Ropinirole mechanism of action, dose, route, frequency, storage, pharmacokinetics, pharmacodynamics, indication, contraindications, adverse effect, side effect, nursing responsibility for drug presentation
Reading File
Finding Sources
Searching the Web
ropinirole mechanism of action pharmacokinetics pharmacodynamics dose nursing
Reading File
Reading Web Page
https://www.ncbi.nlm.nih.gov/books/NBK554532
Reading File
Reading Web Page
https://prescriberpoint.com/therapies/ropinirole-85971b3
Finding Sources
Loading Image
I now have all the information needed for a thorough drug presentation. Here is the complete reference:
ROPINIROLE - Drug Presentation
Generic Name: Ropinirole
Brand Names: Requip, Requip XL
Drug Class: Non-ergoline dopamine agonist
DEA Schedule: Not a controlled substance
1. MECHANISM OF ACTION
Ropinirole is a non-ergoline dopamine agonist with a high affinity for post-synaptic dopamine receptors in the central and peripheral nervous systems. It acts primarily at dopamine D2 receptors (and to a lesser degree D3 receptors) located in the caudate-putamen (striatum) of the brain.
- These D2 receptors are G-protein-coupled inhibitory neurons located primarily in the striatonigral, mesolimbic, and tuberoinfundibular systems
- Ropinirole binding inhibits adenylyl cyclase and calcium channels, and activates potassium channels
- In Parkinson's disease, it mimics the action of dopamine in the depleted nigrostriatal pathway, maximizing "on" time and minimizing "off" time
- It binds approximately 20x more selectively to D3 than D2 receptors (unlike bromocriptine which has a ratio <2:1)
- In Restless Legs Syndrome (RLS), the precise mechanism is less clear but is also thought to be related to dopamine receptor stimulation
Sources: StatPearls - Ropinirole (NBK554532); Lippincott Illustrated Reviews Pharmacology, p. 528
2. INDICATIONS
- Parkinson's Disease (PD) - both early and advanced stages; can be used as monotherapy or adjunct to levodopa
- Restless Legs Syndrome (RLS) - moderate to severe primary RLS (FDA-approved)
- Off-label: Antidepressant-induced sexual dysfunction; fibromyalgia; periodic limb movement disorder (PLMD)
3. DOSAGE
Parkinson's Disease (Immediate-Release Tablets)
| Week | Dose | Total Daily Dose |
|---|---|---|
| Week 1 | 0.25 mg 3x daily | 0.75 mg |
| Week 2 | 0.5 mg 3x daily | 1.5 mg |
| Week 3 | 0.75 mg 3x daily | 2.25 mg |
| Week 4 | 1 mg 3x daily | 3 mg |
| After Week 4 | Increase by 1.5 mg/day weekly up to 9 mg/day, then up to 3 mg/day weekly | Max: 24 mg/day |
Discontinuation: Taper over 7 days - reduce from TID to BID for 4 days, then once daily for 3 days before stopping.
Restless Legs Syndrome
| Time Period | Dose (once daily, 1-3 hours before bedtime) |
|---|---|
| Days 1-2 | 0.25 mg |
| Days 3-7 | 0.5 mg |
| Week 2 | 1 mg |
| Week 3 | 1.5 mg |
| Week 4 | 2 mg |
| Week 5 | 2.5 mg |
| Week 6 | 3 mg |
| Week 7 | 4 mg (maximum) |
Special Populations:
- Renal impairment (ESRD on hemodialysis): Starting dose 0.25 mg TID for PD; max 18 mg/day. Supplemental doses after dialysis are not required.
- Hepatic impairment: Use with caution; titrate slowly as ropinirole is hepatically metabolized.
- Elderly: Titrate more slowly due to higher risk of hallucinations, nausea, and vomiting.
