Give me details anatomy of base of skull , ear , nose , throat . From basic to surgical advances
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Reading File
Reading File
Searching the Web
ENT surgical anatomy base of skull nose throat overview 2024 2025
Loading Image
Loading Image
I now have extensive material. Let me compile the comprehensive answer.
Detailed Anatomy of the Base of Skull, Ear, Nose, and Throat - Basic to Surgical
Sources: Cummings Otolaryngology Head and Neck Surgery (7th ed.), Gray's Anatomy for Students, Scott-Brown's Otorhinolaryngology
PART I: BASE OF SKULL
Overview
The skull base forms the floor of the cranial cavity, composed of five bones: ethmoid, sphenoid, occipital, frontal, and paired temporal bones. It is divided into three regions - anterior, middle, and posterior cranial fossae.
The skull base anatomy overview at Medscape summarizes the three fossae well. Key structures passing through each region:
| Fossa | Contents / Key Foramina |
|---|---|
| Anterior | Olfactory nerves (CN I) through cribriform plate; optic nerve (CN II) through optic canal |
| Middle | Temporal lobes; CN V (trigeminal) via foramen ovale/rotundum; middle meningeal artery (foramen spinosum); internal carotid via foramen lacerum |
| Posterior | CN VII and VIII via IAC; CN IX, X, XI via jugular foramen; CN XII via hypoglossal canal; foramen magnum |
Lateral Skull Base - The Temporal Bone (Surgical Focus)
