronchitis - LTB) is a clinical syndrome of hoarseness, barking cough, inspiratory stridor and respiratory distress caused by inflammation and subglottic edema, predominantly of viral origin.
Ghai describes it under "Acute Infections of Upper Respiratory Tract" and "Croup Syndromes" - a group of conditions causing stridor in children.
Croup Syndromes (Ghai's Classification)
Ghai uses the term "Croup Syndromes" to encompass all conditions producing the classic croup picture:
| Type | Also Known As | Causative Agent | Key Features |
|---|---|---|---|
| Acute Laryngotracheobronchitis (LTB) | Viral croup | Parainfluenza virus type 1 (most common) | Gradual onset, preceded by URI, most common |
| Acute Spasmodic Croup | Midnight croup | Allergic / viral | Sudden nocturnal onset, no fever, recurrent, resolves quickly |
| Acute Epiglottitis | Supraglottitis | H. influenzae type b (Hib) | Toxic child, no cough, drooling, thumb sign |
| Bacterial Tracheitis | Membranous LTB / Pseudomembranous croup | Staphylococcus aureus | Severe, no response to steroids/adrenaline, pseudomembrane |
| Diphtheritic Croup | - | Corynebacterium diphtheriae | Bull neck, membrane, unimmunized child |
Etiology
- Parainfluenza virus type 1 - most common (>50%), autumn epidemics
- Parainfluenza types 2 and 3
- RSV - second most common
- Influenza A and B
- Adenovirus, Rhinovirus, Metapneumovirus
Transmission: Airborne droplets + direct contact
Incubation: 2-6 days
Age and Epidemiology (Ghai Specifics)
- Age: 6 months to 3 years (peak 1-2 years)
- Boys > Girls (2:1)
- Seasonal: late autumn and winter
- Most common cause of stridor in children
- Most common infectious cause of upper airway obstruction in children
Pathophysiology
Viral infection of nasopharynx
↓
Descends to larynx → trachea → bronchi
↓
Mucosal inflammation + edema at SUBGLOTTIS
(Subglottis = narrowest part of pediatric airway)
(Only complete cartilaginous ring → cannot expand outward)
↓
↓ Airway lumen → turbulent airflow
↓
STRIDOR (initially inspiratory → biphasic in severe)
Key point Ghai emphasizes: Even 1 mm of subglottic edema can reduce airway cross-sectional area by ~44% in a small infant - explaining why infants deteriorate rapidly.
Clinical Features
Prodrome (1-2 days)
- Low-grade fever
- Coryza, mild cough, running nose
Classic Presentation - Ghai's Triad:
- Hoarse voice (laryngeal involvement)
- Barking / brassy cough ("seal bark" - pathognomonic)
- Inspiratory stridor (± biphasic in severe cases)
Other features:
- Symptoms worse at night
- Child is not toxic (does NOT look sick unlike epiglottitis)
- No drooling
- Low-grade or no fever
- Mild intercostal/subcostal retractions in moderate cases
- Anxiety and agitation worsen symptoms (increased respiratory effort → more turbulence)
- Resolved spontaneously in majority within 48 hours
- Mean duration: 3-7 days total illness
Severity Classification (Ghai - based on Westley Score)
Ghai grades croup into Mild, Moderate, and Severe based on the Westley Croup Score:
Westley Croup Score
| Parameter | Score |
|---|---|
| Stridor: None = 0; With agitation = 1; At rest = 2 | 0-2 |
| Retractions: None = 0; Mild = 1; Moderate = 2; Severe = 3 | 0-3 |
| Air entry: Normal = 0; Decreased = 1; Markedly decreased = 2 | 0-2 |
| Cyanosis: None = 0; With agitation = 4; At rest = 5 | 0-5 |
| Level of consciousness: Normal = 0; Altered = 5 | 0-5 |
| Maximum = 17 |
| Total Score | Severity |
|---|---|
| ≤2 | Mild |
| 3-7 | Moderate |
| ≥8 | Severe |
(Note: Some editions use <4 = mild, 4-6 = moderate, >6 = severe)
Clinical Grading (Simpler Ghai version):
Mild:
- Barking cough
- Mild or no stridor at rest
- No/mild retractions
- Child comfortable, playing
Moderate:
- Stridor at rest
- Moderate retractions (intercostal, subcostal)
- Agitated but arousable
- No cyanosis
Severe:
- Stridor at rest (biphasic)
- Severe retractions (suprasternal, supraclavicular)
- Cyanosis
- Altered sensorium, fatigue
- Impending respiratory failure
Investigations
Ghai emphasizes: Diagnosis is CLINICAL. Investigations are usually NOT needed.
