58 year female , osteoporosis with intertrochanteric fracture
intertrochanteric fracture management elderly
intertrochanteric fracture osteoporosis management 2024 2025 guidelines surgical treatment
Intertrochanteric Fracture in a 58-Year-Old Female with Osteoporosis
Overview
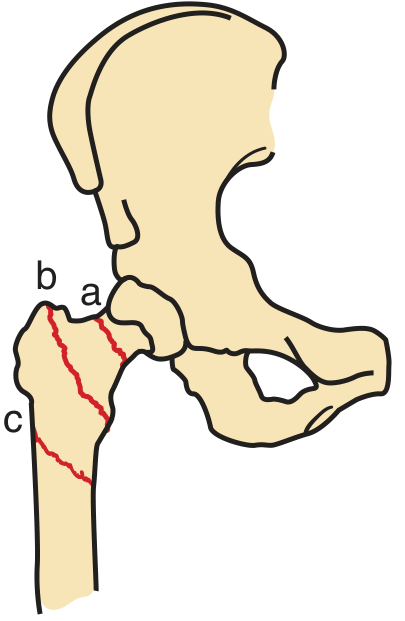
Fracture Sites - Proximal Femur Anatomy
Clinical Presentation
- Markedly shortened and externally rotated lower limb
- Severe pain on any hip movement
- Usually follows low-energy trauma: tripping over a carpet, step, or a slip and fall with direct impact on the trochanteric region
- At 58 years old with osteoporosis, even minimal trauma can cause a complete fracture - in some cases the fracture itself causes the fall ("fracture before the fall")
Imaging
Plain Radiography (First-line)
- AP pelvis (both hips) + lateral hip view
- AP pelvis: include contralateral hip for comparison of reduction and neck-shaft angle
- May add 10° internal rotation view if fracture not clearly seen
Comminuted Intertrochanteric Fracture (X-ray)

When Plain X-ray Is Negative
- ~1% of fractures are initially occult on radiograph
- If clinical suspicion persists and weight-bearing limited at 24 hours: MRI is the gold standard (sensitive and specific)
- If MRI unavailable: CT without contrast is a practical alternative
- Patients with isolated greater trochanteric fractures on plain radiograph frequently have intertrochanteric extension on MRI - this changes management
Classification: OTA/AO System (Rockwood & Green, 10th ed. 2025)
| Type | Description | Stability | Preferred Implant |
|---|---|---|---|
| 31.A1 | Simple two-part fracture, intact lateral wall, fracture line through trochanters | Relatively stable | Sliding Hip Screw (DHS) |
| 31.A2 | Comminuted, intact lateral wall, lesser trochanter detached, 3-4 fragments | Less stable | Cephalomedullary nail (IMN) |
| 31.A3 | Reverse oblique or horizontal, lateral wall disrupted/unstable | Most unstable | Cephalomedullary nail (IMN) - mandatory |
Note: The further AO subdivisions (A1.1, A1.2, etc.) have unacceptable inter-observer variation and are NOT clinically useful - Rockwood & Green, 2025
Management
Surgical vs. Non-surgical Decision
- Surgery is the standard of care for ambulatory patients
- Non-operative treatment is reserved for: truly non-ambulatory patients (e.g., nursing home-bound), patients with severe comorbidities making surgery prohibitive, or personal refusal
- Even a non-displaced ITF is at high risk for displacement with minimal movement (rolling in bed), so non-operative management carries significant risks
Timing of Surgery
- Operate as soon as medically optimized, ideally within 24 hours
- British Hip Fracture Database data: 30-day mortality increases 10% for every 24-hour delay
- The HIP ATTACK trial showed no mortality benefit to ultra-early surgery (median 6 hrs) vs. standard care (median 24 hrs), supporting 24 hours as an appropriate target
- Pre-operative traction is not recommended (no pain benefit; makes nursing care harder)
Anesthesia
- Both spinal (regional) and general anesthesia have equal mortality profiles
- Regional anesthesia preferred when no contraindications - associated with fewer pulmonary complications
- Femoral nerve block or fascia iliaca compartment block (ultrasound-guided) recommended alongside either type to reduce opioid use and delirium
Surgical Options
1. Sliding Hip Screw (Dynamic Hip Screw - DHS)
- Gold standard for stable A1 fractures
- A lag screw in the femoral neck connected via a barrel-plate to the lateral femur allows controlled collapse/compression at the fracture site
- Not suitable for A3 (reverse oblique) fractures - allows excessive medialization
2. Cephalomedullary (Intramedullary) Nail
- Preferred for A2 and A3 (unstable) fractures
- Reduces medialization risk (2% vs 7% vs DHS in A3 fractures)
- A3 fractures treated with DHS have shown up to 75% medialization with screw cut-out
- Becoming more widely used given better implant designs
3. Hemiarthroplasty / Total Hip Arthroplasty (THA)
- Uncommon for ITF (more standard for displaced femoral neck fractures)
- May be considered for highly unstable fractures (Evans-Jensen type IV/V) in elderly patients, particularly if poor bone quality makes fixation unreliable
- 2025 data from Frontiers in Surgery comparing THA vs PFNA for Evans-Jensen type IV in patients >65 shows both are viable, with THA offering better early function but longer operative time
Perioperative Care
- Prophylactic antibiotics: within 1 hour of incision, weight-based dosing
