Diaphyseal aclasia
Reading File
Finding Sources
Finding Sources
Searching PubMed
hereditary multiple exostoses diaphyseal aclasia
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive textbook material. Let me compile the full answer.
Diaphyseal Aclasia (Hereditary Multiple Exostoses)
Synonyms: Hereditary multiple exostoses (HME), multiple osteochondromatosis, diaphyseal aclasis
Definition
Diaphyseal aclasia is a rare autosomal dominant disorder of bone remodeling characterized by the formation of multiple osteochondromas (cartilage-capped bony outgrowths) arising from the metaphyses of long bones. The term "aclasis" reflects the failure of normal bone modeling - excess metaphyseal bone is not resorbed and instead forms irregular exostoses. - Grainger & Allison's Diagnostic Radiology, p. 1009; S Das Manual of Clinical Surgery p. 7990
Genetics
| Feature | Detail |
|---|---|
| Inheritance | Autosomal dominant |
| Genes involved | EXT1 (chr 8q24, MIM 608177) and EXT2 (chr 11p11, MIM 133701) |
| Frequency | 1-2 per 100,000 |
| Mechanism | EXT1/EXT2 encode components of a growth plate complex that enhances Indian hedgehog (IHH) signaling in proliferating chondrocytes |
| Phenotypic variation | Exostoses may be apparent at birth in some; obligate carriers may have seemingly absent lesions |
EXT1 mutation is associated with a greater burden of disease and higher malignancy risk. - Miller's Review of Orthopaedics p. 858; Rheumatology (Elsevier, 2022) p. 1959
Pathophysiology
The condition can be regarded as a disease of the growth plate. Normally, metaphyseal bone is progressively resorbed as the bone elongates. In diaphyseal aclasia, this resorption fails, and ectopic cartilage-bone outgrowths form, protruding from the metaphyseal surface. These exostoses are covered by a thin cartilage cap (analogous to the perichondrium) and grow away from the adjacent joint. - Grainger & Allison, p. 1009
Clinical Features
Sites of predilection (in decreasing frequency):
- Around the knee (~40%) - distal femur, proximal tibia/fibula
- Upper humerus
- Lower ends of radius and ulna
- Above the ankle
- Proximal femur
- Occasionally flat bones (ilium, scapula)
Clinical photograph of diaphyseal (metaphyseal) aclasis - arrows indicate multiple exostoses:

Fig. 11.6 - Diaphyseal (metaphyseal) aclasis. Arrows indicate the exostoses. (S Das Manual of Clinical Surgery)
Complications:
- Shortening and deformity of limbs (when exostoses interfere with epiphyseal growth)
- Mechanical obstruction to joints, muscles, tendons
- Neurovascular compression
- Adventitial bursa formation overlying exostoses
- Malignant transformation (see below)
Radiology
X-ray features:
- Sessile or pedunculated exostoses projecting from the metaphyseal cortex
- Exostoses point away from the adjacent joint
- Medullary cavity of the lesion is continuous with the medullary cavity of the host bone (key diagnostic feature)
- Metaphyses are typically widened and dysplastic compared to solitary osteochondroma