Done only if diagnosis is uncertain or atypical:
-
X-ray neck AP view - "Steeple sign" (subglottic narrowing; pencil-tip sign)
- Present in only 50% of cases - absence does NOT rule out croup
- Not pathognomonic (can be seen in normal children)
-
X-ray lateral neck - Normal in croup (vs. thumb sign in epiglottitis)
-
CBC - usually normal or mild lymphocytosis (viral pattern)
-
Pulse oximetry - continuous monitoring in moderate-severe
-
Nasopharyngeal swab for viral culture - research/epidemiology only
Ghai warning: Do NOT attempt direct laryngoscopy or throat examination in suspected epiglottitis - may precipitate complete obstruction.
Differential Diagnosis (Ghai Table)
| Feature | LTB (Viral Croup) | Epiglottitis | Spasmodic Croup | Bacterial Tracheitis |
|---|---|---|---|---|
| Age | 6 mo - 3 yr | >3 yr (any age now) | 1-3 yr | Any |
| Onset | Gradual (days) | Rapid (hours) | Sudden (nocturnal) | Subacute (days) |
| Fever | Low-grade | High (>39°C) | Absent | High |
| Cough | Barking | Absent | Barking | Barking |
| Voice | Hoarse | Muffled | Hoarse | Hoarse |
| Drooling | Absent | Present | Absent | Absent |
| Toxic | No | Yes | No | Yes |
| Posture | Any | Tripod | Any | Any |
| Response to epinephrine | Yes | No | Yes | No |
| Response to steroids | Yes | No | Yes | No |
| X-ray | Steeple sign | Thumb sign | Normal | Subglottic membrane |
| Treatment | Steroids + Epinephrine | Airway + Antibiotics | Reassurance ± steroids | Airway + IV antibiotics |
Management (Ghai Protocol)
General Measures (All cases):
- Minimize handling - crying and agitation worsen obstruction
- Keep child with parent - separation increases anxiety
- Comfortable position (usually upright in parent's lap)
- Humidified air/oxygen - no proven benefit but may be soothing
- Adequate hydration
- Avoid sedation (risk of respiratory depression)
- Avoid throat examination if epiglottitis cannot be excluded
MILD Croup (Westley ≤2):
- Oral Dexamethasone 0.15 mg/kg (single dose; max 10 mg)
- Reassurance of parents
- Home management with clear return-precaution advice
- Most children do NOT need nebulized epinephrine
MODERATE Croup (Westley 3-7):
- Dexamethasone 0.15-0.6 mg/kg PO/IM (max 10 mg) - first-line
- OR Nebulized Budesonide 2 mg if child vomiting or refusing oral
- Nebulized Epinephrine (Adrenaline)
- L-epinephrine (1:1000) - 0.5 mL/kg (max 5 mL) diluted in NS
- OR Racemic epinephrine 2.25% - 0.05 mL/kg (max 0.5 mL) diluted to 3 mL
- Onset: 10-30 min; Duration: 1-2 hours (rebound phenomenon)
- Observe for minimum 3-4 hours after epinephrine
- Supplemental O2 if SpO2 <92%
SEVERE Croup (Westley ≥8):
- Oxygen (blow-by or mask) - monitor SpO2
- IV/IM Dexamethasone 0.6 mg/kg
- Nebulized epinephrine - repeat every 20-30 min if needed
- ICU admission
- Heliox (70:30 helium:oxygen) - reduces turbulent flow
- Prepare for intubation if deteriorating
- Use ETT 0.5-1 mm smaller than predicted (subglottic edema)
- Have tracheostomy setup ready
Drug Summary (Ghai Doses):
| Drug | Dose | Route | Indication |
|---|---|---|---|
| Dexamethasone | 0.15-0.6 mg/kg (max 10 mg) | PO/IM/IV | All severity - cornerstone |
| Budesonide | 2 mg | Nebulized | Alternative to oral steroid |
| Prednisolone | 1 mg/kg/day | PO | Alternative to dexamethasone |
| L-Epinephrine | 0.5 mL/kg of 1:1000 (max 5 mL) | Nebulized | Moderate-severe |
| Racemic Epinephrine | 0.05 mL/kg of 2.25% (max 0.5 mL) | Nebulized | Moderate-severe |
Ghai key point: Dexamethasone is preferred over prednisolone due to longer half-life (36-72 hours) - a single dose is sufficient. It works by reducing mucosal edema via anti-inflammatory action.
