Leoprolide
Reading File
Finding Sources
Searching the Web
leuprolide mechanism of action clinical uses pharmacology
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information from authoritative sources. Here is a complete overview of Leuprolide (you may have seen it spelled "Leoprolide" - the correct name is Leuprolide):
Leuprolide (Brand names: Lupron, Eligard)
Drug Class
Synthetic GnRH (Gonadotropin-Releasing Hormone) agonist analogue - a member of the GnRH congener family alongside goserelin, nafarelin, triptorelin, and histrelin.
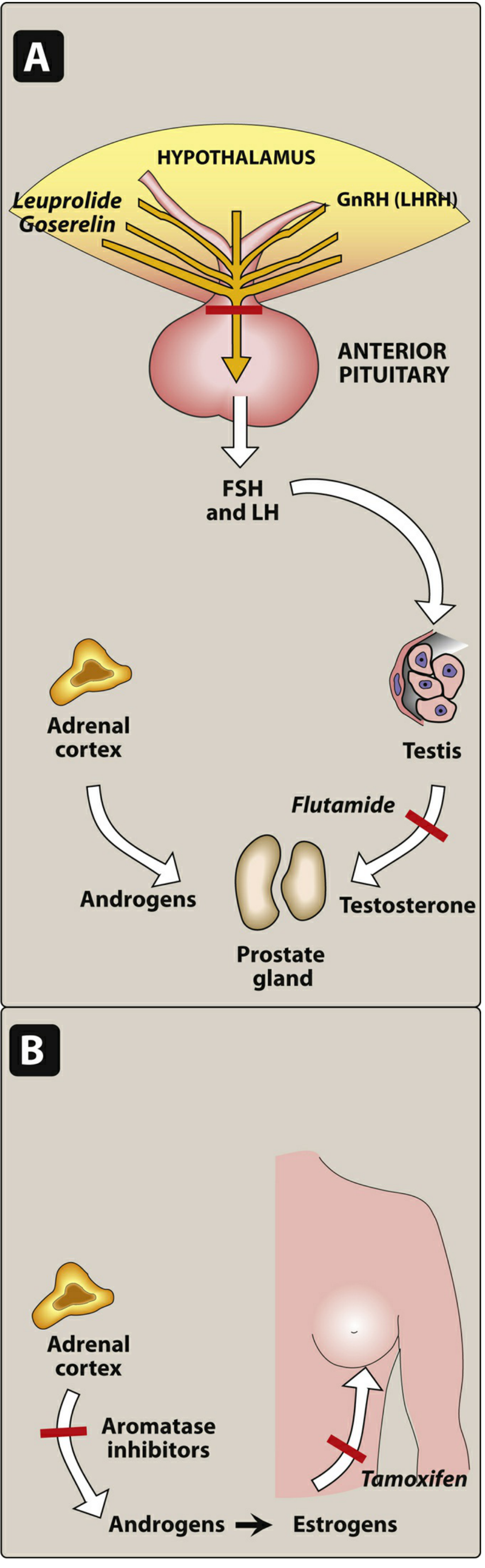
Mechanism of Action
Leuprolide is a synthetic peptide analogue of GnRH with two key structural modifications:
- A substitution at position 6 that protects against proteolysis
- A substitution at the carboxyl terminus that improves receptor-binding affinity
These modifications give it enhanced potency and prolonged duration of action compared to native GnRH.
The biphasic effect:
- Phase 1 (initial - first 1-2 weeks): Leuprolide binds and continuously stimulates GnRH receptors in the anterior pituitary → transient surge in LH and FSH → transient rise in testosterone (males) or estrogen (females). This is called the "flare" effect.
- Phase 2 (sustained - after ~2-4 weeks): Continuous receptor occupancy leads to receptor downregulation and desensitization → marked suppression of LH and FSH secretion → fall in testosterone/estrogen to castration levels ("medical castration").
This is the paradox of leuprolide: a GnRH agonist ultimately produces profound gonadotropin suppression through receptor desensitization.