4. ROUTE OF ADMINISTRATION
- Oral (primary route) - tablets (immediate-release and extended-release)
- Available as: 0.25 mg, 0.5 mg, 1 mg, 2 mg, 3 mg, 4 mg, 5 mg tablets (IR); 2 mg, 4 mg, 6 mg, 8 mg, 12 mg (XL)
5. FREQUENCY
- Parkinson's disease (IR): Three times daily (TID) with meals to reduce nausea
- RLS (IR): Once daily, 1 to 3 hours before bedtime
- Extended-release (XL/ER): Once daily for Parkinson's disease
- Steady-state concentrations are reached within 2 days of dosing
6. STORAGE
- Store at 20°C to 25°C (68°F to 77°F); excursions permitted between 15°C to 30°C (59°F to 86°F) - USP Controlled Room Temperature
- Protect from light and moisture
- Keep container tightly closed after each use
- Keep out of reach of children
7. PHARMACOKINETICS
| Parameter | Value |
|---|---|
| Absorption | Rapid; peak concentration in 1-2 hours |
| Bioavailability | 45-55% (approximately 50% first-pass effect) |
| Volume of Distribution (Vd) | 7.5 L/kg |
| Protein Binding | Low (~40%) |
| Metabolism | Extensive hepatic metabolism via CYP1A2 isoenzyme; major metabolites are pharmacologically inactive |
| Half-life | ~6 hours |
| Elimination | Primarily renal (>88% recovered in urine) as metabolites |
| Kinetics | Linear pharmacokinetics over 1-8 mg TID dosing range |
Drug Interactions (Pharmacokinetic):
- CYP1A2 inhibitors (fluoroquinolones, fluvoxamine, ciprofloxacin): increase ropinirole plasma levels - dose reduction may be needed
- Estrogens: inhibit CYP1A2, may increase ropinirole levels
- CYP1A2 inducers (smoking, omeprazole): decrease ropinirole levels - dose increase may be needed if patient stops smoking
Source: Lippincott Illustrated Reviews Pharmacology, p. 529; Clinical PK of ropinirole (PMID 11069211)
8. PHARMACODYNAMICS
- Stimulates dopamine D2/D3 receptors in the striatum, reproducing the inhibitory effects of endogenous dopamine
- Suppresses serum prolactin concentrations (at doses ≥0.8 mg)
- Causes orthostatic hypotension via D2-mediated blunting of the noradrenergic response to standing, leading to decreased peripheral vascular resistance
- No effect on ECG wave form or rhythm at therapeutic doses
- Compared to levodopa: fewer dyskinesias (motor complications); at 5 years, ropinirole caused motor complications in only 20% of patients vs. 45% with levodopa
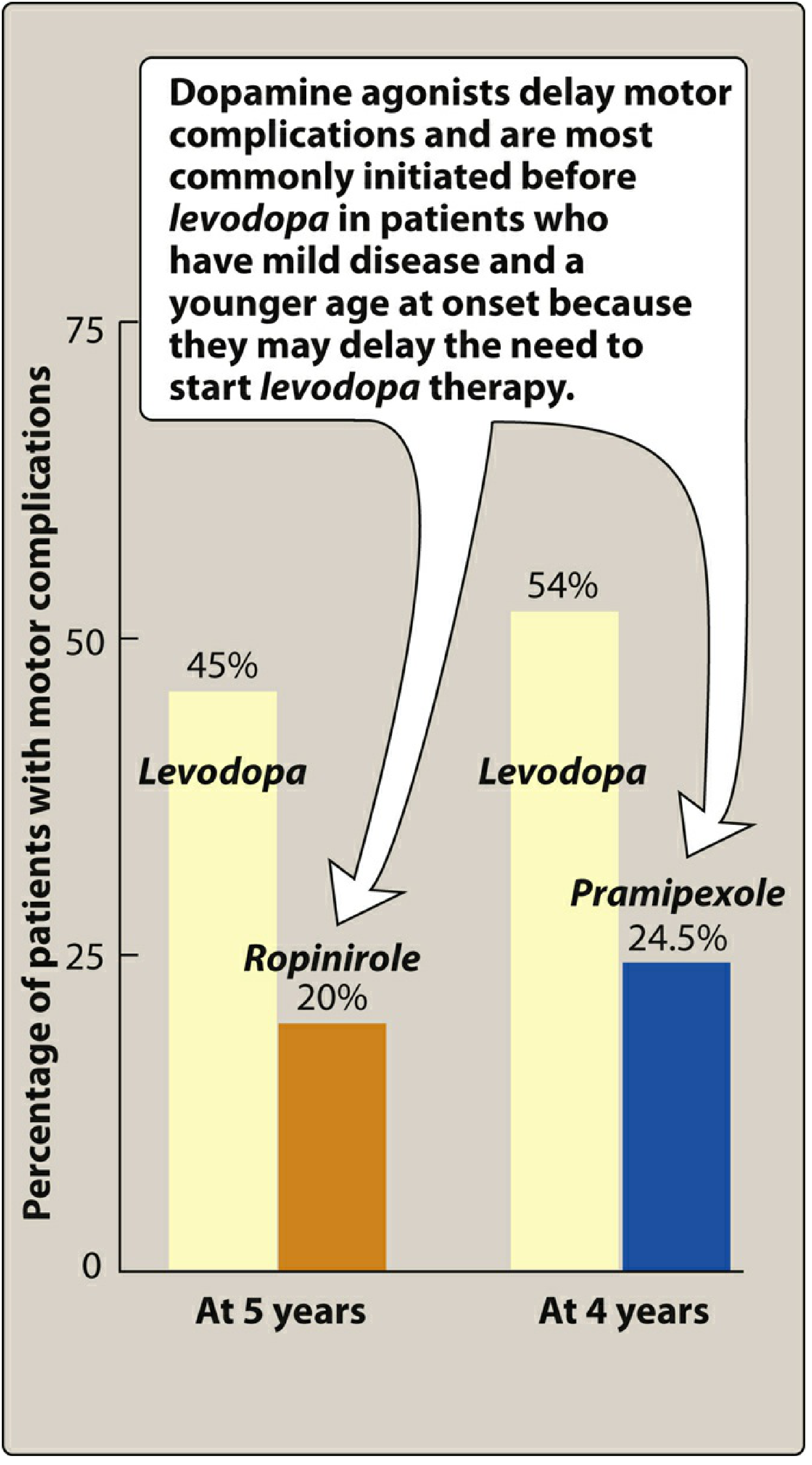
Source: Lippincott Illustrated Reviews Pharmacology, Fig. 15.11
9. CONTRAINDICATIONS
Absolute Contraindications:
- Hypersensitivity to ropinirole or any excipient (rash, pruritus, urticaria, angioedema, anaphylaxis)
Warnings / Relative Contraindications (use with extreme caution):
- Alcohol abuse - increased CNS depression risk
- Severe hepatic failure - impaired metabolism
- History of psychosis or schizophrenia - may worsen hallucinations/psychosis