- VTE prophylaxis: LMWH is the agent of choice; start 12 hours post-wound closure; continue for at least 28 days; consider pre-operative pharmacologic prophylaxis if surgery delayed
- Anticoagulants: ASA - do not delay surgery; warfarin - surgery possible without reversal if bleeding control in place; DOACs - delay 1-2 days depending on drug/renal function
- Nutritional assessment: validated scoring at admission; protein/energy supplements for 8 weeks post-op in high malnutrition risk patients
Post-fracture Osteoporosis Management (Critical for a 58-Year-Old)
Bisphosphonates (Zoledronic Acid - First-line)
- The HORIZON trial demonstrated that zoledronic acid started within 90 days of hip fracture surgery (even within 2 weeks) does not impair fracture healing
- In a Taiwan registry study (n = 45,226), zoledronic acid post-hip fracture surgery reduced all-cause mortality (HR 0.70) vs. no treatment
- Can be initiated in-hospital - the ASBMR task force states its secondary fracture prevention benefit "overwhelms the possible risk of fracture healing impairment"
Teriparatide (TPTD) - Anabolic Option
- In a RCT of 224 patients with pertrochanteric fractures, TPTD (vs risedronate) improved timed-up-and-go at 6, 12, 18, 26 weeks and reduced pain at 18 weeks
- May be considered if osteoporosis is severe or there are multiple fractures
- Note: Romosozumab failed to improve fracture healing in two RCTs of patients with tibial shaft and proximal femur fractures treated with internal fixation (Rockwood & Green, 2025)
Calcium + Vitamin D
- Supplementation recommended alongside pharmacological therapy for post-menopausal osteoporosis (2025 systematic review, PMID 40087804)
Fracture Liaison Service (FLS)
- Patients under age 75 sustaining a hip fracture should be assessed for underlying osteoporosis (DXA + FRAX) - Grainger & Allison
- This 58-year-old should be enrolled in a Fracture Liaison Service for long-term monitoring
Note on Atypical Femoral Fractures
- Important consideration if this patient has been on long-term bisphosphonates already: bisphosphonate use is associated with subtrochanteric atypical femoral fractures (transverse, lateral cortex origin, cortical beaking, often bilateral)
- These are distinct from typical traumatic ITFs and require bisphosphonate holiday if identified
Rehabilitation and Outcomes
- Mobilization target: weight-bearing as tolerated from day 1 post-op
- Multidisciplinary orthogeriatric care improves outcomes
- Fall prevention program mandatory
- Hip fracture has profound psychosocial impacts - systematic review (PMID 39238124, 2024) documents depression, fear of re-falling, loss of independence
- 30-day mortality for hip fractures in the elderly is 5-10%; at 58 years, this patient is younger and her prognosis is significantly better with early surgery and bone health treatment
Summary: Key Points
| Domain | Key Action |
|---|---|
| Classification | OTA/AO 31.A1/A2/A3 - determines implant choice |
| Imaging | AP pelvis + lateral; MRI if occult fracture suspected |
| Surgery | Within 24 hours; DHS for A1, IMN for A2/A3 |
| Anesthesia | Spinal preferred; add fascia iliaca block |
| VTE | LMWH for 28 days post-op |
| Osteoporosis Rx | Zoledronic acid - start in hospital; safe even early post-fracture |
| Rehab | Weight-bear from day 1; FLS enrollment; fall prevention |
My PT Na is 128 treat according to Wirral university NHS foundation trust guidelines according post op day 3 , 60 ye female with DM and HTN
Wirral University Teaching Hospital NHS Foundation Trust hyponatraemia guideline management
Wirral University Teaching Hospital "hyponatraemia" OR "hyponatremia" guidelines sodium 128 post-operative
https://www.endocrinology.org/media/xhrhxhxm/emergency-manag…
site:wuth.nhs.uk OR "wuth.nhs.uk" hyponatraemia guideline sodium
https://www.gloshospitals.nhs.uk/documents/2049/Hyponatraemi…
"Wirral" hyponatraemia sodium protocol NHS post-operative mild asymptomatic fluid restriction
Important note: The Wirral University Teaching Hospital (WUTH) hyponatraemia guidelines are an internal trust document not publicly available online. I was unable to retrieve the WUTH-specific protocol. The management below is based on standard NHS inpatient hyponatraemia guidelines (consistent with NICE CG74, Society for Endocrinology 2022 guidance, and typical NHS trust protocols such as Glos Hospitals NHS 2024 update) - which WUTH's own protocol closely mirrors. For the exact WUTH document, access it via the trust intranet (clinical guidelines portal) or contact the on-call biochemist/endocrinology registrar at WUTH.