The temporal bone is the centerpiece of ENT surgery. It occupies the lateral skull base and articulates with the sphenoid, parietal, occipital, and zygomatic bones. It has a pyramidal shape divided into four embryologically distinct components:
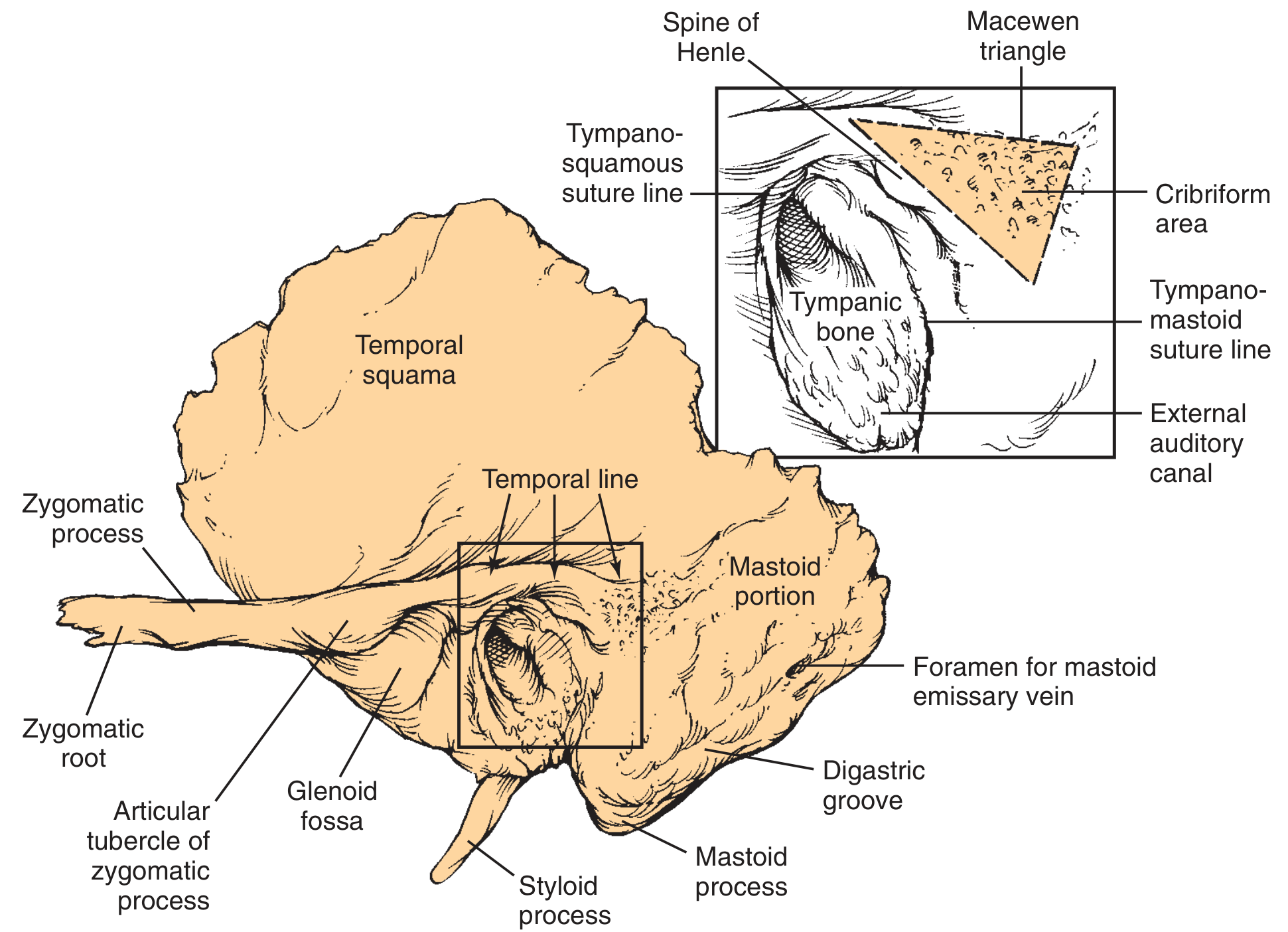
1. Squamous part
- Forms the lateral wall of the middle cranial fossa
- Contains the zygomatic process (roof of glenoid fossa)
- The temporal line is ~5 mm inferior to the middle fossa floor - a critical surgical landmark
- Temporalis muscle inserts on outer cortex; masseter on zygomatic process
2. Mastoid part
- Bullous bony structure shaped by air cells; tip elongated by SCM and digastric pull
- MacEwen triangle (cribriform area): depressed area posterior to Spine of Henle - surgical gateway to mastoid antrum
- Stylomastoid foramen at anterior limit of digastric groove - exit point for CN VII
- Mastoid emissary vein communicates with sigmoid sinus
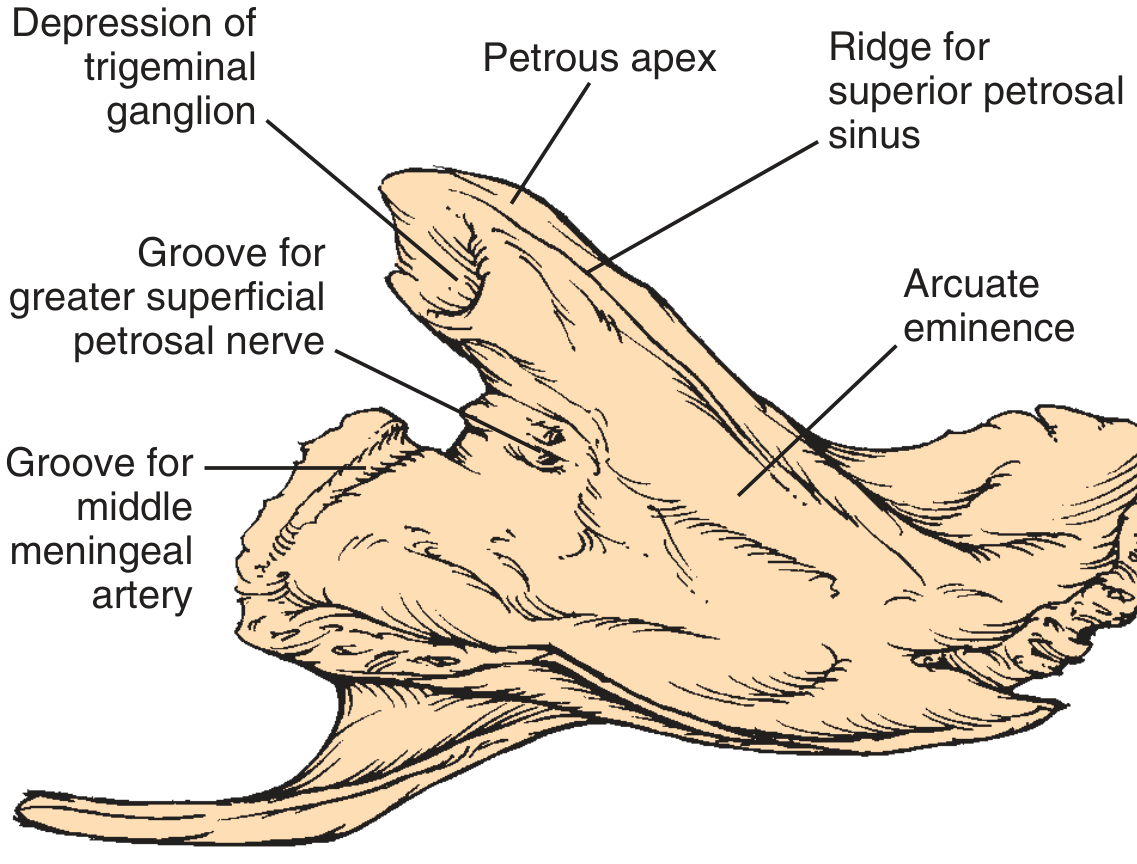
3. Petrous part (pyramid-shaped, pointing anteromedially)
- Superior face (middle fossa floor): shows arcuate eminence (prominence of superior semicircular canal), groove for GSPN, depression for trigeminal ganglion (Meckel cave)
- Posterior face (anterior wall of posterior fossa): houses the internal auditory meatus; framed by sigmoid, superior petrosal, and inferior petrosal sinus sulci
- Petrous apex: between occipital and sphenoid bones; Meckel cave contains trigeminal ganglion here
4. Tympanic part
- Forms anterior and inferior walls + part of posterior wall of the bony EAC
- Forms the posterior wall of the glenoid fossa (TMJ)
