explain in detail about the pareital lobe use guyton and hall and ganong etc. books as your source
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have rich content from all the key sources. Let me compile the comprehensive answer.
The Parietal Lobe - A Comprehensive Review
Sources: Guyton & Hall Textbook of Medical Physiology, Ganong's Review of Medical Physiology (26th ed.), Adams & Victor's Principles of Neurology (12th ed.), Neuroscience: Exploring the Brain (5th ed.), Neuroanatomy Through Clinical Cases (3rd ed.)
1. Anatomy and Boundaries
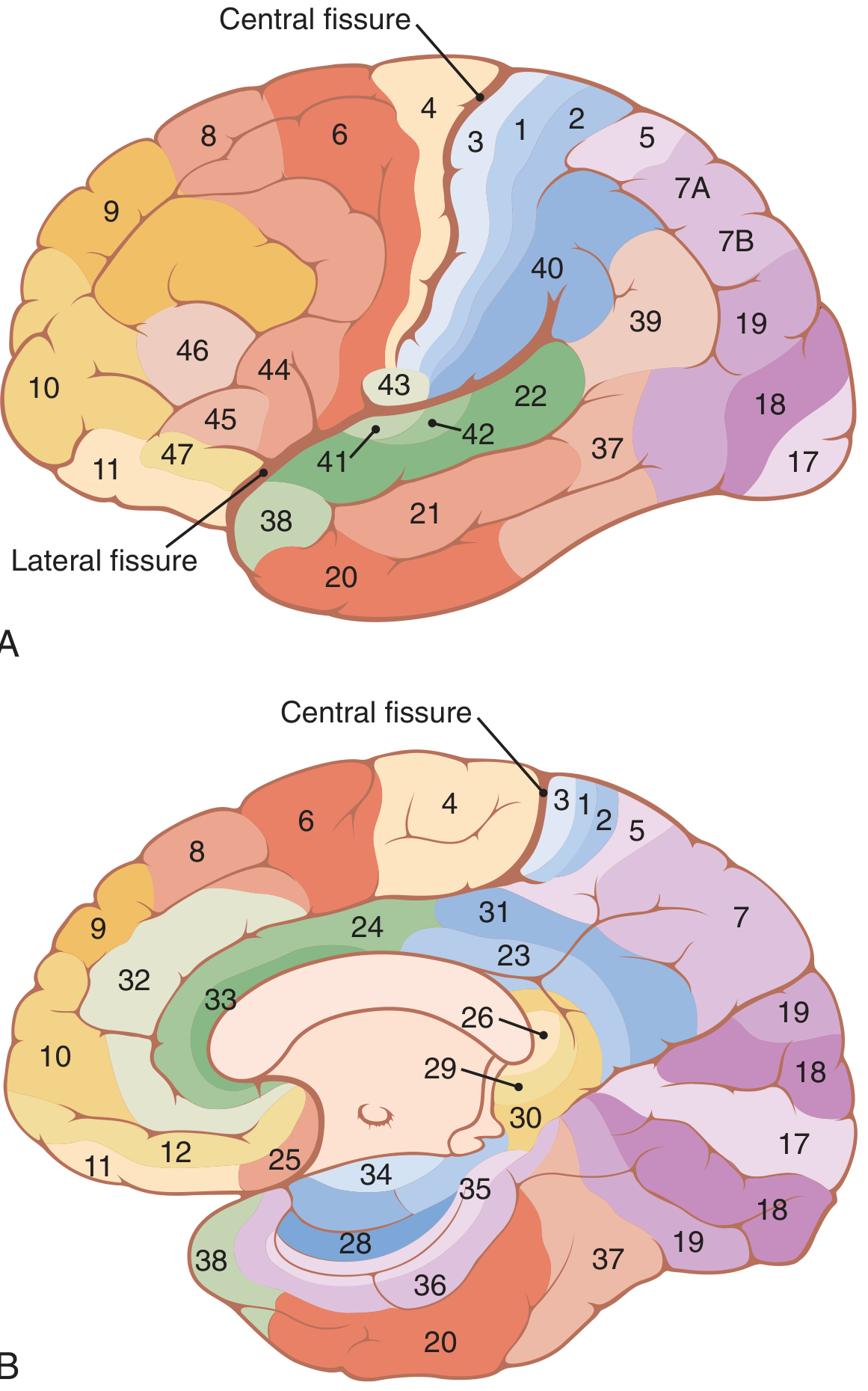
The parietal lobe sits between the frontal lobe anteriorly (separated by the central sulcus/fissure), the occipital lobe posteriorly (separated by the parietooccipital fissure), and the temporal lobe inferiorly (separated by the lateral/Sylvian fissure). It contains several key gyri and sulci:
- Postcentral gyrus - immediately posterior to the central sulcus; contains primary somatosensory cortex (S1)
- Superior parietal lobule - Brodmann areas 5 and 7
- Inferior parietal lobule - contains the supramarginal gyrus (BA 40) and the angular gyrus (BA 39)
- Intraparietal sulcus - divides the superior and inferior parietal lobules
2. The Somatosensory Cortex (Primary Sensory Area - S1)
Guyton & Hall
"Generally, the anterior half of the parietal lobe is concerned almost entirely with reception and interpretation of somatosensory signals, but the posterior half of the parietal lobe provides still higher levels of interpretation." - Guyton & Hall, p. 599
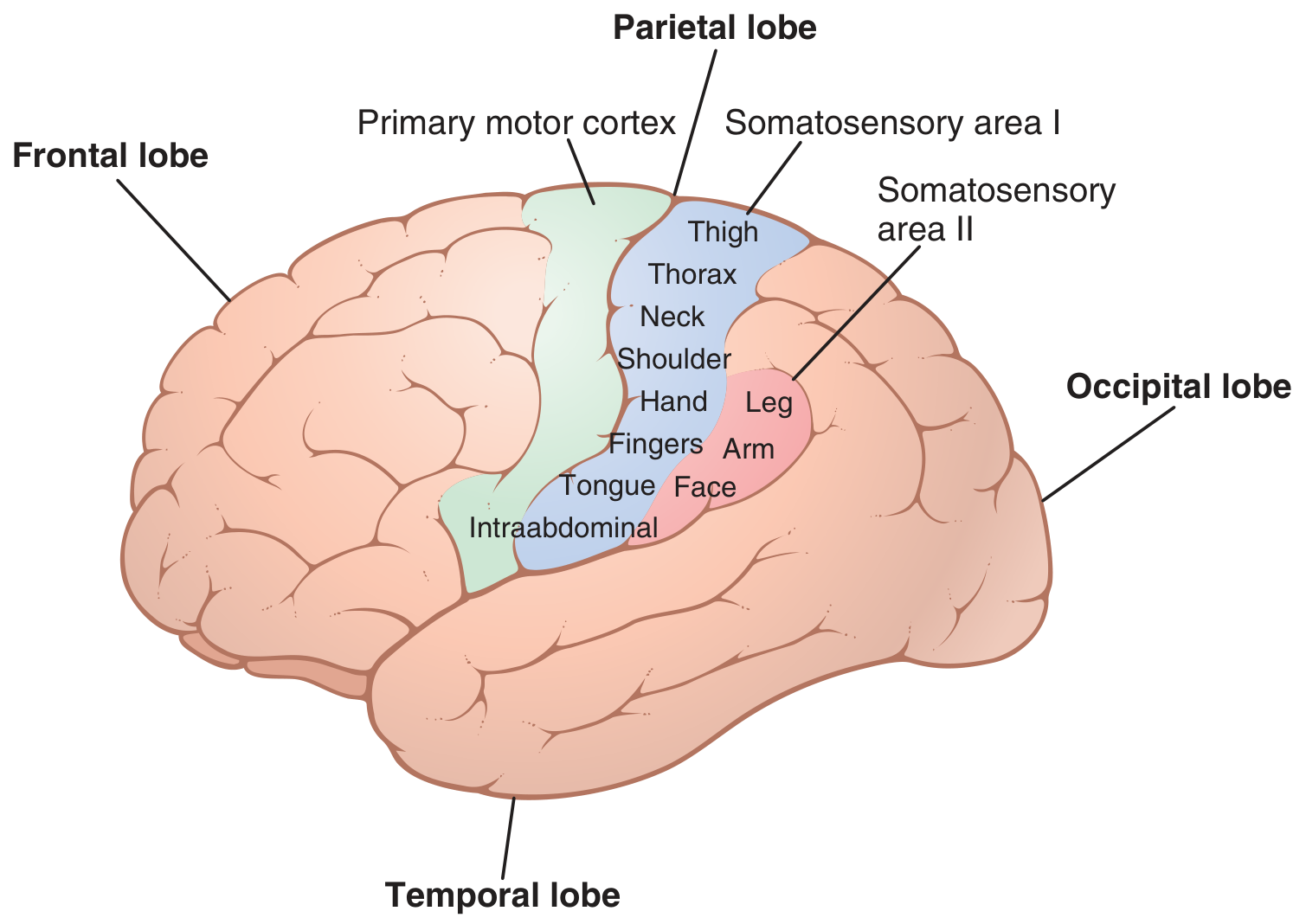
The somatosensory cortex lies in the postcentral gyrus (Brodmann areas 3, 1, and 2). It has two distinct divisions:
Somatosensory Area I (S1) - Brodmann Areas 3, 1, 2
This is the dominant primary sensory area. It has high topographic localization of the body - the classic sensory homunculus (Penfield's map). Key points from Guyton:
