Epilepsy seizures
Reading File
Finding Sources
Searching PubMed
"epilepsy" AND "seizure classification"
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
I now have thorough content to write a comprehensive answer. Let me compile it.
Epilepsy and Seizures
Definition
Epilepsy is a condition of recurrent, unprovoked seizures. A seizure is any paroxysmal, abnormal electrical discharge from cerebral neurons that may produce loss of consciousness, altered perception, convulsive movements, sensory disturbances, or some combination of these. As Hughlings Jackson (1870) described it: "an excessive and disorderly discharge of cerebral nervous tissue on muscles."
- Seizure is the preferred generic term - it covers all paroxysmal electrical discharges, including non-convulsive forms.
- Convulsion refers specifically to paroxysmal involuntary muscular contractions - a subset of seizures.
- Epilepsy = at least two unprovoked seizures.
Epidemiology
- ~2 million people in the United States have epilepsy
- Incidence: ~44 new cases per 100,000 persons/year
- Nearly 1% of the US population will have epilepsy by age 20
- Over two-thirds of all epileptic seizures begin in childhood (highest in the first year of life)
- Incidence rises again after age 60, often due to cerebrovascular disease and neurodegeneration
- Adams and Victor's Principles of Neurology, 12th Edition
ILAE Classification of Seizure Types (2017)
The International League Against Epilepsy (ILAE) 2017 classification divides seizures into:
1. Focal Onset Seizures (formerly "Partial")
Originate in one hemisphere or network.
| Old Term | New Term |
|---|---|
| Simple partial seizure | Focal aware seizure |
| Complex partial seizure | Focal impaired awareness seizure |
| Partial seizure with secondary generalization | Focal-to-bilateral tonic-clonic seizure |
2. Generalized Onset Seizures
Involve both hemispheres from the start.
| Type | Notes |
|---|---|
| Generalized tonic-clonic (grand mal) | Most dramatic; loss of consciousness + convulsions |
| Absence seizure (petit mal) | Brief staring spells; typical in childhood absence epilepsy |
| Myoclonic seizure | Sudden brief muscle jerks; seen in juvenile myoclonic epilepsy, Dravet syndrome |
| Atonic seizure (drop seizure) | Sudden loss of muscle tone; seen in Lennox-Gastaut syndrome |
| Epileptic spasms | Infantile spasms (West syndrome) |
3. Unknown Onset
- Katzung's Basic and Clinical Pharmacology, 16th Edition; Adams and Victor's Principles of Neurology, 12th Edition
Seizure Types by Age
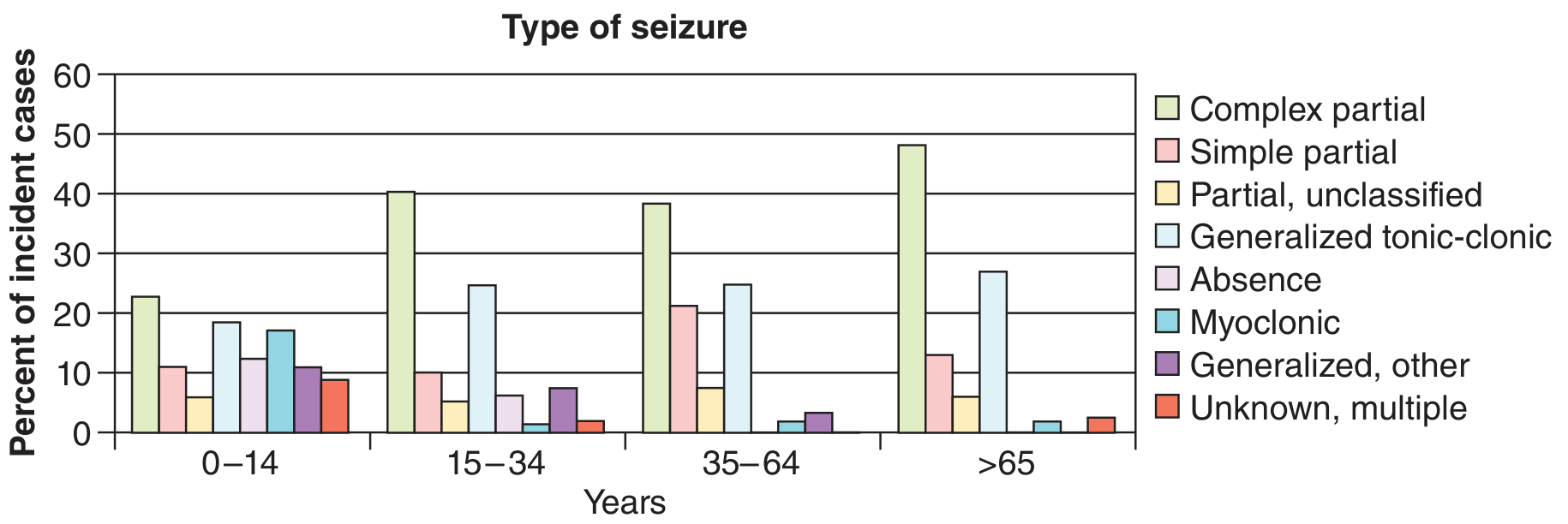
Figure: Seizure type distribution by age. Complex partial (focal impaired awareness) seizures predominate after age 15 and are especially common in adults >65. Absence and myoclonic seizures peak in childhood. - Adams and Victor's Principles of Neurology, 12th Edition
Pathophysiology
Etiology falls into two broad categories:
- Idiopathic/Genetic - no structural lesion; typically due to ion channel mutations (e.g., sodium, potassium, chloride channels, or GABA receptor subunits). Most childhood epilepsies fall here.
- Structural/Acquired - caused by:
- Cortical scars (trauma, prior stroke, infection)
- Hippocampal sclerosis
- Cortical dysplasia or malformations
- Tumors, vascular lesions
- Metabolic disorders
The final common pathway is an imbalance favoring excitation over inhibition: increased glutamate-mediated depolarization or decreased GABA-mediated inhibition leads to hypersynchronous neuronal firing.
