Give me a detailed notes of aortic regurgitation on echo with all the criteria
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Loading Image
I now have comprehensive content from the authoritative sources. Let me compile the complete, detailed notes.
Aortic Regurgitation (AR) on Echocardiography - Detailed Notes
Sources: Textbook of Clinical Echocardiography (Otto), Fuster & Hurst's The Heart 15e, Harrison's Principles 22e
1. Overview and Role of Echocardiography
Echocardiography is the imaging modality of choice for:
- Detection and etiology of AR
- Grading regurgitant severity
- Assessing LV size and systolic function (serial surveillance)
- Timing surgical intervention
A complete echo evaluation covers: valve anatomy → regurgitant severity → LV response → aortic root dimensions.
2. Valve Anatomy Assessment (2D Imaging)
Views Used
- Parasternal long-axis (PLAX) - best for leaflet morphology, regurgitant jet origin
- Parasternal short-axis (PSAX) - number of cusps, commissural fusion, calcification
- Apical 5-chamber / 3-chamber - overall valve function
- Suprasternal notch (SSN) and subcostal - aortic flow reversal
Key 2D Findings by Etiology
| Phenotype | 2D Echo Findings |
|---|---|
| Bicuspid aortic valve | Two cusps on short axis, raphe (incomplete fusion line), systolic doming, eccentric jet |
| Rheumatic | Commissural fusion, thickened leaflet tips, associated mitral involvement |
| Calcific degenerative | Leaflet calcification, concentric involvement, may coexist with stenosis |
| Aortic root dilation (Marfan, HTN) | Normal leaflets with central regurgitation, effacement of sinotubular junction |
| Endocarditis | Perforated or flail leaflet, vegetations, paravalvular abscess |
| Aortic dissection | Flail leaflet, dissection flap visible, compromised commissural support |
3. Indirect Signs of AR (2D / M-mode)
These are clues on standard imaging that suggest a previously unsuspected diagnosis:
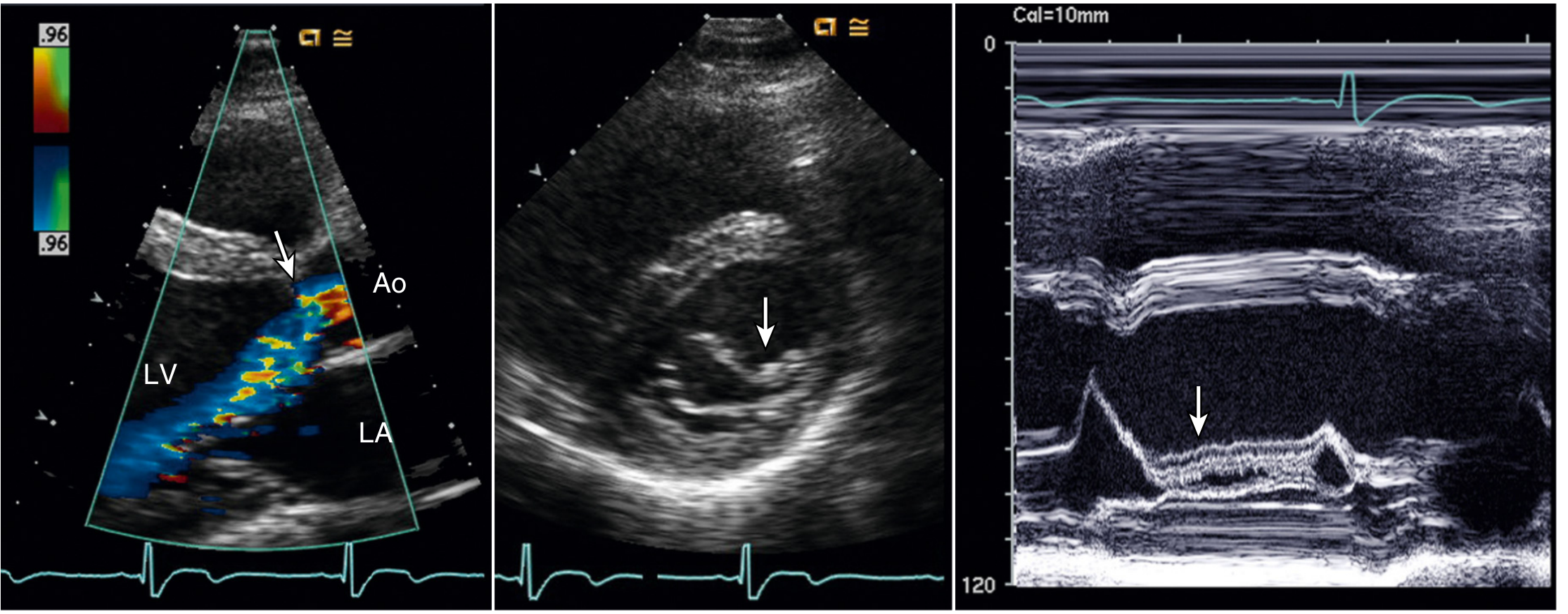
- Anterior mitral leaflet flutter (M-mode): High-frequency diastolic vibration of the anterior mitral leaflet caused by impingement of the AR jet - a classic indirect sign
- Reverse doming of anterior mitral leaflet: In PSAX view the anterior leaflet curves oppositely to rheumatic MS; caused by the AR jet pushing it posteriorly
- Increased E-point septal separation (EPSS): Reflects elevated LV filling or reduced LV function