- Face and lips have the largest representation (proportional to the density of specialized receptors)
- Lips have the greatest representation of all, followed by the face and thumb
- The trunk and lower body are represented by relatively small areas
- Each lateral cortex receives sensory input almost exclusively from the opposite side of the body
- The nose, lips, mouth, and face are represented in the most lateral portion; the head, neck, and lower body are represented medially
Somatosensory Area II (S2)
- Located in the parietal cortex just posterior and inferior to S1, deep in the Sylvian fissure
- Has a rough spatial organization (face anteriorly, arms centrally, legs posteriorly) but with poor localization
- Receives signals from the brain stem from both sides of the body
- Receives secondary input from S1, the visual cortex, and auditory cortex
- S1 input is required for S2 function, but removal of S2 does not affect S1 neurons
3. Cortical Layers and Columnar Organization
The parietal cortex, like all neocortex, has 6 layers:
- Layer I (molecular) - sparse neurons, mainly dendrites and axons
- Layer II - external granular layer
- Layer III - layer of small pyramidal cells
- Layer IV - internal granular layer; receives the main thalamic sensory input
- Layer V - large pyramidal cells projecting to the basal ganglia, brainstem, and spinal cord
- Layer VI - projects back to the thalamus, modulating incoming sensory signals
The neurons are organized in vertical columns (0.3-0.5 mm diameter, ~10,000 neurons each). Each column serves a single specific sensory modality. In the anterior postcentral gyrus (area 3a), columns respond to muscle/tendon/joint stretch receptors. Moving posteriorly, columns respond to slowly adapting cutaneous receptors, then deep pressure, and in the most posterior portion, some columns respond only to directional skin movement. - Guyton & Hall, p. 601
