40 years female with no known comorbidity came with history of generalized weekness for 8-9 days no history of truma and fever on examination power in all 4 limbs 4/5 sensation intact deep tendon reflexes intact what differential diagnosis and management
generalized weakness differential diagnosis neuromuscular
Clinical Analysis: 40-Year-Old Female, Generalized Weakness x 8-9 Days
Key Features to Anchor the Differentials
| Feature | Significance |
|---|---|
| Subacute onset (8-9 days) | Narrows to inflammatory, metabolic, or early neuromuscular causes |
| Power 4/5 all 4 limbs (symmetrical) | Mild but objective weakness; likely generalized (not focal CNS) |
| Sensation intact | Argues against pure sensory neuropathy; does not fully exclude GBS early |
| Deep tendon reflexes intact | Important - argues strongly AGAINST GBS (which requires areflexia/hyporeflexia); favors myopathy or NMJ disease |
| No fever | Reduces likelihood of infectious myositis/encephalitis |
| No trauma | Excludes structural/spinal cord injury |
| No known comorbidities | Metabolic causes still possible; may be first presentation of autoimmune disease |
Differential Diagnoses
Priority 1 - Most Likely Given Intact Reflexes
- Classic presentation: subacute proximal symmetrical weakness over weeks; female predominance; age 40 fits
- DTRs intact or mildly diminished, sensation normal - matches perfectly
- Associated with elevated CK, aldolase, LDH
- May be paraneoplastic in this age group; associated with breast, ovarian, GI cancers
- Goldman-Cecil Medicine notes: "Most patients present with subacute proximal weakness of the arms and legs progressing over months, though these diseases may present acutely"
- Check for skin changes (heliotrope rash, Gottron's papules) that would confirm dermatomyositis
- Acute/subacute generalized weakness with intact reflexes and intact sensation is a hallmark
- Thyrotoxic periodic paralysis is particularly relevant for a 40-year-old woman
- Other causes: diuretic use, vomiting/diarrhea, hyperaldosteronism (Conn's syndrome), renal tubular acidosis
- Harrison's 22E: Onset over minutes to hours may result from "electrolyte disturbances, certain inborn errors of muscle energy metabolism, toxins, and periodic paralyses"
- Thyrotoxic myopathy: proximal weakness, may precede other signs of hyperthyroidism; common in women
- Hypothyroid myopathy: proximal weakness, cramps, stiffness, elevated CK
- Robbins Pathology: "Thyrotoxic myopathy presents most commonly as an acute or chronic proximal muscle weakness that may precede other signs of hyperthyroidism"
- TSH is a mandatory first test
- Autoimmune NMJ disease; peak incidence in women 20-40 years
- Classically fatigable (worse with activity, better with rest), ocular involvement (ptosis, diplopia)
- Intact sensation and reflexes match; ask specifically about bulbar symptoms and diurnal variation
- Tintinalli's EM: "Consider MG in any patient with ocular disturbances or proximal limb muscle weakness not associated with systemic causes"
Priority 2 - Must Rule Out
- Typically presents with areflexia - this patient has intact DTRs, which argues against classical GBS
- However, in the very early phase (day 1-3), reflexes may not yet be lost
- At 8-9 days with intact reflexes, GBS becomes less likely but variants (pharyngeal-cervical-brachial) may have preserved limb reflexes
- Bradley & Daroff's Neurology: "Features required for diagnosis include progressive weakness of both legs and arms + areflexia or hyporeflexia"
- Still merit CSF and nerve conduction study if clinical suspicion remains
- Can cause quadriparesis; would expect sensory level and bladder/bowel dysfunction
- Sensation intact reduces likelihood but does not fully exclude central cord or early cord pathology
- MRI spine if red flags develop
- Proximal limb weakness that transiently improves with repeated use (opposite of MG)
- Associated with occult malignancy (small cell lung cancer); relevant for thorough workup
- Reflexes may be reduced or absent - if DTRs are truly normal, LEMS is less likely
- Generalized weakness, fatigue; may have no other obvious symptoms early
- Can cause hyponatremia and hyperkalemia
- Diagnosis of exclusion; important to rule out all organic causes first
- Harrison's 22E: "A patient with generalized fatigability without objective weakness may have myalgic encephalomyelitis/chronic fatigue syndrome"
Immediate Investigations
Bedside / Urgent
- Serum electrolytes (Na, K, Mg, Ca, phosphate) - rule out hypokalemia
- Blood glucose - rule out hypoglycemia
- Serum TSH + free T4 - thyroid myopathy is common and treatable
- Serum CK (creatine kinase) + aldolase, LDH - elevated in inflammatory myopathy
- CBC + ESR + CRP - inflammatory workup
- LFT, RFT - baseline and metabolic causes
Specific Workup Based on Clinical Suspicion
| Suspected Diagnosis | Key Tests |
|---|---|
| Polymyositis/Dermatomyositis | CK, aldolase, ANA, anti-Jo-1, anti-Mi-2, EMG, muscle biopsy |
| Myasthenia Gravis | Tensilon (edrophonium) test, anti-AChR antibody, anti-MuSK, repetitive nerve stimulation, CT chest (thymoma) |
| GBS | CSF (albuminocytological dissociation), nerve conduction study |
| Thyroid Myopathy | TSH, free T4, free T3 |
| Hypokalemic periodic paralysis | Serum potassium during episode, ECG |
| Adrenal insufficiency | Morning cortisol, ACTH stimulation test |
| LEMS | Voltage-gated calcium channel antibodies, CT chest |
| Spinal cord | MRI spine with contrast |
Management Approach
Step 1 - Immediate Stabilization
- Respiratory assessment: Check respiratory muscle function (FVC at bedside). Neuromuscular causes can progress to respiratory failure. Admit for monitoring if any bulbar or respiratory compromise.