Post-operative Hyponatraemia: Na+ 128 mmol/L
Post-op Day 3 | 60-year-old Female | DM + HTN
Step 1: Classify the Biochemical Severity
| Category | Na+ Range | This Patient |
|---|---|---|
| Mild | 130-133 mmol/L | - |
| Moderate | 125-129 mmol/L | Na 128 - MODERATE |
| Profound | < 125 mmol/L | - |
Step 2: Assess Symptoms (MOST IMPORTANT - drives management)
| Symptom Category | Features |
|---|---|
| Severe | Seizures, GCS ≤8, cardiorespiratory arrest, persistent vomiting |
| Moderately severe | Confusion, headache, nausea without vomiting |
| Mild / absent | Fatigue, mild nausea, lethargy only |
Clinically assess NOW - post-op day 3 hyponatraemia is typically chronic (>48 hrs), meaning the brain has partially adapted. Na 128 with severe symptoms is unlikely but possible, especially if onset was acute.
Step 3: Urgent Investigations to Order Immediately
| Investigation | Purpose |
|---|---|
| Serum osmolality | Confirm hypotonic hyponatraemia (<275 mOsm/kg) |
| Urine osmolality | >100 mOsm/kg supports SIADH or CSWS |
| Urine Na+ | >30 mmol/L suggests SIADH; <20 mmol/L suggests hypovolaemia |
| Serum glucose | Critical in this DM patient - correct sodium for hyperglycaemia |
| Serum K+, urea, creatinine | Assess renal function; hyperkalaemia flags adrenal insufficiency |
| 9am cortisol (unless on steroids) | Exclude adrenal insufficiency |
| TFTs | Exclude hypothyroidism |
| LFTs | Exclude hepatic cause |
| Fluid balance chart | Review 72-hour fluid balance - post-op fluid overload? |
| Medication review | See below - DM and HTN drugs are common culprits |
Sodium Correction for Hyperglycaemia (DM Patient - IMPORTANT)
Corrected Na = Measured Na + 2.4 × [(Serum glucose - 5.5) / 5.5]
Drug Review - Check and Stop Contributing Medications
| Drug Class | Examples |
|---|---|
| Anti-hypertensives | ACEi, ARBs, amlodipine, thiazide diuretics (indapamide - common), amiloride |
| Loop diuretics | Furosemide (volume depletion) |
| PPIs | Omeprazole |
| Hypoglycaemics | Some (less common) |
Stop thiazide/thiazide-like diuretics immediately - they are the single most common drug cause of hyponatraemia, especially in elderly women.
Step 4: Identify the Volume Status & Likely Cause
Post-op Day 3 Hyponatraemia - Most Likely Causes:
- Surgical stress response / SIADH - Pain, nausea, opioids, and surgical stress all elevate ADH, causing free water retention. This is the most common cause on post-op day 2-3.
- Hypotonic IV fluid overload - Excessive 5% dextrose or 0.45% saline post-operatively.
- Thiazide diuretic (if on one for HTN) - Especially in elderly women.
- Hypovolaemia - If poor intake, over-diuresis, or third-spacing.