4. Somatosensory Association Area (Posterior Parietal Cortex)
Guyton & Hall
Brodmann areas 5 and 7 lie behind S1 and constitute the somatosensory association area. They "play important roles in deciphering deeper meanings of the sensory information." Inputs to this area come from:
- Somatosensory area I
- Ventrobasal nuclei of the thalamus
- Other thalamic areas
- The visual cortex
- The auditory cortex
Electrical stimulation here can cause an awake person to experience complex body sensations - even feeling a specific object like a knife or ball.
Amorphosynthesis: When this area is removed on one side, the person:
- Loses ability to recognize complex objects felt on the opposite side
- Loses the sense of form of their own body parts on the opposite side
- Becomes mainly oblivious to the opposite side of the body
- Tends to recognize only one side of a felt object, forgetting the other side exists - Guyton & Hall, p. 602
Ganong's Review
The posterior parietal cortex receives projections from the somatic sensory area. "Some of the neurons are concerned with aiming the hands toward an object and manipulating it, whereas other neurons are concerned with hand-eye coordination." Lesions cause "defects in motor performance that are characterized by inability to execute learned sequences of movements such as eating with a knife and fork." The posterior parietal cortex contributes to descending motor control pathways. - Ganong, p. 244-245
Neuroscience: Exploring the Brain (5th ed.)
"The posterior parietal cortex... is concerned not only with somatic sensation but also with vision, audition, movement planning, spatial navigation, memory, and even decision-making and a person's state of attentiveness." Neurons here have very large receptive fields with highly complex stimulus preferences. This is a convergence zone where simple, segregated sensory streams combine to generate complex neural representations.