- Premature mitral valve closure: Seen in acute severe AR when LV diastolic pressure rises rapidly above LA pressure - indicates need for urgent surgery
- Jet lesion: Area of increased echogenicity on the septum or anterior mitral leaflet where the AR jet impinges (fibrotic reaction, seen on 2D)
- LV dilation: Progressive in chronic AR - the largest end-diastolic volumes of all valvular heart diseases
4. Evaluation of Aortic Regurgitant Severity
Step 1 - Screening Examination (Color Flow + CW Doppler)
- Color flow imaging in PLAX and PSAX identifies the AR jet origin and provides an initial impression of severity
- A central jet filling <25% of LVOT diameter is consistent with mild AR
- CW Doppler from apical approach: a weak or absent diastolic signal below the baseline = no significant AR
- If the screen is positive for more than mild AR, proceed to vena contracta measurement
Step 2 - Vena Contracta Width (Color Flow, PLAX)
The vena contracta = the narrowest segment of the regurgitant jet, located between the proximal flow convergence region and distal jet expansion, measured perpendicular to flow direction.
Technique: PLAX view, zoom mode, narrow sector, angulate medially and laterally to find the narrowest segment.
| Vena Contracta Width | Severity |
|---|---|
| < 0.3 cm | Mild |
| 0.3 - 0.6 cm | Moderate (indeterminate) |
| > 0.6 cm | Severe |
Caveats:
- Accurate for simple (single) jets; not validated for multiple jets
- Eccentric jets: measure perpendicular to the jet long axis, not the LVOT long axis
- 3D vena contracta area shows promise for non-symmetrical orifices but limited by low frame rates
Step 3 - Jet Width / LVOT Ratio (Color Flow, PLAX)
- Measured in PLAX as the ratio of AR jet width at its origin to the LVOT diameter
- Jet width/LVOT ratio >65% is consistent with severe AR
- Inaccurate for eccentric jets - use vena contracta instead in those cases
- A jet/LVOT area ratio >60% by planimetry of the PSAX view is another criterion
Step 4 - Aortic Diastolic Flow Reversal (Pulsed Doppler)
Reversal of blood flow in the descending and abdominal aorta during diastole reflects the regurgitant volume returning to the LV. The further downstream the holodiastolic flow reversal extends, the more severe the AR.
Technique: Sample volume 2-3 mm, decrease wall filters, use subcostal and suprasternal notch views.