- Ends medially at the tympanic sulcus where the TM inserts
- Foramen of Huschke: defect in anterior bony canal from incomplete ossification - allows spread of disease to parotid gland deep lobe
Key Foramina of the Skull Base (Surgical Relevance)
| Foramen | Contents | Surgical Significance |
|---|---|---|
| Foramen spinosum | Middle meningeal artery | Middle fossa floor dissection |
| Foramen ovale | CN V3 (mandibular) | Infratemporal fossa approach |
| Foramen rotundum | CN V2 (maxillary) | Pterygopalatine fossa surgery |
| Jugular foramen | CN IX, X, XI; jugular bulb | Glomus jugulare resection |
| IAC (internal acoustic meatus) | CN VII, VIII; labyrinthine artery | Acoustic neuroma surgery |
| Carotid canal | Internal carotid artery | Petrous apex, infratemporal fossa |
| Stylomastoid foramen | CN VII (exit) | Mastoidectomy, parotid surgery |
| Foramen lacerum | ICA transition (horizontal to vertical) | Base of skull tumor surgery |
| Hypoglossal canal | CN XII | Posterior skull base tumors |
Jugular Foramen Anatomy
The jugular foramen is formed at the petro-occipital junction and is partitioned into:
- Pars nervosa (posterior): CN IX, Jacobson nerve; cochlear aqueduct opening is just medial/anterior to jugular spine, marking its most superior limit
- Pars venosa (anterior): jugular bulb, CN X and XI
The jugular bulb dome sits directly under the middle ear space. The keel (wedge of bone) separates it anteriorly from the carotid canal; the tympanic canaliculus penetrates this keel carrying the Jacobson nerve (sensory and preganglionic parasympathetic fibers).