5. The Angular Gyrus and the Supramarginal Gyrus
Guyton & Hall
The angular gyrus is the most inferior portion of the posterior parietal lobe, lying immediately behind the Wernicke area (temporal lobe) and fusing into the visual areas of the occipital lobe. If it is destroyed:
- The person can still interpret auditory experiences normally (Wernicke intact)
- But visual information cannot be integrated into language understanding
- The person can see words but cannot understand their meaning
- This condition is called alexia (word blindness)
The angular gyrus thus serves as a critical relay for converting visual language input into meaningful symbols. - Guyton & Hall, p. 719
In the dominant (left) hemisphere, the angular gyrus and supramarginal gyrus also integrate:
- Reading and writing
- Arithmetic and calculation
- Spatial reasoning with numbers
6. Visual and Spatial Processing
The parietal lobe forms the "where" (dorsal) visual stream, receiving input from the visual cortex. Guyton notes that "signals representing form, 3D position, and motion are transmitted mainly into the superior portions of the occipital lobe and posterior portions of the parietal lobe," while detailed visual and color signals go to the temporal (ventral) stream.
The posterior parietal cortex (especially BA 7) is part of the "salience and priority map" - it determines where to direct attention in space (Neuroscience: Exploring the Brain).
The equilibrium/vestibular primary cortical center is also located "in the parietal lobe deep in the sylvian fissure" on the opposite side from the stimulated vestibular apparatus. - Guyton & Hall, p. 642
7. Clinical Effects of Parietal Lobe Lesions
Adams & Victor's Principles of Neurology (12th ed.)
Adams & Victor provide the most detailed clinical synthesis. They note that historically the parietal lobe was considered a "silent area" by Oppenheim and Gowers, but is now recognized as producing "the richest variety of clinical phenomena of any territory within the brain."
The core deficit of parietal lobe disease centers on agnosia - loss of recognition that cannot be attributed to a defect in the primary sensory modality itself.
I. Effects of Unilateral Parietal Lobe Disease (Either Side)
| Feature | Description |
|---|---|
| Corticosensory syndrome | Loss of discriminative sensation - astereognosis, agraphesthesia, loss of two-point discrimination, impaired directional tactile sense |
| Mild hemiparesis | Poverty of movement, occasional hemiataxia |
| Visual field defect | Homonymous hemianopia or inferior quadrantanopia; visual inattention |
| Optokinetic nystagmus | Abolished when target moves toward side of the lesion |
| Contralateral neglect | More prominent with right parietal lesions |
II. Effects of Dominant (Left) Parietal Lobe Disease
A. Disorders of language, especially alexia
B. Gerstmann syndrome - the classic tetrad:
- Dysgraphia (impaired writing)
- Dyscalculia (impaired arithmetic)
- Finger agnosia (inability to identify individual fingers)
- Right-left disorientation C. Tactile agnosia (bimanual astereognosis) - cannot identify objects by touch D. Bilateral ideomotor and ideational apraxia - inability to carry out commanded motor acts despite intact motor and sensory function E. Understanding of spoken and written words is partly mediated by the supramarginal and angular gyri of the dominant parietal lobe
III. Effects of Nondominant (Right) Parietal Lobe Disease
A. Visuospatial disorders - inability to orient oneself in space, draw floor plans, navigate familiar routes
B. Topographic memory loss - inability to describe routes, find one's way
C. Anosognosia - unawareness of one's own neurological deficit
D. Dressing apraxia - inability to dress oneself
E. Constructional apraxia - inability to copy or construct geometric figures
F. Confusion and altered attention
G. Tendency to keep the eyes closed and resist lid opening; blepharospasm
H. Hemineglect - the most prominent right parietal syndrome; patient ignores the entire left side of the world and body
Clinical illustration (Adams & Victor): A patient with a right parietal lesion, when asked to describe the buildings around the Piazza del Duomo from memory, consistently omitted all buildings on the left side of the piazza - regardless of which corner of the piazza they imagined themselves standing in. This demonstrated that neglect extends to the mental representation of space itself (Bisiach & Luzzatti experiment).