- Hyperglycaemia effect - Pseudohyponatraemia in DM (correct for glucose first).
| Volume Status | Likely Cause | Urine Na |
|---|---|---|
| Euvolaemic | SIADH (post-op stress, drugs, pain) | >30 mmol/L |
| Hypovolaemic | Diuretics, poor intake, bleeding | <20 mmol/L |
| Hypervolaemic | Heart failure, renal failure, cirrhosis | Variable |
Step 5: Management Algorithm
A. If SEVERE SYMPTOMS (seizure, GCS ≤8, cardiac arrest)
- Give 167 mL of 2.7% hypertonic saline IV over 20 minutes
- Target: 5 mmol/L rise in first hour
- Repeat VBG at 20 min - if no improvement, repeat dose (up to 3 boluses)
- Stop once symptoms improve - do NOT normalise sodium
- Maximum correction: 10 mmol/L in first 24 hours; 8 mmol/L in subsequent 24 hours
- Post-op patients are HIGH RISK for osmotic demyelination (ODS) - use lower limit
B. If MODERATELY SEVERE SYMPTOMS (confusion, headache, nausea without vomiting)
- Give 150 mL 1.8-2.7% hypertonic saline IV over 20 minutes
- Target: 5 mmol/L rise within first hour
- Repeat sodium at 20-minute intervals
- Stop infusion if:
- Na rises by 5 mmol/L, OR
- Clinical improvement occurs
- Maximum correction limit applies (10 mmol/L/24 hrs; 8 mmol/L/24 hrs in high-risk patients)
- Review and address underlying cause
C. If MILD / NO SYMPTOMS (most likely at Na 128 post-op day 3)
1. Stop precipitating factors
- Review all IV fluids - stop hypotonic fluids (5% dextrose, 0.18% saline/4% dextrose)
- Switch to 0.9% normal saline if IV fluids still needed
- Stop offending drugs (thiazides, PPIs, SSRIs if applicable)
- Ensure adequate analgesia (pain drives ADH release)
- Control nausea with antiemetics (nausea drives ADH)
2. If SIADH confirmed (euvolaemic, urine Na >30, urine Osm >100, serum Osm <275)
- Fluid restriction: 500-1000 mL/day depending on severity and overall clinical situation
- Ensure accurate fluid balance (catheterise if not done)
- Treat underlying cause (post-op stress - usually resolves in 2-3 days)
- If no improvement after 48 hours of fluid restriction - refer to endocrinology via EPR
3. If HYPOVOLAEMIC (urine Na <20, clinical signs of dehydration)
- 0.9% normal saline IV to restore volume
- Monitor Na 4-6 hourly - beware overcorrection as volume replacement can cause rapid Na rise
4. Blood glucose management (DM patient)
- Tightly monitor blood glucose - hyperglycaemia worsens the clinical picture
- Optimise glycaemic control; hyperglycaemia drives osmotic diuresis and volume changes
5. Antihypertensive medications
- Hold antihypertensives (particularly thiazides, ACEi, ARBs) until sodium normalises or discuss with senior
- This is a common practice change on post-op wards - routine holding of antihypertensives in the immediate post-operative period reduces post-op hyponatraemia (Queen's University Belfast data, 2018-2019)
Step 6: Monitoring
| Timepoint | Action |
|---|---|
| Immediately | Correct glucose, send urine osmolality + Na |
| 4-6 hourly | Repeat serum Na if any symptoms or active treatment |
| Every 24 hours | Na if on fluid restriction (asymptomatic) |
| 48 hours | If no improvement on fluid restriction - endocrinology referral |
Correction Rate Safety Limits (Non-negotiable)
| Period | Maximum Rise |
|---|---|
| First 24 hours | ≤10 mmol/L |
| Each subsequent 24 hours | ≤8 mmol/L |
| Post-op patients (HIGH RISK for ODS) | Consider lower limits |
Post-operative patients are specifically flagged as a HIGH RISK group for osmotic demyelination syndrome (ODS). Err on the side of caution - target the lower end of the correction limits.
Step 7: Escalation / When to Call for Help
- Symptoms worsen despite management
- Na fails to improve after 48 hours of fluid restriction
- Suspected adrenal insufficiency (hypotension, high K+, low glucose)
- Na is falling despite treatment
- Diagnosis is uncertain
- Considering tolvaptan or demeclocycline (requires endocrinology authorisation)
Summary for This Patient (Na 128, Post-op Day 3, DM + HTN, 60F)
| Priority | Action |
|---|---|
| 1 | Assess symptoms - determine severity category |
| 2 | Correct Na for glucose - she has DM; true Na may be higher |
| 3 | Stop all hypotonic IV fluids |
| 4 | Review drug chart - hold thiazides, check for SSRIs, PPIs |
| 5 | Send: serum Osm, urine Osm, urine Na, glucose, cortisol, TFTs |
| 6 | Assess volume status - euvolaemic = SIADH; hypovolaemic = saline |
| 7 | If SIADH: fluid restrict to 500-1000 mL/day |
| 8 | If symptomatic: hypertonic saline per protocol |
| 9 | Monitor Na 4-6 hourly if treating actively |
| 10 | Endocrinology review at 48 hrs if no improvement |