Clinical Features of a Generalized Tonic-Clonic Seizure
A typical grand mal seizure progresses through distinct phases:
- Prodrome (hours before): mood changes, irritability, or myoclonic jerks on awakening
- Tonic phase (~10-20 sec):
- Sudden loss of consciousness, fall
- Brief flexion of trunk, then sustained rigid extension of neck, back, limbs
- Piercing cry as air is forced through closed vocal cords
- Apnea - skin may become cyanotic
- Pupils dilated and unreactive
- Clonic phase (~30 sec):
- Rhythmic flexor spasms begin at ~8/sec, slow to ~4/sec
- Violent, repetitive whole-body jerking
- Autonomic: rapid pulse, elevated BP, salivation, sweating
- Tongue may be bitten
- Postictal phase (minutes to hours):
- Deep coma, limp, stertorous breathing
- Gradual awakening with confusion, agitation, amnesia for the event
- Headache, muscle soreness, fatigue
- Adams and Victor's Principles of Neurology, 12th Edition
Absence Seizures
- Brief (5-20 sec) episodes of staring and unresponsiveness
- Abrupt onset and offset, no postictal confusion
- EEG shows classic 3 Hz spike-and-wave
- Typical in childhood (ages 4-12); may resolve in adolescence
- Treatment: ethosuximide, valproate, or lamotrigine
Focal Seizures
Focal aware (old: simple partial): consciousness preserved; symptoms depend on origin - motor (Jacksonian march), sensory, autonomic, or psychic (deja vu, fear, rising epigastric sensation)
Focal impaired awareness (old: complex partial): consciousness impaired; often temporal lobe origin; automatisms (lip smacking, hand movements), post-ictal confusion common
Focal-to-bilateral tonic-clonic: starts focal, generalizes - implies a focal structural lesion
Epilepsy Syndromes
| Syndrome | Age Onset | Key Features |
|---|---|---|
| West syndrome | Infancy (3-12 mo) | Infantile spasms, hypsarrhythmia on EEG, developmental regression |
| Dravet syndrome | Infancy | Febrile + afebrile seizures, SCN1A mutation, drug-resistant |
| Childhood absence epilepsy | 4-12 years | Typical absence seizures, 3 Hz spike-wave |
| Benign epilepsy with centrotemporal spikes (BECTS) | 3-13 years | Nocturnal focal motor seizures, self-limiting |
| Juvenile myoclonic epilepsy (JME) | Adolescence | Morning myoclonus, GTC seizures, absence; lifelong but responsive to valproate |
| Lennox-Gastaut syndrome | Childhood | Multiple seizure types, drug-resistant, intellectual disability |
| Temporal lobe epilepsy (mesial) | Any age | Focal impaired awareness seizures; hippocampal sclerosis on MRI; surgically remediable |
Diagnosis
- EEG: cornerstone; inter-ictal spikes, generalized spike-wave, focal slowing
- MRI brain: structural lesions, hippocampal sclerosis, cortical dysplasia
- Blood tests: glucose, electrolytes, calcium (rule out metabolic causes)
- Genetic testing: for suspected genetic epilepsies (sodium/potassium channel mutations, copy number variants)
Treatment
Antiseizure Medications (ASMs)
Choice depends on seizure type and syndrome:
| Seizure Type | First-Line Drugs |
|---|---|
| Generalized tonic-clonic | Valproate, levetiracetam, lamotrigine |
| Absence | Ethosuximide, valproate, lamotrigine |
| Focal (any) | Carbamazepine, oxcarbazepine, levetiracetam, lamotrigine, lacosamide |
| Juvenile myoclonic epilepsy | Valproate, levetiracetam |
| Lennox-Gastaut | Valproate, clobazam, lamotrigine, rufinamide |
- Monotherapy preferred; ~two-thirds of patients achieve seizure control
- Patients failing two appropriate medications are considered pharmacoresistant
Non-pharmacological Options
- Epilepsy surgery: Temporal lobe resection is the most common procedure; curative in mesial temporal lobe epilepsy
- Vagus nerve stimulator (VNS): Implanted device, open-loop stimulation - for drug-refractory focal seizures
- Responsive neurostimulator (RNS): Closed-loop, detects abnormal EEG and delivers stimulation to the seizure focus
- Deep brain stimulation (DBS): Bilateral stimulation of anterior thalamic nuclei for focal epilepsy
- Ketogenic diet: High-fat, low-carbohydrate diet; particularly useful in refractory pediatric epilepsy and specific metabolic epilepsies
- Katzung's Basic and Clinical Pharmacology, 16th Edition
Status Epilepticus
Status epilepticus (SE) is a neurological emergency - either a seizure lasting >5 minutes (GTC) or repeated seizures without recovery of consciousness.
Types:
- Generalized convulsive SE - bilateral limb jerking + impaired consciousness; life-threatening
- Nonconvulsive SE - behavioral change + continuous EEG epileptiform activity without major motor signs; includes absence SE and focal SE
Treatment algorithm:
| Stage | Intervention |
|---|---|
| First-line | IV lorazepam or IM midazolam (benzodiazepine) |
| Second-line | IV levetiracetam, valproate, fosphenytoin, or phenytoin (equally effective after benzo failure; ~50% response each) |
| Refractory SE (seizure continues ≥30 min after 1st + 2nd line) | Anesthetic doses of pentobarbital, propofol, or midazolam infusion |
- Rectal diazepam, intranasal midazolam, or buccal midazolam are acceptable prehospital alternatives
- Convulsive SE may evolve to nonconvulsive SE after treatment - EEG monitoring is essential
- Absence SE: benzodiazepine + IV valproate
- Katzung's Basic and Clinical Pharmacology, 16th Edition
Key Takeaways
- Epilepsy = recurrent unprovoked seizures; seizure = paroxysmal abnormal brain discharge
- ILAE 2017: focal onset / generalized onset / unknown onset
- Grand mal (GTC) = tonic phase → clonic phase → postictal phase
- Two-thirds of patients respond to first or second medication; one-third are pharmacoresistant
- Drug-refractory epilepsy: consider surgery, VNS, RNS, DBS, or ketogenic diet
- Status epilepticus: treat at 5 minutes with benzodiazepines, escalate rapidly
Epilepsy seizures
Reading File
Epilepsy seizures definition epidemiology pathophysiology investigation treatment prevention give me all details and search in all medical book and give me 50 slide power point
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Running Command
mkdir -p /home/daytona/workspace/epilepsy-pptx && ls /home/daytona/workspace/epilepsy-pptx
Writing File
~/epilepsy-pptx/build.js
const pptxgen = require("pptxgenjs");
const pres = new pptxgen();
pres.layout = "LAYOUT_16x9";
pres.author = "Medical Education";
pres.title = "Epilepsy & Seizures – Comprehensive Review";
// ── COLOUR PALETTE ──────────────────────────────────────────────
const DARK_BG = "0D1B2A"; // deep navy (title / section slides)
const MID_BG = "1B2A3B"; // slightly lighter navy
const CARD_BG = "162032"; // card backgrounds
const ACCENT1 = "4FC3F7"; // sky-blue accent
const ACCENT2 = "81C784"; // green accent
const ACCENT3 = "FFB74D"; // amber accent
const ACCENT_R = "EF5350"; // red accent (emergency)
const WHITE = "FFFFFF";
const LIGHT_TXT = "B0C4DE";
const BODY_BG = "F4F8FC"; // light body slides
const BODY_TXT = "1A2B3C";
const SUBHEAD = "1565C0";
// ── HELPERS ─────────────────────────────────────────────────────