Radiographs showing osteochondroma types and HME pattern:
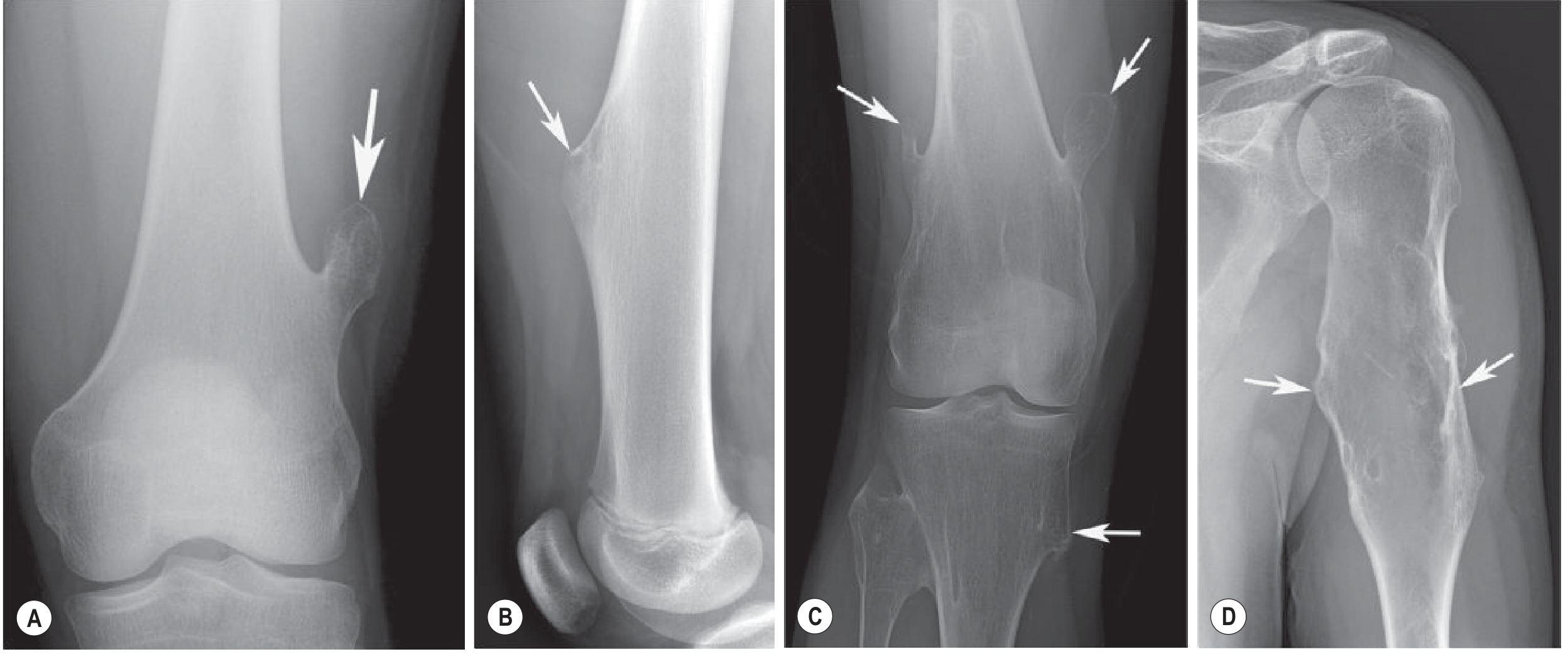
Fig. 40.7 - (C) Multiple osteochondromata in HME around the knee; (D) Irregular metadiaphyseal expansion of humerus in HME. (Grainger & Allison)
MRI / Ultrasound:
- Cartilage cap thickness: 1-3 cm in children, up to a few mm in adults - should not exceed 2 cm in adults
- A cap >2 cm raises concern for malignant transformation
- US shows the cap as hypoechoic against the brightly reflective bone surface
- MRI: cap best seen on T2-weighted or proton density FSE sequences (hyperintense cap vs. iso-/hypointense muscle)
Malignant Transformation
This is the most feared complication. Risk varies by context:
| Condition | Risk of Chondrosarcoma |
|---|---|
| Solitary osteochondroma | <1% |
| Diaphyseal aclasia / HME | 3%–5% (some sources quote up to 10%) |
| Ollier disease (enchondromatosis) | ~20–30% |
| Maffucci syndrome | ~30–100% |
-
Transformation almost always occurs in adults, not children
-
EXT1 mutation carries higher risk than EXT2
-
Warning signs: sudden pain in a previously asymptomatic lesion, or rapid enlargement
-
Any such lesion should be assessed by ultrasound (cap thickness) and MRI
-
Miller's Review of Orthopaedics p. 858; Grainger & Allison p. 1044; Rheumatology (Elsevier) p. 1959
Management
Conservative:
- Most lesions are asymptomatic and can be observed
- Growth of exostoses typically stops when the skeleton matures
Surgical indications:
- Mechanical symptoms (pain, joint restriction, nerve/vessel compression)
- Rapid growth or pain in adulthood (concern for malignant change)
- Cosmetic deformity
Surgical principles:
-
Surgical removal (excision at the base including periosteum and perichondrium)
-
If surgery is required in childhood, it should be deferred as late as possible to reduce the risk of regrowth while the skeleton is still growing
-
Malignant transformation is managed with wide surgical resection (chemotherapy has not been shown to improve survival for chondrosarcoma)
-
Rheumatology (Elsevier, 2022), p. 1959; Grainger & Allison, p. 1044
Associated Syndrome
When small chromosomal deletions on chromosome 8 encompass both the EXT1 locus and the nearby TRPS gene, the result is trichorhinophalangeal syndrome type 2 (Langer-Giedion syndrome) - combining epiphyseal dysplasia with exostoses. - Rheumatology (Elsevier, 2022)
Comparison with Related Conditions
| Feature | Diaphyseal Aclasia | Ollier Disease | Maffucci Syndrome |
|---|---|---|---|
| Lesion type | Osteochondromas (exostoses) | Enchondromas | Enchondromas + soft tissue angiomas |
| Inheritance | Autosomal dominant | Non-familial | Non-familial |
| Gene | EXT1 / EXT2 | IDH1/IDH2 (somatic) | IDH1/IDH2 (somatic) |
| Malignancy risk | 3-5% | 20-30% | 30-100% |
Recent Evidence
Two recent systematic reviews are relevant:
- A 2025 systematic review and meta-analysis (PMID 40266849) assessed the rate of spinal osteochondromas in pediatric patients with HME - noting spinal involvement as an under-recognized complication.