- Severe cardiovascular disease - risk of orthostatic hypotension and syncope
- Pregnancy (Category C) - use only if benefit outweighs risk
- Breastfeeding - ropinirole suppresses prolactin and may impair lactation; an alternative drug is preferred for nursing mothers
- Pediatric patients - safety and efficacy not established
10. ADVERSE EFFECTS / SIDE EFFECTS
Common (>10%)
- Nausea (most frequent)
- Vomiting, dyspepsia, abdominal pain
- Dizziness / somnolence
- Fatigue, asthenic conditions (weakness, malaise)
- Orthostatic hypotension - especially during dose escalation
Nervous System
- Hallucinations (more common in elderly)
- Confusion, dyskinesia (less frequent than levodopa)
- Sudden-onset sleep attacks - "sleep attacks" without warning; major safety concern especially while driving
- Insomnia
Cardiovascular
- Orthostatic hypotension, syncope
- Bradycardia (transient sinus arrest reported in healthy volunteers in clinical trials)
- Leg edema
Impulse Control Disorders (important - often underreported)
- Pathological gambling
- Hypersexuality / increased libido
- Compulsive shopping or eating (binge eating)
- Mechanism: thought to be stimulation of dopamine D3 receptors; patients may not report due to embarrassment - clinicians must proactively ask
Other
- Viral infections
- Augmentation (in RLS - worsening of symptoms)
- Manic symptoms in susceptible patients
- Withdrawal syndrome if abruptly stopped (confusion, fever, rhabdomyolysis - similar to neuroleptic malignant syndrome)
11. NURSING RESPONSIBILITIES
Before Administration (Pre-Drug)
- Assess baseline vital signs - especially blood pressure (sitting and standing) to establish baseline for orthostatic hypotension monitoring
- Review medical history - confirm no hypersensitivity, assess for psychiatric history, liver disease, renal function
- Medication reconciliation - check for CYP1A2 inhibitors (fluoroquinolones, fluvoxamine), estrogens, dopamine antagonists (metoclopramide, antipsychotics) that can block ropinirole's effect
- Assess for smoking status - smoking induces CYP1A2 and decreases ropinirole levels; changes in smoking habit require dose adjustment
- Baseline neurological assessment - document motor function, sleep patterns, mood, and cognitive status
- Pregnancy/lactation screening - assess reproductive status; educate that ropinirole can suppress prolactin and impair milk production
During Administration
- Administer with food or milk to minimize nausea - the most common adverse effect
- For RLS: Give dose 1-3 hours before bedtime only
- Follow titration schedule strictly - do not increase dose faster than prescribed; rapid titration increases orthostatic hypotension risk
- Never abruptly discontinue - taper per schedule to avoid withdrawal (NMS-like syndrome)
Monitoring / Ongoing Assessment