| Finding | Severity |
|---|---|
| No holodiastolic reversal | Mild |
| Holodiastolic reversal in descending thoracic aorta only | Moderate (at least moderate, less specific for severe) |
| Holodiastolic reversal in proximal abdominal aorta | Severe |
| Cutoff velocity: > 20 cm/s peak end-diastolic reversal | Severe |
- In the suprasternal notch view, holodiastolic flow reversal can be detected in the proximal descending thoracic aorta
- The subcostal window is used to record flow in the proximal abdominal aorta (most specific site for severe AR)
Step 5 - Continuous-Wave (CW) Doppler Signal
Recorded from the apical window with careful transducer angulation to align with the AR jet. Provides two key pieces of information:
A. Signal Density (Qualitative)
- Compare intensity of the retrograde diastolic signal to the antegrade systolic flow signal
- Dense signal = equal density to antegrade → suggests severe AR (large regurgitant volume)
- Faint/incomplete signal → mild AR
B. Deceleration Slope / Pressure Half-Time (PHT)
The AR signal slope reflects the rate of pressure equalization between the aorta and LV during diastole:
- A flat slope (slow deceleration) = aorta-LV pressure gradient maintained throughout diastole = mild AR
- A steep slope (rapid deceleration) = rapid pressure equalization = severe AR (especially acute)
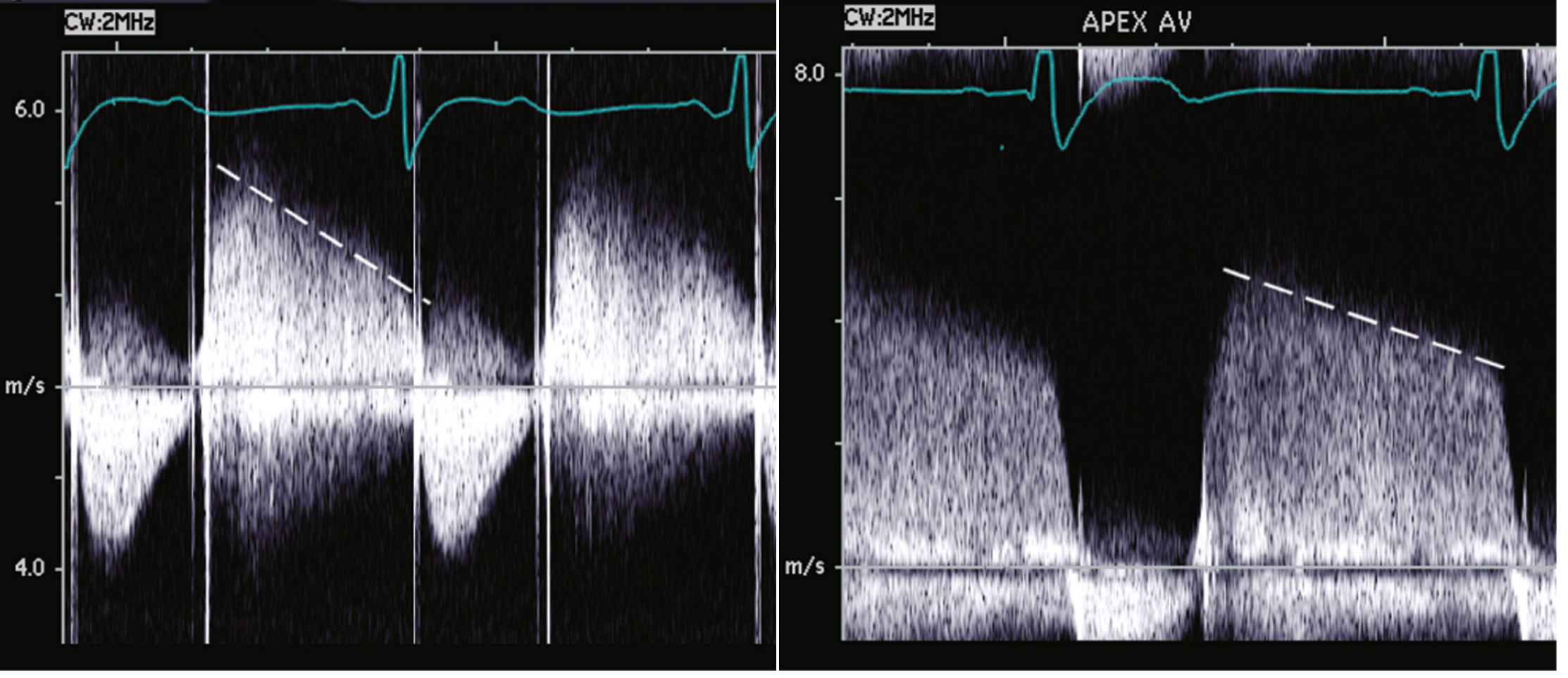
| PHT | Severity |
|---|---|
| > 500 ms | Mild AR |
| 200 - 500 ms | Moderate |
| < 200 ms | Severe AR |
Important caveats for PHT:
- PHT is affected by LV compliance and arterial pressure, not just regurgitant severity
- Accuracy depends heavily on correct beam alignment with the AR jet - off-axis measurements will underestimate the slope
- In chronic severe AR with compliant LV, PHT may be borderline (200-500 ms); in acute AR, PHT is nearly always <200 ms
- PHT should be used as a complementary finding, not in isolation
Step 6 - Quantitative Doppler (Volume Flow at Two Sites)
This is the most rigorous quantitative method and uses pulsed Doppler at two intracardiac sites.