- A 2026 systematic review (PMID 42116060) on ulnar lengthening for forearm deformities in HME (2015-2025) found it an effective surgical option for forearm shortening and deformity, a common complication when exostoses affect the distal radius/ulna differentially.










+16 more
Explain line to line for examination of swelling
Here is a complete line-by-line explanation of all 10 pages from S Das - Chapter 3: Examination of a Lump or a Swelling.
EXAMINATION OF A LUMP OR A SWELLING
(S Das - A Manual on Clinical Surgery, Chapter 3)
DEFINITIONS (Page 1)
Lump - a vague mass of body tissue. Not every lump is a tumour.
Swelling - a vague term denoting any enlargement or protuberance in the body due to any cause. According to cause, a swelling may be:
- Congenital - present from birth (e.g. cystic hygroma, meningocele)
- Traumatic - from injury (e.g. haematoma)
- Inflammatory - due to infection or immune reaction
- Neoplastic - due to abnormal cell growth
- Miscellaneous - any other cause
Tumour / Neoplasm - a growth of new cells which proliferate independent of the body's needs.
- Benign tumour - proliferates slowly, little mitosis, not invasive to surrounding tissues
- Malignant tumour - proliferates fast, with invasiveness and mitosis (Fig. 3.1 shows sacrococcygeal teratoma - a tumour present since birth with a rudimentary hand developing from totipotent cells)
HISTORY (Pages 1-3)
History is recorded as per Chapter 1 with particular attention to these 15 points:
1. Duration
"How long is the lump present there?"
- Ask: "When was the lump first noticed?"
- Congenital swellings (cystic hygroma, meningocele) are present since birth
- Key distinction: "The lump was first noticed two months ago" vs "The lump first appeared two months ago" - the first is the patient's finding (they felt it later than it actually appeared); a painless lump may be present for a long time without the patient's knowledge
- Shorter duration + pain = mostly inflammatory (acute)
- Longer duration + no pain = possibly neoplastic (benign)
- Swellings with longer duration + slight pain = chronic inflammatory
- Shorter duration = may be neoplastic, mostly malignant
2. Mode of Onset
"How did the swelling start?"
- Appeared just after trauma = fracture displacement, dislocation, haematoma
- Appeared with severe pain = inflammation
- Noticed casually and gradually increasing in size = neoplasm (Fig. 3.2 & 3.3 - keloids on vaccination scar and ear pricks)
- From pre-existing condition = e.g. keloid from burn scar or pin prick; malignant melanoma develops from a benign naevus or a birth mark
- Neoplasms are mostly noticed casually: "I felt it during washing" or "Someone else noticed it first" - these painless swellings are more dangerous than painful ones and need careful examination
3. Other Symptoms Associated with the Lump
- Pain is the most important associated symptom
- Other symptoms: difficulty in respiration, difficulty in swallowing, interference with movement, disfigurement
- The patient will give the history of pain spontaneously but may NOT mention other symptoms - so ask specifically
4. Pain
Pain is an important and frequent complaint of traumatic and inflammatory swellings. Pain is conspicuously absent in neoplastic swellings, particularly in the early stage.