Surgical Approaches to the Skull Base
| Approach | Target Region | Key Steps |
|---|---|---|
| Middle fossa approach | IAC, petrous apex | Temporal craniotomy; arcuate eminence and GSPN as landmarks; cochlea lies in bone subtended by 120° angle between GSPN, geniculate ganglion, and labyrinthine CN VII segment |
| Translabyrinthine approach | IAC, CPA | Mastoidectomy + labyrinthectomy; cochlear aqueduct = inferior limit of dissection |
| Retrosigmoid approach | CPA, posterior fossa | Behind sigmoid sinus; exposes CPA without sacrificing hearing |
| Infratemporal fossa approach (Fisch) | Jugular foramen, petrous ICA | Rerouting of CN VII anteriorly; resection of posterior EAC |
| Endoscopic endonasal skull base | Anterior + middle skull base | Through sphenoid/ethmoid sinuses; resects pituitary, clivus, cribriform lesions |
- Cummings Otolaryngology, p. 3341-3360
PART II: THE EAR
External Ear
Auricle (Pinna)
The auricle is a funnel-shaped cartilaginous structure (elastic cartilage + perichondrium) covered by keratinizing squamous epithelium. Its intricate surface anatomy:
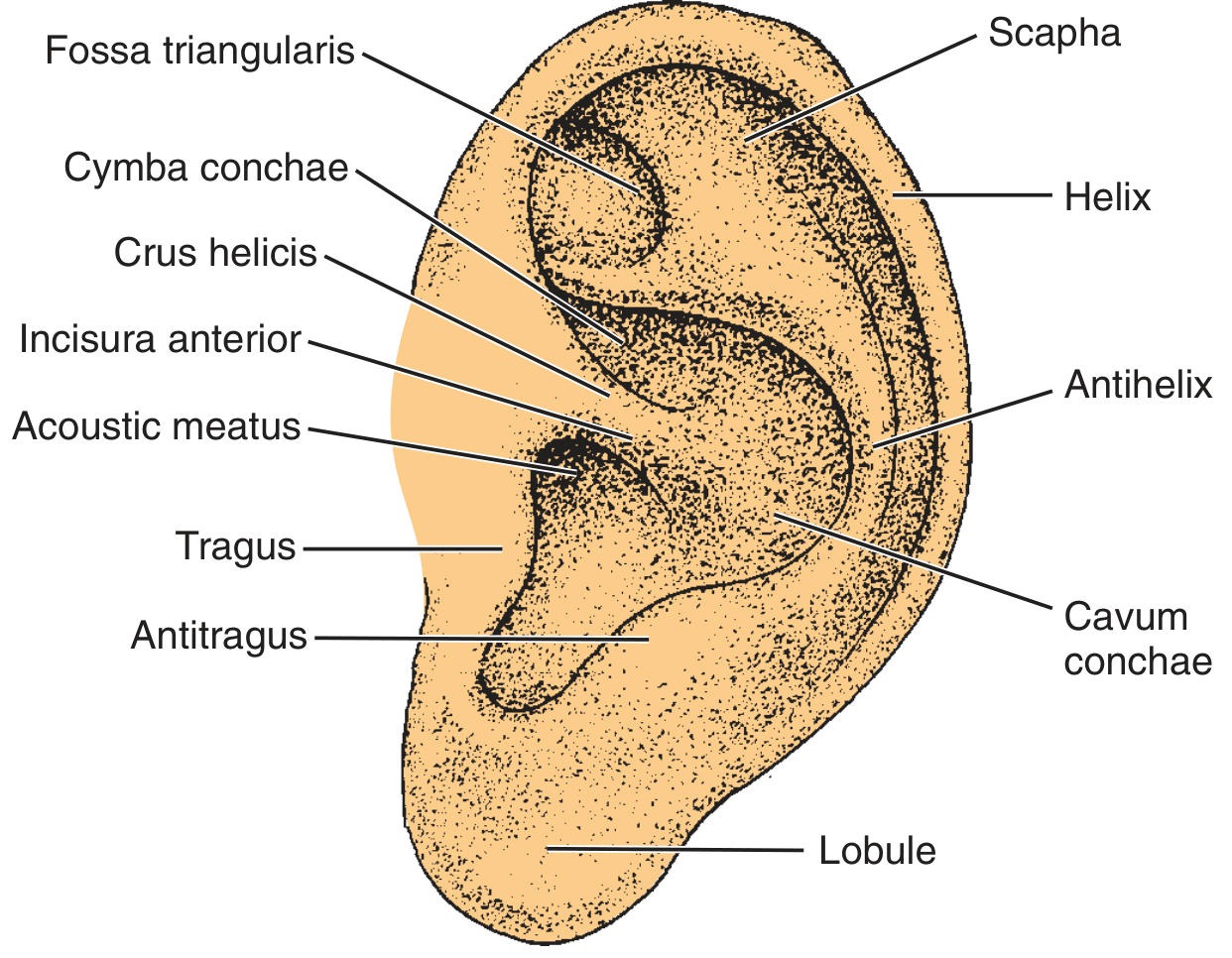
Key landmarks: helix, antihelix, scapha, cymba conchae, cavum conchae, fossa triangularis, tragus, antitragus, lobule (only lobule is fat - no cartilage), incisura anterior.
Blood supply from external carotid: posterior auricular artery (medial surface) + superficial temporal artery (lateral). Lymph drain to preauricular, postauricular, and upper deep cervical nodes.