- Monitor blood pressure in lying and standing positions - watch for orthostatic hypotension (fall in SBP >20 mmHg on standing); instruct patient to change positions slowly
- Monitor for sleepiness and sleep attacks - warn patients not to drive or operate heavy machinery until they know how the drug affects them; ask about sudden-onset sleep without warning
- Screen for impulse control disorders at every visit - ask directly about gambling, hypersexuality, binge eating; patients are often embarrassed and will not volunteer this information
- Hallucinations and psychiatric changes - especially in elderly; report to physician immediately
- Monitor for dyskinesia when used with levodopa - may require levodopa dose reduction
- Liver function monitoring - particularly in patients with hepatic impairment
Patient and Family Education
- Orthostatic precautions: Rise slowly from lying to sitting to standing; sit at the edge of the bed for 1-2 minutes before standing; use grab bars; call for assistance if dizzy
- No abrupt discontinuation - emphasize that the drug must be tapered; missing doses or stopping suddenly can cause a dangerous withdrawal reaction
- Avoid alcohol - potentiates CNS depression and hypotension
- Report compulsive behaviors immediately (gambling, sexual urges, binge eating) - these are drug side effects and the dose may need to be adjusted
- Sleep safety - do not drive or operate machinery if experiencing excessive daytime sleepiness or sudden sleep attacks
- Smoking: Inform physician if starting or stopping smoking (affects drug metabolism)
- Medication interactions - avoid antipsychotics (haloperidol, metoclopramide) as they are dopamine antagonists that can block ropinirole's therapeutic effect
- Storage education: Store at room temperature, protect from light and moisture, keep tightly closed
- Missed dose (PD): If almost time for next dose, skip missed dose - do not double up
QUICK REFERENCE SUMMARY TABLE
| Parameter | Details |
|---|---|
| Class | Non-ergoline dopamine agonist |
| Receptor | D2 > D3 |
| Route | Oral (tablet) |
| Frequency | TID (PD-IR), OD (RLS, PD-XR) |
| Starting dose - PD | 0.25 mg TID |
| Max dose - PD | 24 mg/day |
| Starting dose - RLS | 0.25 mg OD (1-3 h before bed) |
| Max dose - RLS | 4 mg/day |
| Half-life | ~6 hours |
| Metabolism | Hepatic - CYP1A2 |
| Storage | 20-25°C, protect from light & moisture |
| Key ADRs | Nausea, orthostatic hypotension, sleep attacks, hallucinations, impulse control disorders |
| Key CI | Hypersensitivity, severe hepatic failure, breastfeeding |
Sources: StatPearls - Ropinirole; Lippincott Illustrated Reviews Pharmacology 7th Ed., p. 528-529; Katzung's Basic & Clinical Pharmacology 16th Ed., p. 795; Kaplan & Sadock's Comprehensive Textbook of Psychiatry; Clinical PK of ropinirole (PMID 11069211)
This is a shared conversation. Sign in to Orris to start your own chat.