function titleSlide(title, subtitle) {
const s = pres.addSlide();
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: DARK_BG } });
s.addShape(pres.ShapeType.rect, { x: 0, y: 4.5, w: 10, h: 1.125, fill: { color: ACCENT1 }, line: { color: ACCENT1 } });
s.addText(title, { x: 0.5, y: 1.1, w: 9, h: 1.4, fontSize: 38, bold: true, color: WHITE, align: "center", fontFace: "Calibri" });
if (subtitle) s.addText(subtitle, { x: 0.5, y: 2.7, w: 9, h: 0.7, fontSize: 18, color: ACCENT1, align: "center", fontFace: "Calibri" });
s.addText("Sources: Adams & Victor's Neurology 12e | Goldman-Cecil Medicine | Katzung Pharmacology 16e | Bradley & Daroff's Neurology", { x: 0.5, y: 4.6, w: 9, h: 0.4, fontSize: 9, color: DARK_BG, align: "center" });
}
function sectionSlide(num, title) {
const s = pres.addSlide();
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: MID_BG } });
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 0.12, h: 5.625, fill: { color: ACCENT1 }, line: { color: ACCENT1 } });
s.addText(`SECTION ${num}`, { x: 0.4, y: 1.6, w: 9, h: 0.5, fontSize: 14, color: ACCENT1, bold: true, charSpacing: 6, fontFace: "Calibri" });
s.addText(title, { x: 0.4, y: 2.2, w: 9, h: 1.1, fontSize: 34, bold: true, color: WHITE, fontFace: "Calibri" });
}
function bodySlide(title, bullets, opts = {}) {
const s = pres.addSlide();
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: BODY_BG } });
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 10, h: 0.72, fill: { color: DARK_BG }, line: { color: DARK_BG } });
s.addShape(pres.ShapeType.rect, { x: 0, y: 0.72, w: 10, h: 0.06, fill: { color: ACCENT1 }, line: { color: ACCENT1 } });
s.addText(title, { x: 0.3, y: 0.1, w: 9.4, h: 0.52, fontSize: 18, bold: true, color: WHITE, valign: "middle", fontFace: "Calibri", margin: 0 });
const rows = bullets.map((b, i) => ({
text: b,
options: { bullet: { indent: 14 }, color: BODY_TXT, fontSize: opts.fs || 13.5, fontFace: "Calibri", breakLine: i < bullets.length - 1 }
}));
s.addText(rows, { x: 0.35, y: 0.9, w: 9.3, h: 4.5, valign: "top" });
// slide number
s.addText(opts.slideNum ? `${opts.slideNum}` : "", { x: 9.5, y: 5.3, w: 0.4, h: 0.2, fontSize: 8, color: LIGHT_TXT, align: "right" });
}
function twoColSlide(title, leftTitle, leftBullets, rightTitle, rightBullets, opts = {}) {
const s = pres.addSlide();
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: BODY_BG } });
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 10, h: 0.72, fill: { color: DARK_BG }, line: { color: DARK_BG } });
s.addShape(pres.ShapeType.rect, { x: 0, y: 0.72, w: 10, h: 0.06, fill: { color: ACCENT1 }, line: { color: ACCENT1 } });
s.addText(title, { x: 0.3, y: 0.1, w: 9.4, h: 0.52, fontSize: 18, bold: true, color: WHITE, valign: "middle", fontFace: "Calibri", margin: 0 });
// left card
s.addShape(pres.ShapeType.rect, { x: 0.25, y: 0.88, w: 4.5, h: 4.55, fill: { color: "EAF2FB" }, line: { color: "C5D9EE" } });
s.addText(leftTitle, { x: 0.35, y: 0.93, w: 4.3, h: 0.38, fontSize: 13, bold: true, color: SUBHEAD, fontFace: "Calibri", margin: 0 });
const lRows = leftBullets.map((b, i) => ({ text: b, options: { bullet: { indent: 12 }, color: BODY_TXT, fontSize: opts.fs || 12.5, fontFace: "Calibri", breakLine: i < leftBullets.length - 1 } }));
s.addText(lRows, { x: 0.35, y: 1.35, w: 4.25, h: 3.9 });
// right card
s.addShape(pres.ShapeType.rect, { x: 5.25, y: 0.88, w: 4.5, h: 4.55, fill: { color: "EAF2FB" }, line: { color: "C5D9EE" } });
s.addText(rightTitle, { x: 5.35, y: 0.93, w: 4.3, h: 0.38, fontSize: 13, bold: true, color: SUBHEAD, fontFace: "Calibri", margin: 0 });
const rRows = rightBullets.map((b, i) => ({ text: b, options: { bullet: { indent: 12 }, color: BODY_TXT, fontSize: opts.fs || 12.5, fontFace: "Calibri", breakLine: i < rightBullets.length - 1 } }));
s.addText(rRows, { x: 5.35, y: 1.35, w: 4.25, h: 3.9 });
}
function tableSlide(title, headers, rows, opts = {}) {
const s = pres.addSlide();
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: BODY_BG } });
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 10, h: 0.72, fill: { color: DARK_BG }, line: { color: DARK_BG } });
s.addShape(pres.ShapeType.rect, { x: 0, y: 0.72, w: 10, h: 0.06, fill: { color: ACCENT1 }, line: { color: ACCENT1 } });
s.addText(title, { x: 0.3, y: 0.1, w: 9.4, h: 0.52, fontSize: 18, bold: true, color: WHITE, valign: "middle", fontFace: "Calibri", margin: 0 });
const tableData = [
headers.map(h => ({ text: h, options: { bold: true, color: WHITE, fill: DARK_BG, fontSize: 11, fontFace: "Calibri", align: "center", valign: "middle" } })),
...rows.map((row, ri) => row.map(cell => ({ text: cell, options: { color: BODY_TXT, fill: ri % 2 === 0 ? "FFFFFF" : "EAF2FB", fontSize: 10.5, fontFace: "Calibri", valign: "middle" } })))
];
s.addTable(tableData, { x: 0.25, y: 0.85, w: 9.5, h: 4.6, colW: opts.colW, border: { color: "C5D9EE" }, rowH: opts.rowH || 0.42 });
}
function emergencySlide(title, bullets) {
const s = pres.addSlide();
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: "1A0000" } });
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 10, h: 0.72, fill: { color: ACCENT_R }, line: { color: ACCENT_R } });
s.addText(title, { x: 0.3, y: 0.1, w: 9.4, h: 0.52, fontSize: 18, bold: true, color: WHITE, valign: "middle", fontFace: "Calibri", margin: 0 });
const rows = bullets.map((b, i) => ({ text: b, options: { bullet: { indent: 14 }, color: WHITE, fontSize: 13.5, fontFace: "Calibri", breakLine: i < bullets.length - 1 } }));
s.addText(rows, { x: 0.35, y: 0.9, w: 9.3, h: 4.5, valign: "top" });
}
function closingSlide() {
const s = pres.addSlide();
s.addShape(pres.ShapeType.rect, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: DARK_BG } });
s.addShape(pres.ShapeType.rect, { x: 0, y: 4.5, w: 10, h: 1.125, fill: { color: ACCENT1 }, line: { color: ACCENT1 } });
s.addText("Key Takeaways", { x: 0.5, y: 0.6, w: 9, h: 0.7, fontSize: 28, bold: true, color: WHITE, align: "center", fontFace: "Calibri" });
s.addText([
{ text: "Epilepsy = ≥2 unprovoked seizures; seizure = paroxysmal abnormal cerebral discharge", options: { bullet: true, breakLine: true } },
{ text: "ILAE 2017: Focal onset | Generalized onset | Unknown onset", options: { bullet: true, breakLine: true } },
{ text: "EEG + MRI are the cornerstones of investigation", options: { bullet: true, breakLine: true } },
{ text: "~2/3 of patients achieve seizure control with appropriate ASM monotherapy", options: { bullet: true, breakLine: true } },
{ text: "Status epilepticus: treat at 5 min — Benzodiazepine → IV ASM → Anesthesia", options: { bullet: true, breakLine: true } },
{ text: "Drug-refractory epilepsy: consider surgery, VNS, RNS, DBS, or ketogenic diet", options: { bullet: true } },
], { x: 0.5, y: 1.4, w: 9, h: 2.9, color: WHITE, fontSize: 13.5, fontFace: "Calibri" });
s.addText("Thank You", { x: 0.5, y: 4.55, w: 9, h: 0.5, fontSize: 20, bold: true, color: DARK_BG, align: "center", fontFace: "Calibri" });
}