External Auditory Canal (EAC)
- Length: ~2.5 cm in adults
- Lateral 1/3: cartilaginous, contains sebaceous + apocrine (ceruminous) glands, hair follicles, lined by thick mobile skin
- Medial 2/3: bony (tympanic part of temporal bone), covered by thin skin tightly adherent to bone, no glands or hair
- Isthmus = bony-cartilaginous junction = narrowest point; fibrous interface = pathway for malignant spread (requires en bloc lateral temporal bone resection for EAC carcinoma)
- Fissures of Santorini: transverse slits in cartilaginous canal - allow spread of infection/neoplasm to surrounding soft tissues
- Foramen of Huschke: incomplete ossification defect in anterior bony canal - spreads disease to parotid deep lobe
- Cerumen: hydrophobic, slightly acidic (pH 6.0-6.5); formed by glandular secretions + sloughed epithelium; self-cleansing by centrifugal migration from TM surface outward
Tympanic Membrane (TM)
The TM is a four-layered concave membrane forming the medial wall of the EAC and much of the lateral wall of the middle ear:
- EAC skin (outer squamous layer)
- Outer radiate fibrous layer - inserts on malleus manubrium
- Inner circular fibrous layer - circumferential at periphery
- Middle ear mucosa (inner layer)
- Umbo: tip of malleus manubrium attachment (most depressed point)
- Mallear stria: runs superiorly from umbo along manubrium
- Mallear prominence: formed by lateral process of malleus
- Pars flaccida (Shrapnell membrane): superior, lacks fibrous layer; anchored to notch of Rivinus - site of acquired cholesteatoma formation
- Pars tensa: rest of TM (inferior); anchored by annular ligament to tympanic sulcus (fibrocartilaginous ring)
- Anterior and posterior mallear folds demarcate pars tensa from pars flaccida

Middle Ear
The middle ear consists of the tympanic cavity - a mucosa-lined, air-filled space subdivided into:
- Mesotympanum: at the level of the TM
- Epitympanum (attic): above the level of the TM; contains malleus head and incus body
- Hypotympanum: below the level of the TM
Ossicular Chain
- Malleus: consists of handle (manubrium), neck, lateral process, and head; the long process of the malleus is the manubrium; head articulates with incus in the attic
- Incus: body (in attic) + short process (posterior) + long process (descending toward stapes); the long process of the incus has a single nutrient vessel and no collateral circulation - the most vulnerable portion of the ossicular chain to avascular necrosis
- Stapes: head, anterior and posterior crura, oval window footplate; footplate is held in the oval window by the annular ligament
The ossicular chain and mucosal folds separate epitympanum from mesotympanum, leaving narrow apertures for air supply to the attic and antrum.
Medial Wall of Middle Ear (key surgical landmarks)
- Promontory: bulge of basal turn of cochlea
- Oval window (fenestra vestibuli): covered by stapes footplate
- Round window (fenestra cochleae): separated from oval window by round window niche; covered by secondary TM
- Cochleariform process: bony landmark where tensor tympani tendon turns laterally to insert on malleus; facial nerve runs over its superior aspect (key surgical landmark)
- Pyramidal eminence: small bony eminence posterior to oval window; stapedius tendon emerges from its apex