Principle: Total stroke volume (TSV) through the aortic valve = forward stroke volume (FSV) + regurgitant volume (RVol). Since FSV = volume crossing the mitral valve (assuming no MR), the difference = RVol.
Formulas
| Parameter | Formula |
|---|---|
| Total SV (TSV) | CSA_LVOT × VTI_LVOT |
| Forward SV (FSV) | CSA_MA × VTI_MA |
| Regurgitant Volume (RVol) | TSV - FSV |
| Regurgitant Fraction (RF) | (RVol / TSV) × 100% |
| Regurgitant Orifice Area (ROA) | RVol / VTI_AR |
Where:
- CSA = π × (diameter/2)² (cross-sectional area, assuming circular geometry)
- LVOT diameter measured in PLAX in mid-systole; VTI measured by pulsed Doppler in apical view
- Mitral annulus (MA) diameter measured in apical 4-chamber (PLAX); VTI measured at same level
- VTI_AR = velocity-time integral of the CW Doppler AR signal (the diastolic retrograde signal)
Severity Thresholds
| Parameter | Mild | Moderate | Severe |
|---|---|---|---|
| Regurgitant Volume (RVol) | < 30 mL | 30-59 mL | ≥ 60 mL |
| Regurgitant Fraction (RF) | < 30% | 30-49% | ≥ 50% |
| ROA / EROA | < 0.10 cm² | 0.10-0.29 cm² | ≥ 0.30 cm² |
Step 7 - PISA (Proximal Isovelocity Surface Area) Method
An alternative quantitative method using flow convergence on color Doppler:
- Regurgitant flow rate = PISA × aliasing velocity
- PISA = 2πr² (hemisphere assumption)
- Shift baseline toward the AR jet direction to an aliasing velocity of 30-40 cm/s for best measurement
- Limitations: poor feasibility with heavy valve calcification; large errors from small mismeasurements (errors are squared); less valid for multiple jets
5. Summary Severity Criteria Table
| Parameter | Mild | Moderate | Severe |
|---|---|---|---|
| Jet width/LVOT ratio | < 25% | 25-64% | ≥ 65% |
| Vena contracta width | < 0.3 cm | 0.3-0.6 cm | > 0.6 cm |
| Holodiastolic flow reversal | Absent | Descending thoracic aorta | Proximal abdominal aorta |
| End-diastolic reversal velocity | - | - | > 20 cm/s |
| CW signal density | Faint | Intermediate | Dense (= antegrade) |
| Pressure half-time | > 500 ms | 200-500 ms | < 200 ms |
| Regurgitant Volume | < 30 mL | 30-59 mL | ≥ 60 mL |
| Regurgitant Fraction | < 30% | 30-49% | ≥ 50% |
| ROA/EROA | < 0.10 cm² | 0.10-0.29 cm² | ≥ 0.30 cm² |
Grading approach:
- If most parameters are concordant → assign grade
- If discordant → label as indeterminate and use clinical context, CMR, or repeat echo
- Qualitative signs alone are adequate for acute AR because quantitative methods are not accurate when the LV is non-dilated (normal-sized)
6. Acute vs. Chronic AR - Echo Differences
| Feature | Chronic AR | Acute AR |
|---|---|---|
| LV size | Markedly dilated (eccentric hypertrophy) | Normal size |
| LVEF | Normal until late; drops below 50% late | Normal EF (deceptively preserved) |
| LV filling pressure | Normal in compensated state | Severely elevated (high LVEDP) |
| PHT | ≥200 ms typically | < 200 ms (very steep slope) |
| Aortic flow reversal | Proximal abdominal aorta | Proximal abdominal aorta (holodiastolic) |
| Mitral valve | Anterior leaflet flutter | Premature mitral valve closure (pathognomonic - LVEDP > LAP) |
| CW deceleration | Gentler slope | Very steep, almost vertical slope |
| Etiology clues | Bicuspid valve, calcification, rheumatic changes | Dissection flap, vegetations, flail leaflet |
7. LV Response - Dimensions and Function
Once severe AR is established, serial measurement of LV dimensions and function is essential for surgical timing.