// ════════════════════════════════════════════════════════════════
// SLIDE CONTENT
// ════════════════════════════════════════════════════════════════
// SLIDE 1 – Title
titleSlide("Epilepsy & Seizures", "A Comprehensive Medical Review\nDefinition · Epidemiology · Pathophysiology · Classification\nInvestigation · Treatment · Prevention");
// SLIDE 2 – Overview / Agenda
bodySlide("Presentation Outline", [
"1. Definition & Historical Background",
"2. Epidemiology",
"3. Aetiology & Risk Factors",
"4. Pathophysiology",
"5. ILAE 2017 Classification of Seizures",
"6. Epilepsy Syndromes",
"7. Clinical Features of Seizure Types",
"8. Differential Diagnosis",
"9. Investigations",
"10. Treatment – Antiseizure Medications (ASMs)",
"11. Treatment – Non-pharmacological",
"12. Status Epilepticus – Emergency Management",
"13. Special Populations",
"14. Prevention & Seizure Triggers",
"15. Prognosis & SUDEP",
], { fs: 13 });
// ── SECTION 1: DEFINITION ───────────────────────────────────────
sectionSlide(1, "Definition & Historical Background");
// SLIDE 4
bodySlide("Definitions", [
"SEIZURE – a paroxysmal, abnormal electrical discharge from cerebral neurons producing loss of consciousness, altered perception, convulsive movements, sensory disturbance, or autonomic features.",
"EPILEPSY – a disorder characterised by ≥2 unprovoked seizures occurring >24 h apart; OR 1 unprovoked seizure with ≥60% risk of recurrence over the next 10 years.",
"CONVULSION – subset of seizure involving involuntary repetitive muscular contractions; does NOT capture the full spectrum.",
"STATUS EPILEPTICUS – seizure lasting ≥5 min (GTC) or ≥10 min (focal/absence), or repeated seizures without full recovery.",
"PROVOKED (ACUTE SYMPTOMATIC) SEIZURE – occurs in direct relation to acute CNS insult (metabolic, toxic, structural); NOT classified as epilepsy.",
], { fs: 13 });
// SLIDE 5
bodySlide("Historical Milestones", [
"Ancient times – epilepsy called the 'Sacred Disease' (Hippocrates, ~400 BC); he attributed it to brain disorder, not divine intervention.",
"Medieval era – known as the 'Falling Sickness' or 'Falling Evil.'",
"1870 – Hughlings Jackson: seizures are 'an excessive and disorderly discharge of cerebral nervous tissue on muscles.'",
"1929 – Hans Berger invents the EEG, revolutionising seizure diagnosis.",
"1938 – First clinical use of phenytoin (Merritt & Putnam) — first non-sedating ASM.",
"1989 – ILAE first formal classification of epilepsies and epileptic syndromes.",
"2017 – ILAE revised Operational Classification of Seizure Types adopted worldwide.",
]);
// ── SECTION 2: EPIDEMIOLOGY ─────────────────────────────────────
sectionSlide(2, "Epidemiology");
// SLIDE 7
bodySlide("Global Burden", [
"~50 million people worldwide have epilepsy – one of the most common neurological disorders.",
"~2 million individuals with epilepsy in the United States alone.",
"Incidence: ~44 new cases per 100,000 persons/year (USA).",
"Lifetime prevalence: ~1 in 26 people in the US will develop epilepsy.",
"Nearly 1% of persons in the US will have epilepsy by age 20.",
"Over two-thirds of all epileptic seizures begin in childhood (peak: first year of life).",
"Second incidence peak occurs after age 60 – due to stroke, neurodegeneration, tumours.",
"80% of people with epilepsy live in low- and middle-income countries; many never receive treatment.",
]);
// SLIDE 8
twoColSlide("Epidemiology – Age & Sex Distribution",
"Age Distribution",
[
"Bimodal incidence: childhood & elderly",
"Neonates: metabolic, hypoxic-ischaemic causes",
"Infancy–childhood: genetic/structural syndromes",
"Adolescence: JME, absence epilepsy",
"Adults 15-64: trauma, CNS infections, tumours",
"Elderly >65: cerebrovascular disease #1 cause",
"Absence & myoclonic seizures peak in childhood",
"Complex partial (focal impaired awareness) predominate in adults",
],
"Sex & Socioeconomic",
[
"Slight male predominance overall",
"Some syndromes female-predominant (Rett syndrome, PCDH19 epilepsy)",
"Mortality 2–3× higher than general population",
"SUDEP (Sudden Unexpected Death in Epilepsy) ~1/1000 patient-years",
"Significant psychosocial burden: depression, anxiety, stigma",
"Employment and driving restrictions common",
"Annual economic cost in USA: >$15 billion",
]
);
// ── SECTION 3: AETIOLOGY ────────────────────────────────────────
sectionSlide(3, "Aetiology & Risk Factors");
// SLIDE 10
twoColSlide("Aetiology – ILAE Framework (2017)",
"Structural",
[
"Post-stroke or post-traumatic gliosis (50% of new adult focal)",
"Hippocampal sclerosis (mesial temporal lobe epilepsy)",
"Cortical dysplasia / malformations of cortical development",
"Brain tumours (primary & metastatic) – 15%",
"Vascular malformations (cavernomas, AVMs) – 15%",
"Traumatic brain injury",
"Post-infectious encephalitis/abscess",
"Perinatal hypoxic-ischaemic injury",
],
"Genetic / Metabolic / Immune / Unknown",
[
"Genetic: ion channel mutations (SCN1A, KCNQ2, GABRG2); copy-number variants",
"Metabolic: pyridoxine deficiency, mitochondrial disease, GLUT1 deficiency",
"Immune: autoimmune encephalitis (anti-NMDAR, LGI1, CASPR2)",
"Infectious: neurocysticercosis (most common cause worldwide), HSV encephalitis, HIV",
"Unknown – no cause found in ~40%",
"Risk factors: family history, febrile seizures, head trauma, CNS infections, prematurity",
]
);
// ── SECTION 4: PATHOPHYSIOLOGY ──────────────────────────────────
sectionSlide(4, "Pathophysiology");
// SLIDE 12
bodySlide("Cellular & Molecular Mechanisms", [
"Core principle: imbalance between EXCITATION and INHIBITION in neuronal networks.",
"Seizure initiation – 'paroxysmal depolarisation shift' (PDS): prolonged abnormal depolarisation of a neuron (epileptic focus) → burst of action potentials.",
"Excessive glutamate (AMPA & NMDA receptor) activation drives depolarisation.",
"Impaired GABA-mediated inhibition allows synchronous firing to spread.",
"Ion channel dysfunction is central: Na⁺ channel gain-of-function (e.g. SCN1A in Dravet), K⁺ channel loss-of-function (KCNQ2 in BFNC), GABA_A receptor mutations.",
"Focal seizures: abnormal discharge confined to one cortical network.",
"Generalised seizures: thalamocortical circuits involved from the outset; corticothalamic loop drives synchrony.",
"Epileptogenesis: process by which a normal brain becomes chronically epileptic — involves structural/synaptic remodelling, mossy fibre sprouting in hippocampus.",
]);
// SLIDE 13
bodySlide("Neuropathology of Common Epileptic Substrates", [
"HIPPOCAMPAL SCLEROSIS – neuronal loss in CA1, CA3, CA4 (Sommer's sector); gliosis; mossy fibre sprouting into molecular layer. Hallmark of mesial temporal lobe epilepsy.",
"FOCAL CORTICAL DYSPLASIA (FCD) – abnormal cortical lamination and neuronal morphology; highly epileptogenic; identified on high-resolution MRI (FLAIR sequences).",
"TUMOUR-RELATED EPILEPSY – low-grade tumours (DNET, ganglioglioma) near cortex are particularly epileptogenic; mechanisms include K⁺/glutamate dysregulation by tumour cells.",