- Monitoring: Pulse oximetry, serial neurological exam every 4-6 hours to assess for progression
Step 2 - Treat Reversible Causes First
| Finding | Immediate Treatment |
|---|---|
| Hypokalemia | Oral/IV potassium replacement; investigate underlying cause |
| Hypothyroidism | Levothyroxine |
| Hyperthyroidism | Beta-blockers + antithyroid drugs (carbimazole/PTU) |
| Hypercalcemia | IV fluids, bisphosphonates |
Step 3 - Condition-Specific Management
- High-dose prednisolone: 1 mg/kg/day orally
- Steroid-sparing agents: azathioprine or methotrexate for long-term maintenance
- Physical therapy / rehabilitation
- Pyridostigmine (acetylcholinesterase inhibitor) - first-line symptomatic treatment
- Oral prednisolone for autoimmune control
- Plasmapheresis or IVIG for myasthenic crisis or rapid deterioration
- Thymectomy if thymoma is found
- Admit to ICU if FVC <20 mL/kg or rapid progression
- IVIG 0.4 g/kg/day x 5 days OR plasmapheresis
- No role for corticosteroids in GBS
- Serial FVC monitoring; intubate if respiratory failure
Step 4 - Specialist Referral
- Neurology referral for all patients pending EMG/nerve conduction study
- Rheumatology if inflammatory myopathy confirmed
- Screen for occult malignancy in confirmed dermatomyositis (mammography, CT abdomen-pelvis, CA-125, CEA) given age and association
Red Flags Requiring Immediate ICU Admission
- FVC <1.5 L or rapidly declining
- Bulbar symptoms (dysphagia, dysphonia, nasal regurgitation)
- Autonomic instability (blood pressure lability, arrhythmia)
- Rapid progression of weakness
- Inability to lift head off pillow
Summary Priority Order
Sources: Harrison's Principles of Internal Medicine 22E | Bradley & Daroff's Neurology in Clinical Practice | Goldman-Cecil Medicine | Tintinalli's Emergency Medicine
Create a diagnostic flowchart for subacute generalized weakness with intact reflexes
A detailed clinical diagnostic flowchart for "Subacute Generalized Weakness with Intact Deep Tendon Reflexes". Clean medical/clinical style with white background, organized top to bottom with color-coded boxes and arrows. Start at the top with a green box: "Subacute Generalized Weakness (days–weeks) + Intact DTRs + Intact Sensation + No Trauma/Fever" Arrow down to a blue decision diamond: "Check Serum Electrolytes, TSH, CK, CBC, BMP" Branch into 4 paths from left to right: LEFT PATH - orange box: "Electrolyte Abnormality (↓K+, ↓Mg, ↓Ca, ↓PO4)" → arrow down to "Metabolic Myopathy / Periodic Paralysis" → treatment box: "Correct electrolyte deficit; investigate cause (RTA, diuretics, thyrotoxicosis)" LEFT-CENTER PATH - orange box: "Abnormal TSH / Thyroid Function" → arrow down to "Thyroid Myopathy: Hypo- or Hyperthyroid" → treatment box: "Levothyroxine (hypothyroid) OR Carbimazole + Beta-blocker (hyperthyroid)" RIGHT-CENTER PATH - orange box: "Elevated CK / Aldolase (>5x normal)" → arrow down to blue decision diamond: "EMG + Muscle Biopsy + Myositis Antibodies (ANA, Anti-Jo-1, Anti-Mi-2)" → two branches: left branch red box "Inflammatory Myopathy (Polymyositis/Dermatomyositis)" → "Prednisolone 1mg/kg/day + Azathioprine; Screen for malignancy" and right branch purple box "Inclusion Body Myositis / Necrotizing Myopathy" → "Refer Rheumatology" RIGHT PATH - orange box: "Normal Labs — Fatigable Weakness? Ocular/Bulbar Symptoms?" → two branches: left branch "YES" → blue diamond "Anti-AChR Ab, Anti-MuSK, Repetitive Nerve Stimulation, CT Chest" → red box "Myasthenia Gravis" → "Pyridostigmine + Prednisolone; IVIG if crisis; Thymectomy if thymoma" and right branch "NO" → blue diamond "Nerve Conduction Study + CSF" → two sub-branches: "Demyelination/Axonal pattern" → red box "GBS Variant (check: are reflexes truly intact?)" → "IVIG or Plasmapheresis" and "Normal NCS/CSF" → purple box "Consider: LEMS (VGCC Ab), Addison's (cortisol), Functional" At the bottom, a wide red warning box: "⚠ RED FLAGS — Admit to ICU: FVC <1.5L or declining | Bulbar symptoms | Autonomic instability | Rapid progression" Use color coding: green for entry, blue for decision points/investigations, orange for findings, red for diagnoses needing urgent treatment, purple for less urgent diagnoses, yellow/gold for treatment boxes. All text should be clear, readable, professional medical font. Include a small legend in the bottom corner.