Ask precisely:
Nature of the pain:
- Throbbing = suggests inflammation leading to suppuration
- Burning / stabbing = sudden, sharp, severe, short duration
- Distending / aching = dull type
Site of pain:
- Pain may be referred to another site (e.g. hip joint disease → pain referred to the knee joint)
- Most often pain is localized to the site of the swelling
Time of onset:
- In inflammation - pain always appears before the swelling
- In tumours (both benign and malignant) - swelling appears long before the pain
Key rule: Most malignant tumours (stomach, kidney, rectum, breast) are painless to start with. Pain only appears due to nerve involvement, deep infiltration, ulceration, fungation, or associated inflammation - and often indicates inoperability. The exception is osteosarcoma, where mild pain is usually the first symptom and precedes the swelling. (Page 23)
5. Progress of the Swelling
"Has the lump changed its size since it was first noticed?"
- Benign growths - grow very slowly, may remain static for a long time
- Malignant tumours - grow very quickly
- Sudden increase in size after remaining stationary = malignant transformation of a benign growth
- Decrease in size = suggests inflammatory lesion
- Also ask about any change in surface or consistency
6. Exact Site
- Mostly obvious on inspection
- In case of a huge swelling, the patient may help by telling the exact site of origin
- The surgeon may be confused about which structure the swelling appeared from
7. Fever
- Enquire whether the patient had temperature along with the swelling
- Fever = suggests inflammatory swelling
- Examples: axillary abscess, gluteal abscess, ischiorectal abscess = fever
- Pyogenic lymphadenitis is often associated with fever
- Hodgkin's disease, renal carcinoma = associated with peculiar fever (Pel-Ebstein fever in Hodgkin's)
8. Presence of Other Lumps
"Whether the patient ever had or has any other lump?"
- Neurofibromatosis and diaphyseal aclasis will always have multiple swellings
- Hodgkin's disease generally shows multiple lymphoglandular enlargements
- Abscesses may occur one after the other
9. Secondary Changes
Some swellings present secondary changes such as:
- Softening
- Ulceration
- Fungation
- Inflammatory changes
- Ask specifically for these secondary changes
10. Impairment of Function
- Particularly of the limb or spine
- A swelling near a joint may cause partial or total loss of movement
- Osteosarcoma near the knee = partial or total loss of knee movement
- Cold abscess from caries spine = limitation of movement of the spine
11. Recurrence of the Swelling
- If a swelling recurs after removal = often indicates malignant change in a benign growth, or the primary was malignant
- Certain swellings are notoriously known to recur: e.g. Paget's recurrent fibroid
- Cystic swellings may recur if the cyst wall is not completely removed
12. Loss of Body Weight
- Appearance of swelling + loss of body weight = either a malignant growth or cold abscess with generalized tuberculosis
- Student's notes visible: 6 months → 10%; 3 months → 5%; 1 month → 5%
13. Past History
- May reveal presence of similar swelling or recurrence
- Past history of syphilis or tuberculosis may offer a clue to the present swelling
14. Personal History
- Habit of eating betel leaf, betel nut, slaked lime or tobacco = growth in the mouth, tongue, cheek or lip
- "Chutta Cancer" of hard palate = women who smoke cigars with burning ends in their mouths
- "Khaini Cancer" = lime and tobacco kept in the gingivolabial sulcus
15. Family History
- Many diseases have familial incidence
- Tuberculosis, Von Recklinghausen's disease, many malignant tumours often recur among family members
PHYSICAL EXAMINATION
A. GENERAL SURVEY (Page 4)
When a patient presents with a swelling, the patient should be looked at as a whole:
- Cachexia or malnutrition may be obvious at first look
- Attitude of the patient is very important:
- Abnormal attitude = osteosarcoma pressing on nerve → paresis or paralysis of distal limb; or displaced fracture/dislocation → limb assumes abnormal attitude
- Raised temperature and pulse rate = always associated with inflammatory swelling
B. LOCAL EXAMINATION
A. INSPECTION (Pages 4-6)
A good clinician always spends time in observation - students should not rush to touch the swelling immediately.