"CORTICAL SCARS – post-traumatic or post-infarct gliosis creates irritative zone that generates ictal discharges.",
"STATUS EPILEPTICUS INJURY – prolonged seizure activity causes glutamate excitotoxicity → hippocampal neuronal death → worsening epileptogenesis (secondary hippocampal sclerosis).",
]);
// ── SECTION 5: CLASSIFICATION ───────────────────────────────────
sectionSlide(5, "ILAE 2017 Classification of Seizures");
// SLIDE 15
tableSlide("ILAE 2017 Seizure Classification", ["Category", "Type", "Former Name", "Key Feature"],
[
["Focal Onset", "Focal Aware", "Simple Partial", "Consciousness preserved"],
["Focal Onset", "Focal Impaired Awareness", "Complex Partial", "Consciousness impaired; automatisms"],
["Focal Onset", "Focal-to-Bilateral Tonic-Clonic", "Secondarily Generalised", "Focal onset → bilateral spread"],
["Generalised Onset", "Tonic-Clonic (GTC)", "Grand Mal", "LOC + tonic → clonic phases"],
["Generalised Onset", "Absence (typical)", "Petit Mal", "Brief stare; 3 Hz spike-wave"],
["Generalised Onset", "Absence (atypical)", "—", "Slower spike-wave; Lennox-Gastaut"],
["Generalised Onset", "Myoclonic", "—", "Sudden brief muscle jerks"],
["Generalised Onset", "Atonic (drop)", "Astatic", "Sudden loss of muscle tone"],
["Generalised Onset", "Epileptic Spasms", "Infantile Spasms", "West syndrome"],
["Unknown Onset", "Unknown", "—", "Insufficient data to classify"],
],
{ colW: [1.5, 2.0, 2.0, 3.5], rowH: 0.38 }
);
// ── SECTION 6: SYNDROMES ────────────────────────────────────────
sectionSlide(6, "Epilepsy Syndromes");
// SLIDE 17
tableSlide("Major Epilepsy Syndromes – Childhood Onset",
["Syndrome", "Age Onset", "Seizure Types", "EEG / Key Feature", "Prognosis"],
[
["West Syndrome", "3–12 mo", "Infantile spasms", "Hypsarrhythmia", "Poor if untreated; developmental regression"],
["Dravet Syndrome", "6–12 mo", "Febrile + afebrile; multiple types", "Non-specific; SCN1A mutation", "Drug-resistant; intellectual disability"],
["Childhood Absence Epilepsy", "4–12 yr", "Typical absence", "3 Hz generalised spike-wave", "Often resolves in adolescence"],
["Lennox-Gastaut Syndrome", "1–7 yr", "Tonic, atonic, atypical absence", "Slow spike-wave <2.5 Hz", "Drug-resistant; lifelong disability"],
["BECTS (Rolandic)", "3–13 yr", "Focal motor; nocturnal GTC", "Centrotemporal spikes", "Self-limiting; resolves by 16 yr"],
["Panayiotopoulos Syndrome", "3–6 yr", "Autonomic focal seizures", "Occipital spikes", "Benign; spontaneous remission"],
],
{ colW: [1.7, 0.9, 1.8, 2.2, 2.5], rowH: 0.44 }
);
// SLIDE 18
tableSlide("Major Epilepsy Syndromes – Adolescent & Adult Onset",
["Syndrome", "Age Onset", "Seizure Types", "Key Feature", "Treatment"],
[
["Juvenile Myoclonic Epilepsy (JME)", "12–20 yr", "Morning myoclonus + GTC ± absence", "4–6 Hz poly-spike-wave; photosensitive", "Valproate / levetiracetam; lifelong"],
["Juvenile Absence Epilepsy", "10–17 yr", "Absence + GTC", "3.5–4 Hz spike-wave", "Valproate / ethosuximide"],
["Mesial Temporal Lobe Epilepsy", "Any; peak 20s", "Focal impaired awareness; aura", "Hippocampal sclerosis on MRI", "Surgically remediable"],
["Autosomal Dom. Nocturnal Frontal Lobe", "Childhood–adult", "Nocturnal hypermotor seizures", "CHRNA4/CHRNB2 mutations", "Carbamazepine"],
["Progressive Myoclonic Epilepsies", "Variable", "Myoclonus + GTC + cerebellar signs", "Multiple causes (Unverricht, Lafora)", "Symptomatic; poor prognosis"],
],
{ colW: [2.2, 1.0, 2.0, 2.2, 1.8], rowH: 0.47 }
);
// ── SECTION 7: CLINICAL FEATURES ────────────────────────────────
sectionSlide(7, "Clinical Features of Seizure Types");
// SLIDE 20
bodySlide("Generalised Tonic-Clonic Seizure – Phase by Phase", [
"PRODROME (hours before): mood change, irritability, myoclonic jerks on awakening — not universal.",
"AURA: epigastric rising sensation, déjà vu, fear (if focal onset preceding GTC).",
"TONIC PHASE (10–20 sec): sudden LOC + fall; brief flexion → sustained rigid extension of neck, back, limbs; piercing cry (air through closed cords); apnea → cyanosis; pupils dilated & unreactive.",
"CLONIC PHASE (~30 sec): rhythmic flexor spasms at 8/sec → 4/sec; tongue bite (lateral margin); hypersalivation, sweating, tachycardia, elevated BP, urinary incontinence.",
"TERMINAL PHASE: movements cease; deep coma; stertorous breathing; pupils return to light.",
"POSTICTAL PHASE (min–hours): gradual awakening; confusion, agitation, amnesia for event; headache; muscle soreness.",
]);
// SLIDE 21
twoColSlide("Clinical Features – Focal & Absence Seizures",
"Focal Aware (Simple Partial)",
[
"Consciousness PRESERVED",
"Symptoms reflect cortical origin:",
"• Motor: Jacksonian march (hand → arm → face)",
"• Somatosensory: tingling, numbness",
"• Visual: lights, spots, formed images",
"• Auditory: buzzing, voices",
"• Autonomic: flushing, epigastric sensation",
"• Psychic: déjà vu, jamais vu, fear",
"Todd's paralysis: post-ictal focal weakness",
],
"Absence (Typical) Seizure",
[
"Sudden onset & offset (5–20 sec)",
"Blank staring, unresponsive",
"Subtle automatisms (eye blinking, lip smacking)",
"NO fall, NO postictal confusion",
"Easily induced by hyperventilation",
"EEG: classic 3 Hz generalised spike-wave",
"Multiple episodes per day possible",
"May be mistaken for daydreaming",
]
);
// SLIDE 22
twoColSlide("Clinical Features – Focal Impaired Awareness & Myoclonic",
"Focal Impaired Awareness (Complex Partial)",
[
"Consciousness IMPAIRED (not fully lost)",
"Most often temporal lobe origin",
"Typical aura: rising epigastric sensation",
"Automatisms: lip smacking, hand fumbling, chewing, ambulation",
"Duration: 1–3 minutes",
"Post-ictal confusion & amnesia",
"Can spread to bilateral tonic-clonic",
"Hippocampal sclerosis on MRI common",
],
"Myoclonic & Atonic Seizures",
[
"MYOCLONIC: sudden brief bilateral jerks, typically proximal limbs",
"• Morning predominance in JME",
"• Preserved consciousness",
"• Can cause drop or fall",
"ATONIC (Drop Attacks):",
"• Sudden loss of muscle tone → fall",
"• Risk of head injury → helmet use",
"• Common in Lennox-Gastaut syndrome",
"• Very brief; rapid recovery",
]
);
// ── SECTION 8: DIFFERENTIAL DIAGNOSIS ───────────────────────────
sectionSlide(8, "Differential Diagnosis");
// SLIDE 24
bodySlide("Differential Diagnosis of Seizures", [
"SYNCOPE – most common mimic; prodrome of lightheadedness, dimming vision; brief convulsive movements possible (anoxic convulsions); rapid full recovery; triggered by standing/pain/emotion.",
"TRANSIENT ISCHAEMIC ATTACK (TIA) – usually negative symptoms (weakness, numbness) vs positive motor symptoms of seizure; no postictal phase.",
"MIGRAINE with aura – slow spreading aura (minutes); headache follows; no LOC.",
"PSYCHOGENIC NON-EPILEPTIC SEIZURES (PNES) – resemble seizures; variable across episodes; prominent pelvic thrusting, eye closure during 'convulsions'; no EEG correlate; often history of trauma/abuse.",
"PANIC ATTACKS – prolonged duration (>5 min); linked to specific triggers; no tonic-clonic activity; no postictal state.",