Key Measurements
| Parameter | Threshold for Intervention | Method |
|---|---|---|
| LV end-systolic diameter (LVESD) | > 50 mm (or > 25 mm/m² BSA) | M-mode or 2D in PLAX |
| LV end-diastolic diameter (LVEDD) | > 65 mm | M-mode or 2D |
| LV ejection fraction (LVEF) | < 50% | Biplane Simpson's; 3D preferred |
| Global longitudinal strain (GLS) | < -17 to -18% (subclinical dysfunction) | Speckle tracking; may detect dysfunction before LVEF drops |
Important concepts:
- In AR, LVEF is an unreliable marker of myocardial contractility because preload is elevated (Frank-Starling effect artificially maintains EF)
- Subclinical myocardial dysfunction can occur with normal LVEF - GLS is more sensitive
- An irreversible decrease in systolic function can occur without symptoms - this is why serial echo is mandatory
- 3D volumetric assessment is preferred over linear measurements because it avoids apical foreshortening
8. Aortic Root and Ascending Aorta Measurement
Measurement is mandatory because:
- Aortic root dilation may be the primary cause of AR (functional AR from non-coaptation)
- Dilation may coexist even when valve leaflets are the primary culprit
Measurement Sites (PLAX, standard)
- Annulus
- Sinuses of Valsalva
- Sinotubular junction (STJ)
- Proximal ascending aorta
Intervention Thresholds (diameter)
| Condition | Threshold |
|---|---|
| Isolated aortic dilation | > 55 mm |
| Bicuspid aortic valve | > 50 mm |
| Marfan syndrome / connective tissue disease | > 45-50 mm |
| Loeys-Dietz or familial aortic aneurysm | > 45 mm |
9. Disease Staging (ASE/ACC/AHA Framework)
| Stage | Definition | Valve Hemodynamics |
|---|---|---|
| A | At risk | Normal valve but at risk (bicuspid, dilated aorta) - no AR |
| B | Progressive AR | Mild to moderate AR; no LV dilation |
| C1 | Severe asymptomatic, compensated | Severe AR; LVEF ≥ 50%, LVESD ≤ 50 mm |
| C2 | Severe asymptomatic, decompensated | Severe AR; LVEF < 50% or LVESD > 50 mm |
| D | Severe symptomatic | Severe AR with symptoms (dyspnea, angina, HF) |
10. Color Flow Doppler - AR Jet Characteristics
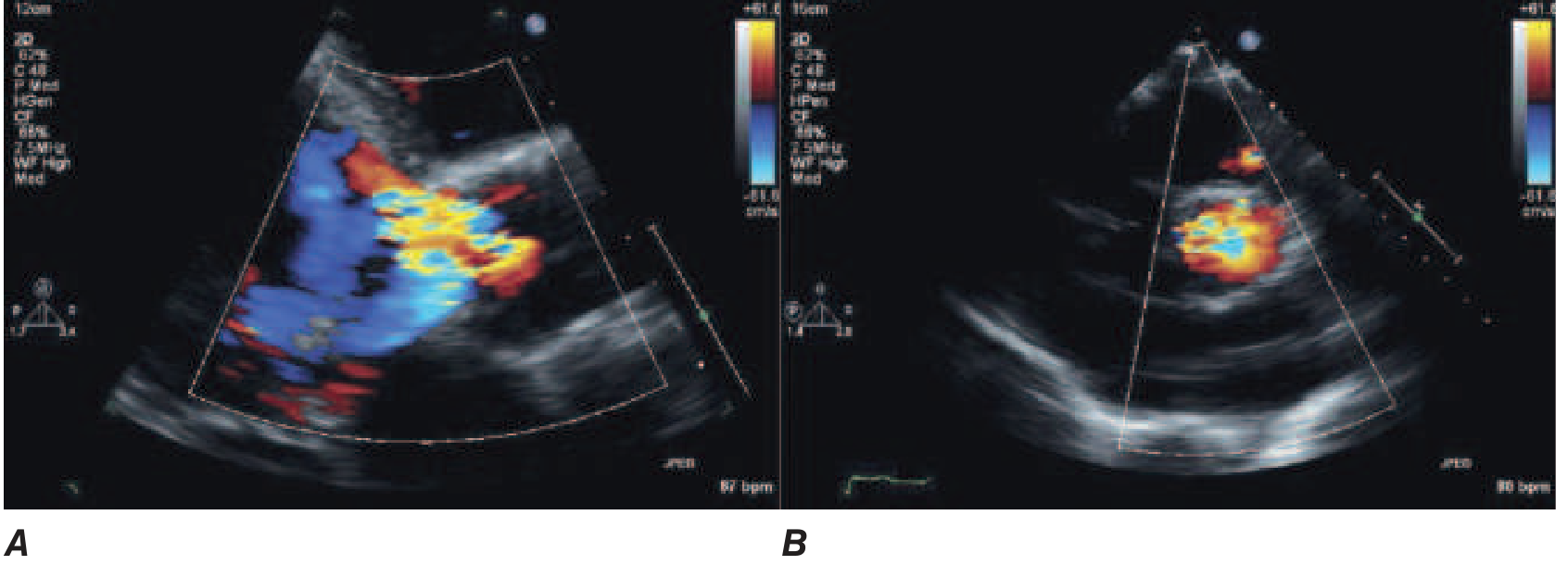
- Central jets: originate at the center of the valve (aortic root dilation, Marfan)
- Eccentric jets: originate from the margin of one leaflet (bicuspid valve, leaflet prolapse, endocarditis)
- Eccentric jets underestimate severity by jet area/width methods → vena contracta is the preferred measure