In inspection, note the following precisely:
1. Situation
- Some swellings are peculiar in their positions:
- Dermoid cysts - mostly seen in the midline or on the line of fusion of embryonic processes
- Outer canthus of the eye = line of fusion between fronto-nasal process and maxillary process (Fig. 3.8)
- Behind the ear = post-auricular dermoid (Fig. 3.9) - on the line of fusion of mesodermal hillocks forming the pinna
- Dermoid cysts - mostly seen in the midline or on the line of fusion of embryonic processes
- Note the extent of the swelling in vertical and horizontal directions on the case note
2. Colour
- Colour gives a definite hint to diagnosis:
- Black colour = benign naevus and melanoma
- Red or purple = haemangioma (Fig. 3.53) - arterial or venous haemangioma
- Bluish colour = ranula - obvious and diagnostic
3. Shape
- Note whether it is: ovoid, pear-shaped, kidney-shaped, spherical, or irregular
- Do not say "circular" - we don't know the deeper dimension, so say "spherical"
4. Size
- Note the vertical and horizontal dimensions
- On inspection, the deeper dimension is missed - palpation gives this
- Mention clearly in cm on the history sheet, with a sketch showing position
5. Surface
- May be difficult on inspection alone, but some are diagnostic:
- Cauliflower surface = squamous cell carcinoma (Fig. 3.11)
- Irregular branched surface = papilloma (Fig. 3.10)
6. Edge
- Edge may be clearly defined or indistinct
- Swelling may be pedunculated or sessile
7. Number
- Some swellings are always multiple:
- Diaphyseal aclasis, neurofibromatosis, multiple glandular swellings
- Some are typically solitary:
- Lipoma, dermoid cyst, etc.
8. Pulsation
- Swellings arising from arteries = pulsatile (e.g. aneurysms and carotid body tumour)
- Swellings just superficial to the artery in close relation = transmitted pulsation
- Swellings originating from arterial walls = expansile pulsation
9. Peristalsis
- Certain swellings are associated with visible peristalsis:
- Congenital hypertrophic pyloric stenosis
- Swellings causing intestinal obstruction
10. Movement with Respiration
- Swellings arising from upper abdominal viscera (liver, spleen, stomach, gallbladder, hepatic and splenic flexures of the transverse colon) move with respiration
- Not seen in hard swellings (student's note)
11. Impulse on Coughing
- Swellings in continuity with the abdominal cavity, pleural cavity, spinal canal or cranial cavity will give rise to impulse on coughing
- Ask the patient to cough and the swelling will give an impulse while coughing
- In children - crying works as coughing (Fig. 3.20 & 3.21)
12. Movement on Deglutition
- Swellings fixed to the larynx or trachea move during swallowing:
- Thyroid swellings
- Thyroglossal cysts
- Subhyoid bursitis
- Pre- or paratracheal lymph node enlargement
13. Movement with Protrusion of the Tongue
- A thyroglossal cyst moves up along with protrusion of the tongue - showing its intimate relation with the thyroglossal tract
14. Skin Over the Swelling
- Red and oedematous = inflammatory swelling
- Tense, glossy with venous prominence = sarcoma with rapid growth (Fig. 3.12)
- Black punctum over a cutaneous swelling = sebaceous cyst
- Pigmentation = moles, naevi, or after repeated deep X-rays
- Linear scar with suture marks = previous operation
- Puckered, broad, irregular scar = previous suppuration
- Peau d'orange (skin looks like peel of an orange) = oedematous swelling from blockage of small lymphatics → most peculiarly seen in breast carcinoma (Fig. 30.9)
- Presence of ulcer on skin = discussed in the next chapter
15. Any Pressure Effect
- Always examine the limb distal to the swelling
- Axillary swelling + oedema of upper limb = swelling probably arising from the lymph nodes
- Wasting of the distal limb = traumatic swelling, or injury to the nerves
- Swelling in the neck with venous engorgement = immediately gives suspicion of retrosternal prolongation → venous obstruction
B. PALPATION (Pages 7-10)
Palpation is the most important part of local examination. It not only corroborates inspection findings but gives new, definitive diagnostic clues. Be methodical and follow a definite order so no important examination is missed. Be very gentle - a few swellings may be malignant and may spread due to reckless handling.