"HYPOGLYCAEMIA / HYPONATRAEMIA – acute symptomatic seizures; blood tests reveal cause; correct metabolic abnormality.",
"PAROXYSMAL MOVEMENT DISORDERS – dyskinesias, chorea; maintain consciousness; no EEG correlate.",
"NARCOLEPSY / CATAPLEXY – sudden muscle atonia triggered by emotion; mimics atonic seizures.",
]);
// ── SECTION 9: INVESTIGATIONS ────────────────────────────────────
sectionSlide(9, "Investigations");
// SLIDE 26
bodySlide("Investigation Overview", [
"History & Eyewitness Account – cornerstone; detailed description of events before, during, and after episode.",
"ELECTROENCEPHALOGRAM (EEG) – keystone investigation in all patients with seizures and epilepsy.",
"BRAIN MRI – should be performed in essentially ALL patients with new-onset seizures.",
"BLOOD TESTS – electrolytes, glucose, calcium, magnesium, liver/renal function, FBC, toxicology screen.",
"LUMBAR PUNCTURE – indicated if CNS infection suspected or in HIV-positive patients.",
"GENETIC TESTING – guided by syndrome; highest yield with intellectual disability + autism + dysmorphic features.",
"Functional imaging (PET, SPECT), magnetoencephalography (MEG) – used in pre-surgical evaluation.",
"Neuropsychological assessment – pre-surgical mapping of cognitive function.",
]);
// SLIDE 27
bodySlide("EEG – The Keystone Investigation", [
"EEG diagnoses epilepsy definitively ONLY if electrical seizure is recorded simultaneously with clinical event.",
"Interictal initial EEG is NORMAL in up to 60% of known epilepsy patients — normal EEG does NOT exclude epilepsy.",
"Epileptiform abnormalities present in >80% of focal epilepsy patients if 3 or more EEGs are performed.",
"Syndrome-specific patterns:",
" • Generalised absence epilepsy: 3 Hz spike-and-wave",
" • West syndrome: hypsarrhythmia (chaotic high-amplitude pattern)",
" • Rolandic epilepsy: centrotemporal spikes",
" • Juvenile myoclonic epilepsy: 4–6 Hz poly-spike-and-wave",
" • Lennox-Gastaut: slow spike-and-wave (<2.5 Hz)",
"Video-EEG monitoring – mandatory for pre-surgical evaluation and when diagnosis is uncertain.",
"Continuous EEG – used in ICU for suspected nonconvulsive status epilepticus in comatose patients.",
]);
// SLIDE 28
bodySlide("Neuroimaging in Epilepsy", [
"BRAIN MRI (preferred over CT) – performed in essentially all patients with new-onset seizures.",
"Most common findings in adults with new-onset focal seizures:",
" • Post-stroke/post-traumatic gliosis: ~50%",
" • Tumours (primary/metastatic): ~15%",
" • Vascular malformations: ~15%",
" • Developmental abnormalities (FCD, cortical dysplasia): ~15%",
" • Mesial temporal sclerosis: ~9%",
"FLAIR sequences – increased sensitivity for hippocampal sclerosis and focal cortical dysplasia.",
"PET (FDG-PET) – identifies hypometabolic seizure focus; used in pre-surgical workup.",
"SPECT (ictal > interictal) – blood flow imaging; ictal SPECT identifies hyperperfused seizure onset zone.",
"MEG (magnetoencephalography) – maps interictal discharges + eloquent cortex for surgical planning.",
]);
// ── SECTION 10: ASM TREATMENT ────────────────────────────────────
sectionSlide(10, "Treatment – Antiseizure Medications (ASMs)");
// SLIDE 30
bodySlide("General Principles of ASM Therapy", [
"Goal: complete seizure freedom with minimal adverse effects.",
"Monotherapy preferred — reduces adverse effects; adequate in ~2/3 of patients.",
"Choice depends on seizure type / epilepsy syndrome and patient factors.",
"Start low, titrate slowly to effective dose.",
"Pharmacoresistance: failure of ≥2 appropriate ASMs at adequate doses = drug-refractory epilepsy (affects ~30–40%).",
"Women of childbearing age: avoid valproate if possible due to teratogenicity (neural tube defects, cognitive effects on offspring).",
"Monitor for idiosyncratic reactions: rash (carbamazepine, lamotrigine — SJS), hepatotoxicity (valproate), aplastic anaemia (felbamate).",
"Drug interactions: enzyme-inducers (carbamazepine, phenytoin, phenobarb) reduce efficacy of OCP, anticoagulants, immunosuppressants.",
]);
// SLIDE 31
tableSlide("ASM Selection by Seizure Type",
["Seizure Type", "First-Line ASMs", "Alternative ASMs", "Avoid"],
[
["Generalised Tonic-Clonic", "Valproate, Levetiracetam, Lamotrigine", "Topiramate, Zonisamide", "Carbamazepine (worsens absence/myoclonus)"],
["Typical Absence", "Ethosuximide, Valproate, Lamotrigine", "Zonisamide, Clobazam", "Carbamazepine, Phenytoin, Gabapentin"],
["Myoclonic", "Valproate, Levetiracetam, Clonazepam", "Zonisamide, Topiramate", "Carbamazepine, Gabapentin, Pregabalin"],
["Focal (Aware/Impaired)", "Carbamazepine, Oxcarbazepine, Levetiracetam, Lamotrigine", "Lacosamide, Brivaracetam", "—"],
["Focal-to-Bilateral TC", "Carbamazepine, Levetiracetam, Lamotrigine", "Lacosamide, Eslicarbazepine", "—"],
["Lennox-Gastaut", "Valproate, Lamotrigine, Clobazam, Rufinamide", "Fenfluramine, Cannabidiol (CBD)", "Vigabatrin (worsens absence)"],
["Infantile Spasms (West)", "ACTH, Vigabatrin, Prednisolone", "Pyridoxine (if B6-dep.)", "—"],
],
{ colW: [2.0, 2.5, 2.5, 2.5], rowH: 0.44 }
);
// SLIDE 32
bodySlide("Mechanisms of Major ASMs", [
"SODIUM CHANNEL BLOCKERS (most common mechanism) – phenytoin, carbamazepine, oxcarbazepine, lamotrigine, lacosamide, eslicarbazepine → reduce sustained repetitive firing by prolonging Na⁺ channel inactivation.",
"CALCIUM CHANNEL MODIFIERS – ethosuximide, valproate → block T-type Ca²⁺ channels in thalamic neurons → suppress absence seizures.",
"GABA ENHANCEMENT – benzodiazepines (GABA_A Cl⁻ channel opening), phenobarbitone (GABA_A duration), vigabatrin (inhibits GABA transaminase → ↑ GABA), tiagabine (blocks GABA reuptake).",
"GLUTAMATE ANTAGONISM – perampanel (AMPA receptor antagonist) — first in class.",
"SV2A (Synaptic Vesicle Protein 2A) modulation – levetiracetam, brivaracetam → reduce presynaptic neurotransmitter release.",
"MULTIPLE MECHANISMS – valproate (Na⁺ block + T-Ca²⁺ block + ↑GABA), topiramate (Na⁺ + GABA + AMPA block + CA inhibition), zonisamide (Na⁺ + T-Ca²⁺).",
]);
// ── SECTION 11: NON-PHARM TREATMENT ─────────────────────────────
sectionSlide(11, "Treatment – Non-Pharmacological");
// SLIDE 34
bodySlide("Epilepsy Surgery", [
"Indicated in pharmacoresistant epilepsy (failed ≥2 ASMs) with identifiable seizure focus.",
"Pre-surgical evaluation: video-EEG, high-resolution MRI, neuropsychological testing, PET, MEG, Wada test (language/memory lateralisation).",
"TEMPORAL LOBE RESECTION – most commonly performed; ~60–70% seizure-free rate at 2 years; most effective for mesial temporal lobe epilepsy with hippocampal sclerosis.",
"EXTRATEMPORAL CORTICAL RESECTION – lower success rates; requires precise localisation.",
"LESIONECTOMY – resection of discrete lesion (tumour, cavernoma, FCD); potentially curative.",
"HEMISPHERECTOMY / HEMISPHEROTOMY – for severe unilateral hemisphere disease (Rasmussen's encephalitis, large perinatal stroke); best outcomes when done early.",