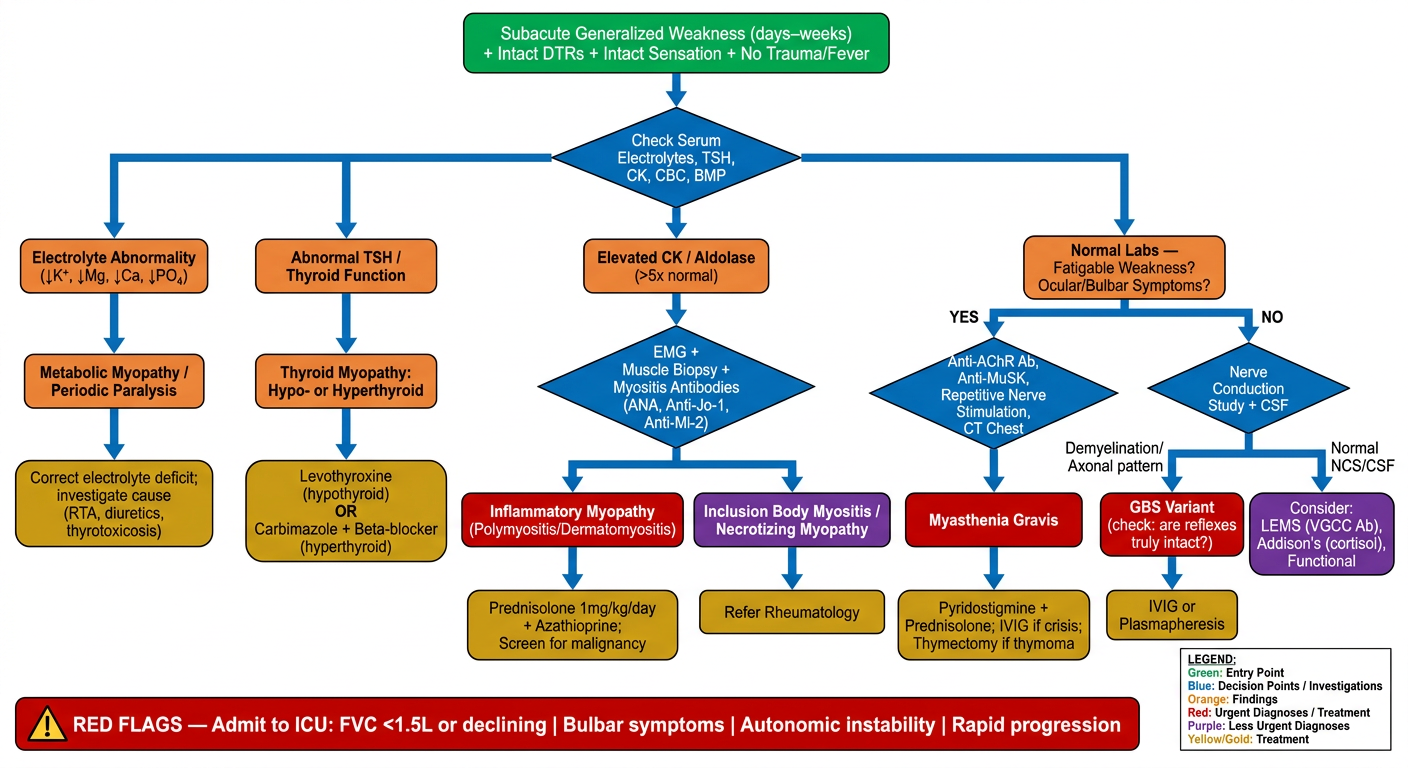
- Electrolyte abnormality - Points to metabolic myopathy or hypokalemic periodic paralysis; treat the underlying cause
- Abnormal thyroid function - Thyroid myopathy (hypo- or hyperthyroid); treat the thyroid disorder
- Elevated CK/aldolase - Triggers EMG + muscle biopsy + myositis antibodies, leading to inflammatory myopathy (polymyositis/dermatomyositis) with malignancy screening, or necrotizing myopathy
- Normal labs + fatigable/ocular/bulbar symptoms - Leads to MG workup (anti-AChR, anti-MuSK, repetitive nerve stimulation, CT chest); if no fatigable pattern, nerve conduction study and CSF to evaluate for GBS variants, LEMS, or adrenal insufficiency