- Facial nerve (tympanic/horizontal segment): runs in fallopian canal over the oval window; may be dehiscent in 15-40% of ears
Epitympanum (Attic)
- Contains heads of malleus and incus
- Supratubal recess (STR): anterior extreme of attic, superior to ET opening; geniculate ganglion lies just deep to its medial wall (may be dehiscent); site of CN VII injury in cholesteatoma surgery or blind dissection
Eustachian Tube (ET)
- ~35 mm long; bony portion (medial 1/3) + cartilaginous portion (lateral 2/3)
- Opens into nasopharynx; functions in pressure equalization and drainage
- The semicanal of the tensor tympani lies superior to the ET semicanal in the musculotubal canal
Inner Ear
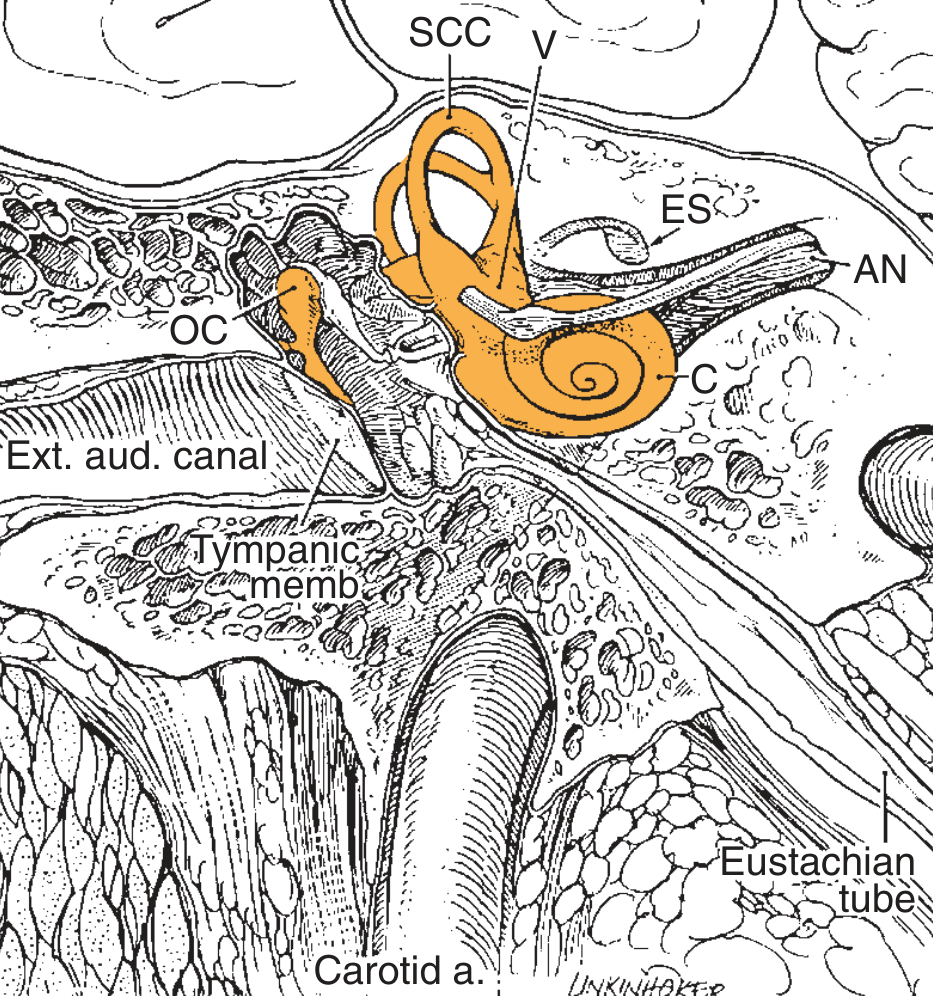
The inner ear is enclosed within the otic capsule - the densest bone in the body, located within the petrous portion of the temporal bone.
Cochlea
- 2.5 turns spiraling around the modiolus
- Tonotopic organization: high frequencies at base, low frequencies at apex
- Three scalae: scala vestibuli (perilymph), scala media / cochlear duct (endolymph), scala tympani (perilymph); helicotrema connects vestibuli and tympani at apex
- Organ of Corti: sits on basilar membrane within scala media; contains inner hair cells (IHC, 3500) and outer hair cells (OHC, 12,000)
- Afferent neurons in the spiral ganglion (bipolar); project centrally as the cochlear nerve
Vestibular Labyrinth
- 3 semicircular canals (superior/anterior, posterior, lateral/horizontal) - sense angular acceleration
- Utricle and saccule (otolithic organs) - sense linear acceleration and gravity
- Superior SCC creates the arcuate eminence on the middle fossa floor - key landmark for middle fossa surgery
Facial Nerve (CN VII) - Temporal Bone Course
The facial nerve traverses the temporal bone in the fallopian canal from IAC fundus to stylomastoid foramen, in four segments:
| Segment | Location | Key Features |
|---|---|---|
| Meatal segment | IAC fundus (anterosuperior quadrant) | No fibrous sheath in IAC; arachnoid-covered |
| Labyrinthine segment | IAC fundus → geniculate ganglion | Shortest, narrowest; watershed vascular supply (vertebrobasilar + external carotid); most vulnerable in viral infections (Bell palsy) and fractures |
| Tympanic (horizontal) segment | Geniculate ganglion → second genu | Runs over cochleariform process; forms superior wall of oval window niche; dehiscent in 25% of ears |
| Mastoid (vertical) segment | Second genu → stylomastoid foramen | Passes anteriorly to lateral SCC (second genu hugs its anterior-inferior aspect); descends posterior to EAC |
At the geniculate ganglion: GSPN leaves anteriorly toward pterygopalatine ganglion (lacrimal gland, nasal glands). The geniculate ganglion is only a thin bone layer from the middle fossa floor, dehiscent in ~25%.
The chorda tympani leaves the mastoid segment, runs across the middle ear (between malleus and incus), and exits via the petrotympanic fissure.
- Cummings Otolaryngology, Ch. 126-127, pp. 2443-2454
Mastoid Pneumatization
Three types: well-pneumatized (cellular), diploic, sclerotic. Pneumatization reaches adult size at puberty. Poor pneumatization correlates with chronic otitis media history. Air cells surround the labyrinth and cortical plates in tracts - the Koerner septum (embryologic petrosquamous junction) is the lateral limit of the antrum and a common source of confusion during mastoidectomy.