11. TEE (Transesophageal Echocardiography)
Indications in AR:
- Poor TTE windows
- Pre-operative valve repair planning
- Intraoperative guidance (valve repair or replacement)
- Suspected endocarditis (abscess, perforation)
- Aortic dissection (confirm leaflet involvement)
TEE advantages: superior resolution for leaflet anatomy, direct measurement of the regurgitant orifice, 3D vena contracta area measurement
12. Stress Echocardiography
- Used when symptoms are out of proportion to the degree of AR on resting echo
- Exercise echo can unmask reduced exercise capacity or reveal LV dysfunction not apparent at rest
- Useful in asymptomatic patients where the decision to operate is borderline
13. Follow-Up Echo Intervals (Surveillance)
| Severity | Follow-Up Interval |
|---|---|
| Mild AR | Every 3-5 years |
| Moderate AR | Every 1-2 years |
| Severe AR, asymptomatic, compensated (Stage C1) | Every 6-12 months |
| Severe AR with borderline LV (C2 approaching threshold) | Every 3-6 months |
14. Post-TAVR / Post-Surgical Echo
For paravalvular or central AR after TAVI:
- Assessed immediately post-procedure and on follow-up
- Severity graded using same vena contracta, flow reversal, and quantitative criteria
- Circumferential extent of paravalvular leak on short-axis view: < 10% mild; 10-20% moderate; > 20% severe
Key Points Summary
- Screening = color flow PLAX + CW Doppler (apical). Weak CW signal = no significant AR.
- Vena contracta > 0.6 cm = severe AR (most reproducible single measure).
- Holodiastolic flow reversal in proximal abdominal aorta = severe AR (most specific qualitative sign).
- PHT < 200 ms = severe AR (but heavily dependent on LV compliance and beam alignment).
- Quantitative criteria for severe: RVol ≥ 60 mL, RF ≥ 50%, ROA ≥ 0.30 cm².
- Premature mitral valve closure = pathognomonic of acute severe AR (LVEDP > LAP).
- Anterior mitral leaflet flutter = indirect sign of AR jet impingement on MV.
- LV function thresholds for surgery: LVEF < 50%, LVESD > 50 mm, LVEDD > 65 mm.
- Always measure aortic root at all four standard levels - dilation may be the primary etiology.
- Multi-parameter, integrated approach is mandatory - no single criterion is sufficient.
Textbook of Clinical Echocardiography (Otto), 6e, Chapter 12 | Fuster & Hurst's The Heart, 15e, Chapter 29 | Harrison's Principles of Internal Medicine, 22e, Chapter 248
This is a shared conversation. Sign in to Orris to start your own chat.