"CORPUS CALLOSOTOMY – palliative for drop attacks (atonic seizures); reduces spread between hemispheres.",
]);
// SLIDE 35
bodySlide("Neurostimulation & Dietary Therapies", [
"VAGUS NERVE STIMULATOR (VNS) – implanted pulse generator; helical electrode on left vagus nerve; open-loop stimulation; approved for drug-refractory focal seizures; ~50% achieve ≥50% seizure reduction.",
"RESPONSIVE NEUROSTIMULATOR (RNS) – closed-loop system; detects abnormal EEG pattern in seizure focus → delivers stimulation to prevent seizure.",
"DEEP BRAIN STIMULATION (DBS) – bilateral open-loop stimulation of anterior nuclei of thalamus; indicated as adjunctive therapy for focal seizures ± secondary generalisation.",
"KETOGENIC DIET – high fat, low carbohydrate, controlled protein; produces ketosis → anticonvulsant effects; particularly effective in children with refractory epilepsy; beneficial in specific metabolic epilepsies (GLUT1 deficiency, pyruvate dehydrogenase deficiency).",
"MODIFIED ATKINS DIET / LOW GLYCAEMIC INDEX DIET – less restrictive alternatives to classic ketogenic diet; comparable efficacy in some studies.",
"TRANSCRANIAL MAGNETIC STIMULATION (TMS) – investigational; may reduce cortical excitability at seizure focus.",
]);
// ── SECTION 12: STATUS EPILEPTICUS ───────────────────────────────
sectionSlide(12, "Status Epilepticus – Emergency Management");
// SLIDE 37 – emergency style
emergencySlide("Status Epilepticus – Recognition", [
"DEFINITION: GTC seizure ≥5 minutes OR focal/absence seizure ≥10 minutes OR repeated seizures without full recovery between.",
"TYPES:",
" 1. Generalised Convulsive SE – bilateral limb jerking + impaired consciousness; LIFE-THREATENING",
" 2. Nonconvulsive SE (NCSE) – behaviour change + continuous EEG epileptiform activity WITHOUT major motor signs",
" • Absence SE, Focal SE with/without impaired awareness",
" • NCSE in coma – often follows undertreated convulsive SE; requires EEG for diagnosis",
"RISKS OF DELAY: neuronal injury (glutamate excitotoxicity → hippocampal cell death), systemic complications (hyperthermia, acidosis, rhabdomyolysis), death",
"ECG and O₂ monitoring mandatory; establish IV access; check glucose",
]);
// SLIDE 38 – emergency style
emergencySlide("Status Epilepticus – Treatment Algorithm", [
"T = 0: Assess ABCs; O₂; IV access; bloods (glucose, electrolytes, drug levels, toxicology); ECG monitoring",
"T = 5 min — FIRST LINE (Benzodiazepines):",
" • IV Lorazepam 0.1 mg/kg (max 4 mg) — preferred",
" • IV Diazepam 0.15–0.2 mg/kg (max 10 mg) — alternative",
" • IM Midazolam 10 mg (>40 kg) or 5 mg (13–40 kg) — prehospital / no IV access",
" • Rectal diazepam / intranasal midazolam — if above unavailable",
"T = 20 min — SECOND LINE (if seizure continues): IV Levetiracetam 60 mg/kg (max 4500 mg) OR IV Valproate 40 mg/kg (max 3000 mg) OR IV Fosphenytoin 20 PE/kg (max 1500 PE) — equally effective",
"T = 40 min — REFRACTORY SE: ICU admission; anaesthetic infusions — Propofol OR Midazolam infusion OR Thiopental/Pentobarbital; continuous EEG monitoring required",
"SUPER-REFRACTORY SE (≥24h): consider ketamine, lacosamide, ketogenic diet, immunotherapy",
]);
// ── SECTION 13: SPECIAL POPULATIONS ─────────────────────────────
sectionSlide(13, "Special Populations");
// SLIDE 40
twoColSlide("Special Populations",
"Women with Epilepsy",
[
"Catamenial epilepsy: seizures cluster around menstruation (progesterone withdrawal)",
"Contraception: enzyme-inducing ASMs reduce OCP efficacy; use ≥50 µg EE pill or non-hormonal method",
"Pregnancy counselling BEFORE conception:",
"• Lowest effective ASM dose",
"• Avoid valproate (teratogen; 4–10× risk NTD; cognitive effects in child)",
"• Folic acid 5 mg/day pre-conception",
"• Lamotrigine / levetiracetam safest",
"• Seizure monitoring frequency ↑",
"Breastfeeding: generally permitted; most ASMs low excretion",
],
"Elderly & Paediatric",
[
"ELDERLY:",
"• Most common new epilepsy after stroke",
"• Drug interactions with polypharmacy",
"• Prefer levetiracetam, lamotrigine, gabapentin (better tolerated)",
"• Fall risk with sedating ASMs",
"PAEDIATRIC:",
"• Fever can lower seizure threshold",
"• Febrile seizures (6 mo – 6 yr): usually benign; prophylactic ASMs rarely needed",
"• Neonatal seizures: treat underlying cause (hypoglycaemia, hypocalcaemia) first",
"• Infantile spasms: ACTH or vigabatrin — early treatment critical",
]
);
// SLIDE 41
twoColSlide("Epilepsy & Driving / Psychosocial Issues",
"Driving",
[
"Most countries: seizure-free period required (6–12 months) before driving",
"Physician must counsel patients and document",
"Reporting obligations vary by jurisdiction",
"Commercial vehicle licensing has stricter rules",
"Breakthrough seizures while driving = significant mortality risk",
],
"Psychiatric & Social Comorbidities",
[
"Depression: 2–3× more prevalent in epilepsy than general population",
"Anxiety disorders: highly prevalent",
"Cognitive impairment: memory deficits common in TLE",
"Stigma: major barrier to treatment adherence globally",
"Employment: epilepsy affects career choices and job security",
"SUDEP risk: highest in nocturnal uncontrolled GTC; sleeping alone increases risk",
"Comprehensive epilepsy care includes neurologist + neuropsychologist + social worker",
]
);
// ── SECTION 14: PREVENTION ───────────────────────────────────────
sectionSlide(14, "Prevention & Seizure Triggers");
// SLIDE 43
twoColSlide("Seizure Triggers (Common)",
"Lifestyle Triggers",
[
"Sleep deprivation – most potent trigger; adequate sleep critical",
"Alcohol consumption / alcohol withdrawal",
"Recreational drug use (cocaine, amphetamines)",
"Missed ASM doses – most common preventable cause of breakthrough seizure",
"Physical or emotional stress",
"Fever / systemic illness",
"Menstrual cycle (catamenial epilepsy)",
"Flashing lights / visual patterns (photosensitive epilepsy – ~3% of epilepsy)",
"Overhydration / electrolyte disturbance",
],
"Medical / Pharmacological Triggers",
[
"Withdrawal of ASMs (abrupt)",
"Medications lowering seizure threshold:",
"• Antibiotics: fluoroquinolones, imipenem",
"• Antidepressants: bupropion, clomipramine",
"• Antipsychotics: clozapine, chlorpromazine",
"• Theophylline, tramadol, lithium toxicity",
"Drug–drug interactions reducing ASM levels",
"Hypoglycaemia, hyponatraemia, hypocalcaemia",
"Contrast agents (intrathecal – rare)",
]
);
// SLIDE 44
bodySlide("Primary & Secondary Prevention", [
"PRIMARY PREVENTION (preventing epilepsy from developing):",
" • Reduce head trauma: helmet laws, seatbelts, fall prevention in elderly",
" • Reduce CNS infections: vaccination (measles, H. influenzae, Neisseria meningitidis), anthelmintic campaigns (neurocysticercosis)",
" • Perinatal care: prevent hypoxic-ischaemic birth injury with skilled obstetric care",
" • Stroke prevention (hypertension, AF management, lipid control) — critical in elderly",
" • Avoid teratogenic exposure in utero (valproate in pregnancy)",