FDA-Approved Clinical Uses
| Indication | Notes |
|---|---|
| Advanced prostate cancer | Medical castration; equivalent in efficacy to bilateral orchiectomy |
| Endometriosis | Reduces estrogen-dependent lesions and pelvic pain |
| Uterine fibroids (leiomyomata) | Preoperative reduction in fibroid size |
| Central (GnRH-dependent) precocious puberty | Arrests premature sexual maturation with minimal side effects |
| Assisted reproduction | Prevents premature LH surge during ovarian stimulation |
Diagnostic use: The depot form (3.75 mg SC) is used to differentiate GnRH-dependent from GnRH-independent precocious puberty. A plasma LH > 6.6 mIU/mL at 2 hours is diagnostic of central (GnRH-dependent) disease. In hypothalamic disease, the intact pituitary responds to leuprolide; in pituitary disease, it does not.
Formulations and Dosing
| Route | Formulation | Dose |
|---|---|---|
| SC injection | Daily | 1 mg/day |
| SC depot | Monthly | 7.5 mg/month |
| SC depot | 3-month | 22.5 mg q3 months |
| SC depot | 4-month | 30 mg q4 months |
| SC depot | 6-month | 45 mg q6 months |
| IM depot | Monthly | 3.75 mg/month |
| IM depot | 3-month | 11.25 mg q3 months |
For endometriosis, the 3.75 mg or 11.25 mg formulations are co-packaged with norethindrone 5 mg/day (oral progestin) to minimize hypoestrogenic bone loss.
Pediatric (central precocious puberty): 0.2-0.3 mg/kg IM (monthly); 11.25-30 mg IM (3 months); 45 mg SC (6 months).
Adverse Effects
Tumor "Flare" (Critical - first 1-2 weeks)
- The initial testosterone surge can worsen symptoms in prostate cancer patients with bone metastases - spinal cord compression, increased bone pain, urinary obstruction
- Prevention: Pre-treat with an antiandrogen (flutamide, bicalutamide, or nilutamide) for 1-2 weeks before starting leuprolide in patients with significant metastatic disease
Hypogonadal Effects (both sexes)
- Hot flashes
- Sexual dysfunction (reduced libido, erectile dysfunction in males)
- Decreased bone mineral density (osteoporosis with long-term use)
- Vaginal dryness / atrophic changes (females)
- Weight gain
- Fatigue and loss of muscle mass
Metabolic Effects (long-term ADT in prostate cancer)
- Increased serum cholesterol
- Increased blood pressure
- Increased risk of major adverse cardiovascular events (MACE) - notably, the cumulative incidence of MACE is approximately 50% higher with leuprolide compared to the GnRH antagonist relugolix, per Goldman-Cecil Medicine
Other
- Injection site reactions
- Gynecomastia (males)
Key Comparison: GnRH Agonists vs. Antagonists
| Feature | Leuprolide (GnRH agonist) | Degarelix/Relugolix (GnRH antagonist) |
|---|---|---|
| Mechanism | Receptor desensitization after initial stimulation | Direct receptor blockade |
| Initial testosterone surge (flare) | Yes - requires antiandrogen cover | No |
| Speed to castration | ~30 days | Faster (days) |
| PSA suppression | Slower | More rapid |
| Cardiovascular risk | Higher (vs. relugolix) | Lower (relugolix) |
Pharmacokinetics
- Bioavailability of intranasal formulations is low (~4%), while parenteral formulations (SC/IM) have much higher bioavailability
- Multiple depot formulations allow for monthly to biannual dosing, improving compliance
- The GnRH agonists as a class are resistant to proteolytic degradation due to the D-amino acid at position 6
Sources:
- Goodman & Gilman's Pharmacological Basis of Therapeutics, Table 46-3 and Ch. 46
- Lippincott Illustrated Reviews: Pharmacology, Ch. 37 (GnRH agonists, Figure 37.27)
- Goldman-Cecil Medicine, Androgen Deprivation Therapy section
This is a shared conversation. Sign in to Orris to start your own chat.