PART III: THE NOSE
External Nose and Nasal Framework
The external nose has a bony upper third (nasal bones, frontal process of maxilla) and a cartilaginous lower two-thirds:
- Upper lateral (triangular) cartilages: form the middle vault; articulate with the caudal edge of the nasal bones; the internal nasal valve (angle between upper lateral cartilage and septum, ~15°) is the narrowest part of the nasal airway
- Lower lateral (alar/greater alar) cartilages: medial crura (form columella base) + lateral crura (form alar rims); govern nasal tip projection and rotation
- Nasal septum: quadrilateral cartilage (anterior), perpendicular plate of ethmoid (posterior-superior), vomer (posterior-inferior), maxillary crest + palatine bone (floor)
Nasal Cavity
Boundaries
- Floor: hard palate
- Roof: nasal bones, cribriform plate of ethmoid (very thin, ~0.5 mm - risk of CSF leak in surgery), sphenoid body
- Medial wall: nasal septum
- Lateral wall: most complex - carries the turbinates
Turbinates (Conchae)
Three pairs, each creating a corresponding meatus below:
- Inferior turbinate (largest, independent bone): inferior meatus contains the nasolacrimal duct (opens ~6 mm posterior to the anterior end of the inferior turbinate)
- Middle turbinate (ethmoid bone): middle meatus contains the ostiomeatal complex (OMC) - the drainage pathway for frontal, anterior ethmoid, and maxillary sinuses
- Superior turbinate (ethmoid bone): superior meatus drains posterior ethmoid cells and sphenoid sinus via sphenoethmoidal recess
Ostiomeatal Complex (OMC)
- Key structures: uncinate process, hiatus semilunaris, ethmoid bulla, infundibulum
- Maxillary sinus ostium opens into infundibulum (ethmoid infundibulum)
- Frontal recess drains above/lateral to uncinate process
- Site of obstruction in chronic rhinosinusitis - target of FESS (functional endoscopic sinus surgery)
Blood Supply of the Nasal Cavity
- Kiesselbach plexus (Little's area): anterior septum, anastomosis of 5 arteries:
- Anterior ethmoidal artery (from ophthalmic artery → ICA)
- Posterior ethmoidal artery (from ophthalmic artery)
- Sphenopalatine artery (largest - from internal maxillary artery → ECA) - enters nasal cavity through sphenopalatine foramen (posterior to middle turbinate)
- Greater palatine artery
- Superior labial branch of facial artery
- Anterior epistaxis: >90% at Little's area (Kiesselbach plexus); managed conservatively or by cautery
- Posterior epistaxis: sphenopalatine artery territory; requires endoscopic sphenopalatine artery ligation or embolization
Olfactory Region
- Upper nasal cavity: olfactory epithelium (pseudostratified columnar with olfactory receptor neurons)
- Fila olfactoria pass through cribriform plate foramina → olfactory bulb
- Cribriform plate = thinnest skull base bone; fractured in anterior skull base trauma (CSF rhinorrhea); traversed in endoscopic skull base approaches
Paranasal Sinuses
| Sinus | First visible | Drainage | Surgical Note |
|---|---|---|---|
| Maxillary | Birth | OMC (infundibulum) | Largest sinus; root of antrum = floor of orbit; inferior turbinate runs along entire lateral wall; accessory ostia common |
| Ethmoid | Birth | Multiple ostia; anterior → OMC; posterior → superior meatus/sphenoethmoidal recess | Paper-thin lamina papyracea (medial wall of orbit) - blown out in trauma/surgery |
| Frontal | 2-4 years | Frontal recess → OMC | Variable drainage; nasofrontal duct anatomy highly variable |
| Sphenoid | 3 years | Sphenoethmoidal recess | Most posterior; roof = planum sphenoidale; lateral wall = cavernous sinus + CN II, III, IV, V1, VI; sella above (pituitary) |
Surgical Notes on Sinuses
- Lamina papyracea: paper-thin medial orbital wall; penetration during ethmoidectomy can herniate orbital fat or injure medial rectus
- Optic nerve: may bulge into sphenoid sinus or be dehiscent in 4-6% of people - endangered during posterior ethmoidectomy and sphenoidotomy
- Anterior ethmoidal artery: crosses the orbit to enter the skull base at the junction of the ethmoid roof and the anterior skull base; ligation used in epistaxis management; landmark in endoscopic skull base surgery
- FESS (Functional Endoscopic Sinus Surgery): based on middle meatus surgery - uncinectomy, ethmoid bulla opening, frontal recess widening, maxillary ostium enlargement
PART IV: THE THROAT (Pharynx and Larynx)
Pharynx
The pharynx is a half-cylinder chamber, walls formed by muscles and fascia. Its walls attach superiorly to the base of skull and inferiorly to esophageal margins.