"SECONDARY PREVENTION (preventing seizure recurrence once epilepsy diagnosed):",
" • Adherence to ASMs — missed doses are #1 cause of breakthrough seizures",
" • Avoid known personal triggers (maintain diary)",
" • Regular adequate sleep; avoid sleep deprivation",
" • Abstain from alcohol / recreational drugs",
" • Wear medical alert bracelet; ensure caregivers know rescue medication protocol",
"TERTIARY PREVENTION (minimising disability):",
" • Access to epilepsy specialist care; surgical evaluation when pharmacoresistant",
" • Psychosocial support; driving safety counselling; vocational rehabilitation",
]);
// SLIDE 45
bodySlide("Patient & Caregiver Education – First Aid for Seizures", [
"STAY calm and stay with the person.",
"TIME the seizure — call emergency services if >5 minutes.",
"PROTECT from injury: clear area, cushion head, loosen tight clothing.",
"POSITION: place in recovery (lateral) position when convulsions stop — prevents aspiration.",
"DO NOT restrain movements or put anything in the mouth.",
"DO NOT give food or water until fully conscious.",
"RESCUE MEDICATION: administer prescribed rescue benzodiazepine (rectal diazepam, intranasal midazolam, buccal midazolam) if seizure ≥5 minutes.",
"AFTER seizure: stay until fully conscious; explain what happened; be supportive.",
"DOCUMENT: date, time, duration, nature of seizure; report to physician.",
]);
// ── SECTION 15: PROGNOSIS & SUDEP ───────────────────────────────
sectionSlide(15, "Prognosis & SUDEP");
// SLIDE 47
bodySlide("Prognosis of Epilepsy", [
"Overall: ~60–70% of patients achieve long-term seizure remission with appropriate treatment.",
"~2/3 of patients achieve seizure control with first or second appropriate ASM.",
"~30–40% are pharmacoresistant; surgical evaluation should be pursued early.",
"Favourable prognosis: idiopathic/genetic epilepsy (especially childhood onset), normal neurological exam, normal MRI, single seizure type.",
"Unfavourable prognosis: structural aetiology, abnormal MRI, early onset, multiple seizure types, intellectual disability.",
"Seizure remission after ASM withdrawal: ~60% remain seizure-free after slow taper if seizure-free ≥2 years and normal EEG/MRI.",
"Temporal lobe epilepsy surgery: ~60–70% seizure-free at 2 years vs <10% with continued medical management.",
]);
// SLIDE 48
bodySlide("SUDEP – Sudden Unexpected Death in Epilepsy", [
"DEFINITION: sudden, unexpected, witnessed or unwitnessed, non-traumatic and non-drowning death in epilepsy, with or without evidence of seizure.",
"INCIDENCE: ~1 per 1000 patient-years in adults; up to 1 per 150 in high-risk groups.",
"RISK FACTORS:",
" • Nocturnal generalised tonic-clonic seizures – strongest risk factor",
" • High seizure frequency (≥3 GTC/year)",
" • Sleeping alone (unable to intervene)",
" • Uncontrolled epilepsy; non-adherence to ASMs",
" • Male sex; early onset; duration of epilepsy >15 years",
"MECHANISM (incompletely understood): post-ictal autonomic dysfunction → cardiac arrhythmia (prolonged QT, bradycardia), central respiratory depression → asphyxia.",
"PREVENTION: optimise seizure control; nocturnal monitoring devices / mattress sensors; supervised sleeping; avoid prone sleeping position.",
]);
// SLIDE 49
bodySlide("Antiseizure Drug Reference Summary", [
"VALPROATE – broad spectrum; Na⁺ + T-Ca²⁺ + ↑GABA; avoid in women of childbearing age; monitor LFTs, platelets; pancreatitis, weight gain, tremor.",
"LAMOTRIGINE – broad spectrum; Na⁺ blocker; slow titration required (SJS risk); interacts with valproate; safe in pregnancy (relatively).",
"LEVETIRACETAM – broad spectrum; SV2A; well tolerated; IV form available; behavioural side effects (irritability, depression) notable.",
"CARBAMAZEPINE / OXCARBAZEPINE – focal epilepsy; Na⁺ blocker; enzyme inducer (carbamazepine); hyponatraemia with oxcarbazepine; avoid in generalised epilepsy.",
"ETHOSUXIMIDE – absence only; T-Ca²⁺ blocker; nausea; not effective for GTC.",
"PHENYTOIN / FOSPHENYTOIN – Na⁺ blocker; narrow therapeutic window; gingival hyperplasia, hirsutism, ataxia; zero-order kinetics (non-linear).",
"TOPIRAMATE – Na⁺ + AMPA + CA; cognitive side effects ('Dopamax'); kidney stones; weight loss; teratogenic.",
"LACOSAMIDE – Na⁺ (slow inactivation); focal seizures; PR prolongation; IV form.",
"PHENOBARBITONE – GABA_A; sedation; cognitive impairment; enzyme inducer; widely used in low-income settings.",
]);
// SLIDE 50 – Closing
closingSlide();
// ── WRITE FILE ───────────────────────────────────────────────────
pres.writeFile({ fileName: "/home/daytona/workspace/epilepsy-pptx/Epilepsy_Seizures_Comprehensive.pptx" })
.then(() => console.log("✅ PPTX saved successfully"))
.catch(e => { console.error("❌ Error:", e); process.exit(1); });
Running Command
cd /home/daytona/workspace/epilepsy-pptx && node build.js 2>&1
Running Command
ls -lh /home/daytona/workspace/epilepsy-pptx/Epilepsy_Seizures_Comprehensive.pptx
Your 50-slide PowerPoint is ready:
Epilepsy Seizures Comprehensive
Presentation · PPTX
What's Inside (50 Slides)
The deck is designed with a professional deep-navy + sky-blue colour scheme and covers every topic you requested, sourced from Adams & Victor's Neurology 12e, Goldman-Cecil Medicine, Katzung's Pharmacology 16e, and Bradley & Daroff's Neurology:
| # | Section | Slides |
|---|---|---|
| 1 | Title & Outline | 1–2 |
| 2 | Definition & History | 3–5 (Hughlings Jackson, EEG history, terminology) |
| 3 | Epidemiology | 6–8 (global burden, age/sex distribution, bimodal incidence) |
| 4 | Aetiology & Risk Factors | 9–10 (structural, genetic, metabolic, immune, infectious) |
| 5 | Pathophysiology | 11–13 (PDS, ion channels, GABA/glutamate imbalance, hippocampal sclerosis, FCD) |
| 6 | ILAE 2017 Classification | 14–15 (full table: focal / generalised / unknown onset with old vs new terms) |
| 7 | Epilepsy Syndromes | 16–18 (West, Dravet, Childhood Absence, LGS, BECTS, JME, MTLE — with tables) |
| 8 | Clinical Features | 19–22 (GTC phase-by-phase, focal aware, absence, focal impaired awareness, myoclonic/atonic) |
| 9 | Differential Diagnosis | 23–24 (syncope, TIA, PNES, panic, migraine, metabolic) |
| 10 | Investigations | 25–28 (EEG patterns, MRI findings, genetic testing, MEG, PET/SPECT) |
| 11 | ASM Treatment | 29–32 (principles, selection by seizure type table, mechanisms) |
| 12 | Non-pharmacological Tx | 33–35 (surgery, VNS, RNS, DBS, ketogenic diet) |
| 13 | Status Epilepticus | 36–38 (recognition + emergency algorithm — red slide design) |
| 14 | Special Populations | 39–41 (women, elderly, paediatric, driving, psychosocial) |
| 15 | Prevention & Triggers | 42–45 (triggers, primary/secondary/tertiary prevention, first aid) |
| 16 | Prognosis & SUDEP | 46–48 (remission rates, surgery outcomes, SUDEP risk factors) |
| 17 | Drug Reference | 49 (valproate, lamotrigine, levetiracetam, carbamazepine, phenytoin, etc.) |
| 18 | Key Takeaways | 50 |
This is a shared conversation. Sign in to Orris to start your own chat.