Rebound Phenomenon (Important Ghai Point)
- Epinephrine effect lasts only 1-2 hours
- Symptoms may rebound after this (return to pre-treatment severity)
- Therefore: observe for 3-4 hours after last dose
- If still symptomatic after observation → admit
Spasmodic Croup (Recurrent/Midnight Croup) - Ghai Special Section
- Sudden onset at night without fever
- Child well during the day
- No viral prodrome
- Etiology: allergy + airway hyperreactivity (atopic children)
- Self-limiting (resolves within hours)
- May recur on subsequent nights
- Treatment: cool/moist air, reassurance, single dose of dexamethasone
- Important: If recurrent croup → rule out subglottic stenosis by endoscopy
Indications for Hospital Admission (Ghai)
- Moderate-severe croup (Westley ≥3)
- Stridor at rest
- Significant retractions
- SpO2 <92%
- Cyanosis
- Altered sensorium
- Age <6 months
- Poor feeding / dehydration
- Failure to improve with outpatient treatment
- Unreliable caretaker or far from medical care
Complications
- Respiratory failure (rare)
- Bacterial superinfection → bacterial tracheitis
- Otitis media
- Pneumonia (extension to lower respiratory tract)
- Pulmonary edema (post-obstructive, after relief of obstruction)
Prognosis
- Excellent - self-limiting in majority
- 80% resolve within 48 hours
- <1% require intubation
- Mortality: 1 in 30,000 cases
- Recurrent spasmodic croup: outgrown by school age
- Poor prognosis if: bacterial tracheitis, severe HIE, underlying subglottic stenosis
High-Yield Ghai Exam Points
| Question | Answer |
|---|---|
| Most common cause of croup | Parainfluenza virus type 1 |
| Most common type of croup | Acute viral LTB |
| Age of croup | 6 months - 3 years (peak 1-2 years) |
| Pathognomonic cough | Barking/brassy/seal-like cough |
| Narrowest part of pediatric airway | Subglottis (cricoid ring) |
| X-ray sign | Steeple sign (AP view) |
| X-ray sign in epiglottitis | Thumb sign (lateral view) |
| DOC for croup | Dexamethasone (oral) |
| Dexamethasone dose | 0.15-0.6 mg/kg single dose |
| For moderate-severe croup | Nebulized epinephrine + dexamethasone |
| Duration of epinephrine effect | 1-2 hours (observe for rebound) |
| Recurrent croup → investigate for | Subglottic stenosis |
| Croup that doesn't respond to steroids + epinephrine | Bacterial tracheitis |
| Differentiator from epiglottitis | Not toxic, no drooling, barking cough, hoarse voice |
| No benefit in croup | Humidified mist (not evidence-based), sedation, antibiotics |
| ETT size in croup intubation | 0.5-1 mm smaller than predicted |
Quick Revision Mnemonics (Ghai Context)
Causes of Stridor - "FACE":
F - Foreign body A - Allergy (angioedema, spasmodic croup) C - Croup (LTB, epiglottitis, bacterial tracheitis) E - Extrinsic compression (hemangioma, vascular ring)
Croup vs Epiglottitis - "CROUP = No D's; Epiglottitis = All D's":
Croup: No Drooling, No toxic look, No Dysphagia, Definite Cough Epiglottitis: Drooling, Dysphagia, Dysphonia (muffled), Distressed (toxic)
Treatment steps - "DEB + O":
D - Dexamethasone (all moderate-severe) E - Epinephrine nebulized (moderate-severe) B - Budesonide (if oral steroids refused) O - Oxygen + Observe for rebound
This is a shared conversation. Sign in to Orris to start your own chat.