1. Temperature
- Local temperature is raised due to:
- Excessive vascularity of the swelling
- Infection
- Well-vascularized tumour (e.g. sarcoma)
- Must be examined FIRST in palpation - as manipulation during subsequent examinations may increase temperature without any definite reason
- Temperature is best felt by the back of the fingers (Fig. 3.13) - the back is more sensitive than the palmar surface
2. Tenderness
- Tenderness = pain on pressure exerted by the clinician
- To elicit: be very gentle; watch the patient's facial expression while palpating
- Inflammatory swellings = mostly tender
- Neoplastic swellings = NOT tender
3. Size, Shape and Extent
- Palpation gives the deeper dimension (missed on inspection)
- Clarifies the vertical and horizontal dimensions better
- Mention in cm, sketched on the history sheet clearly indicating the position
- Find out the whole extent - if a portion disappears behind a bone, clearly mention this
4. Surface
- Palpate with palmar surfaces of fingers to its entirety
- Surface may be:
- Smooth = cyst
- Lobular with smooth bumps = lipoma
- Nodular = mass of matted lymph nodes
- Irregular and rough = carcinoma
5. Edge
- Palpated by tips of the fingers
- Well-defined margins tend to slip away from the finger
- Neoplastic and chronic inflammatory swellings = well-defined margins
- Benign growths = smooth margins; Malignant growths = irregular margins
- Acute inflammatory swellings = ill-defined or indistinct margins
Slip sign (Fig. 3.14 & 3.15): The margin of a solid swelling (e.g. lipoma) slips away from the palpating finger but does NOT yield to it. The margin of a cystic swelling yields to the palpating finger and cannot slip away. This differentiates benign tumour like lipoma (slips away, does not yield) from a cyst (yields and does not slip away).
6. Consistency
- The consistency depends on what the swelling is made of
- Types:
- Soft = lipoma
- Cystic = cysts, chronic abscesses
- Firm = fibroma
- Hard but yielding = chondroma
- Bony hard = osteoma
- Stony hard = carcinoma
- All except cystic are solid
- A solid swelling may also be soft (e.g. lipoma)
- Gaseous swellings (gas gangrene, surgical emphysema) = crepitus may be heard
- Variable consistency = often indicates malignancy (carcinoma or sarcoma)
- Moulding on pressure = pultaceous/putty-like material → sebaceous cyst, dermoid cyst, or abdominal colonic swelling containing faecal mass
- Pitting on pressure = oedematous tissue = inflammatory swelling
7. Fluctuation (Fig. 3.16, 3.18)
-
A swelling fluctuates when it contains liquid or gas
-
Technique: One finger of each hand is used. Sudden pressure on one pole → pressure transmitted equally at right angles to all parts of wall → the finger on the opposite pole is raised passively = fluctuation positive
-
Rules:
- Test must be performed in two planes at right angles to each other (a fleshy muscle like quadriceps femoris may show fluctuation at right angle to fibres but not along the line → false positive)
- Two fingers should be kept as far apart as the size of swelling allows
- If swelling is freely movable - fix it with thumb and forefinger of one hand, compress the other pole with thumb and fingers of the other hand
- For very small swellings that cannot accommodate two fingers = simply press at its centre (the fluid-containing swelling will be softer at the centre; a solid swelling will be firmer at the centre)
-
Paget's test: Another method - two fingers of left hand on swelling (watching fingers); right index finger (displacing finger) presses on the swelling to displace fluid inside, felt by watching fingers. Must be done in two planes at right angles.
-
For large swellings: tapping one side with two fingers while the percussion wave is felt on the other side = fluid thrill.
-
Important warning: Soft swellings sometimes yield false positive fluctuation test (lipoma, myxoma, soft fibroma, vascular sarcoma) - they yield to pressure but fail to expand in other parts of the swelling like a true fluctuant swelling.
8. Fluid Thrill
- In large swellings containing fluid - a percussion wave is conducted to the other pole when one pole is tapped (as in percussion)
- Large swelling: tap one side with two fingers → feel the wave on other side with palmar aspect of the hand
- Small swelling: three fingers placed on the swelling, middle finger tapped → wave felt by the two fingers on each side
This covers all 10 pages completely. The chapter follows a systematic order: History (15 points) → General Survey → Inspection (15 points) → Palpation (8+ points), with the remaining palpation points (translucency, reducibility, compressibility, mobility, relations to deeper and superficial structures, regional lymph nodes, and special tests) continuing in subsequent pages.










+16 more
Explain line to line
!
An error occurred (ValidationException) when calling the ConverseStream operation: The model returned the following errors: messages.1.content.33.image.source.base64.data: At least one of the image dimensions exceed max allowed size for many-image requests: 2000 pixels
We encountered an error while processing your request. Please try again or reach out to us for help.
This is a shared conversation. Sign in to Orris to start your own chat.