IV. Effects of Bilateral Parietal Lobe Disease
Balint Syndrome (three components):
- Simultanagnosia (visual-spatial imperception) - inability to perceive more than one object at a time despite intact visual acuity
- Optic apraxia - difficulty directing gaze toward objects
- Optic ataxia - difficulty reaching for objects under visual guidance
8. Sensory Loss Caused by Parietal Lobe Lesions (Adams & Victor)
The key distinction is that parietal cortical lesions produce discriminative sensory loss rather than complete loss of primary sensation:
- Astereognosis - inability to distinguish shape, size, weight, texture
- Agraphesthesia - inability to recognize figures written on skin
- Impaired two-point discrimination
- Impaired detection of tactile stimulus direction
Primary pain, temperature, touch, pressure, and vibration are relatively preserved if the postcentral gyrus itself is spared. It is only when the lesion involves the postcentral gyrus directly that primary somatosensory deficits occur. The Dejerine-Mouzon syndrome presents with severe impairment of all modalities from parietal lesions.
9. Motor Functions of the Parietal Lobe
The parietal lobe has important roles in motor control beyond purely sensory processing:
- Large parietal lobe lesions produce ideomotor apraxia - the conceptual patterns for complex voluntary acts depend on the integrity of the dominant parietal lobe (Adams & Victor)
- The postcentral gyrus sends signals directly to the motor cortex to guide motor activity based on sensory feedback - especially from muscle/tendon/joint stretch receptors in area 3a (Guyton)
- The posterior parietal cortex projects to the premotor cortex and contributes to descending motor pathways (Ganong)
- Lesions cause mild contralateral hemiparesis or poverty of movement (Adams & Victor)
10. The Parietal Lobe and Neglect Syndrome
The neglect syndrome is the most striking nondominant parietal manifestation (Neuroscience: Exploring the Brain, 5th ed.):
- Occurs most commonly with right hemisphere (nondominant) damage
- Patient ignores or suppresses entire contralateral hemispace
- May deny that the contralateral limb is their own (as Oliver Sacks described in "The Man Who Fell Out of Bed")
- Patients may ignore food on one half of the plate, or dress only one side of their body
- Usually improves or disappears with time
From Neuroanatomy Through Clinical Cases: Parietal lobe seizures produce vertigo, contralateral numbness, tingling, burning, sensation of movement, and in the dominant hemisphere, aphasia; in the nondominant hemisphere, contralateral hemineglect.
11. Summary: Functions of the Parietal Lobe by Region
| Region | Brodmann Areas | Main Functions |
|---|---|---|
| Postcentral gyrus (S1) | 3a, 3b, 1, 2 | Primary somatosensory cortex; tactile discrimination, proprioception, topographic body map |
| Somatosensory area II (S2) | Deep in Sylvian fissure | Bilateral somatic input; role in tactile learning and memory |
| Superior parietal lobule | 5, 7 | Somatosensory association; limb/body spatial position; hand-eye coordination; reaching |
| Supramarginal gyrus | 40 | Language (dominant: phonological processing); ideomotor praxis |
| Angular gyrus | 39 | Language (dominant: visual-verbal integration, reading); visuospatial processing |
| Posterior parietal cortex (bilateral) | 5, 7, 39, 40 | Spatial attention, neglect, body schema, multimodal integration |
Key Takeaways
- The parietal lobe is divided functionally into the anterior half (primary and secondary somatosensory cortex) and the posterior half (higher-order association areas).
- It is the hub of somatosensory discrimination, spatial awareness, body schema, and visuomotor integration.
- Dominant (left) parietal lesions produce Gerstmann syndrome, apraxia, alexia, and language dysfunction.
- Nondominant (right) parietal lesions produce contralateral neglect, anosognosia, constructional/dressing apraxia, and visuospatial deficits.
- Bilateral lesions produce Balint syndrome.
- The parietal lobe is not "silent" - it is one of the most functionally rich regions of the cerebral cortex, acting as a high-order sensory integration organ with direct implications for motor control, language, spatial orientation, and self-awareness.
References:
- Guyton and Hall Textbook of Medical Physiology (Chapters 48, 57, 58) - p. 599-602, 719-720
- Ganong's Review of Medical Physiology, 26th Edition - p. 244-245
- Adams and Victor's Principles of Neurology, 12th Edition - Chapter 21, pp. 485-497
- Neuroscience: Exploring the Brain, 5th Edition - pp. 1188-1190
- Neuroanatomy Through Clinical Cases, 3rd Edition - p. 880, 1007
This is a shared conversation. Sign in to Orris to start your own chat.