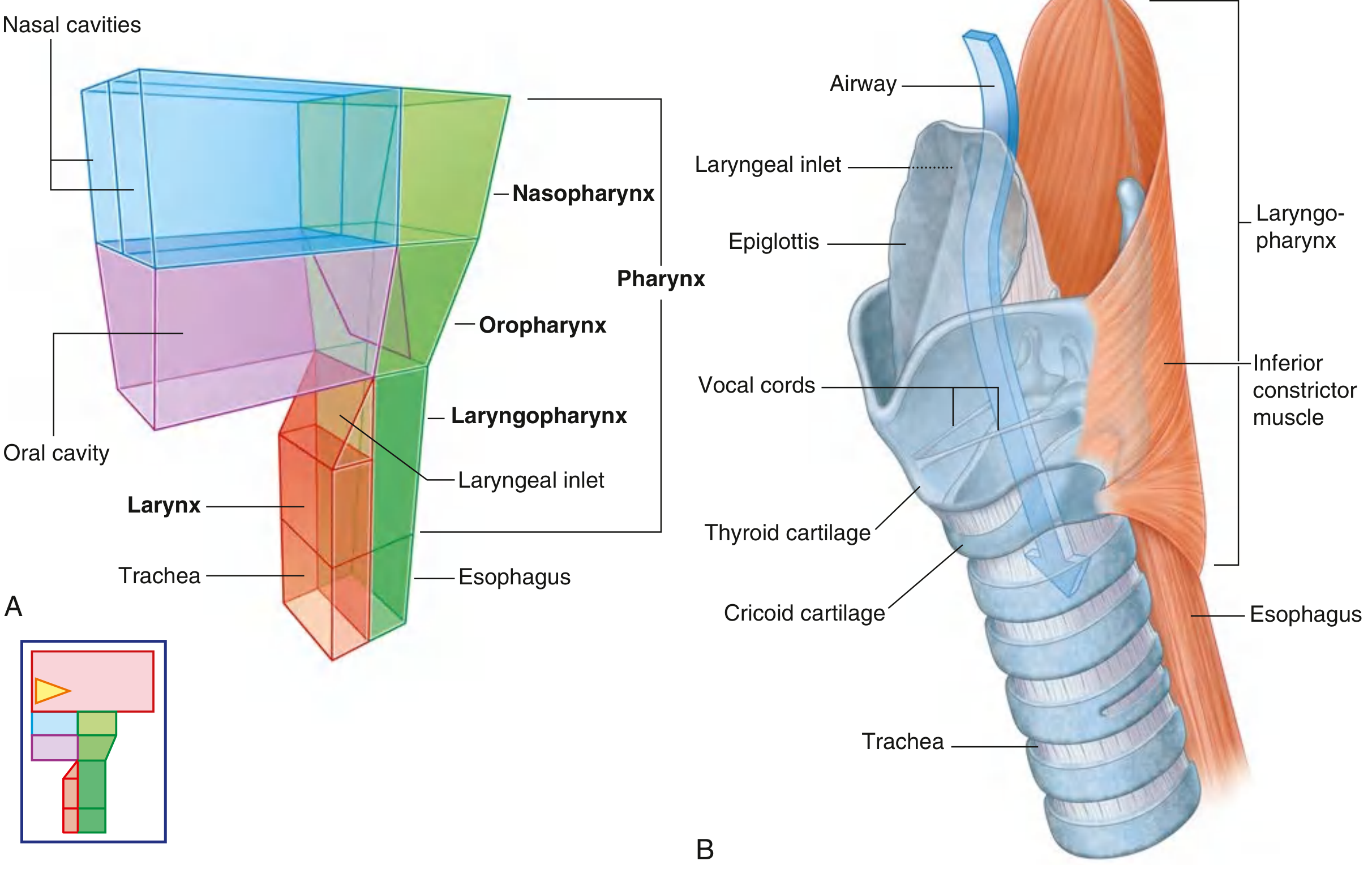
Three regions:
1. Nasopharynx (posterior to nasal cavities)
- Roof = body of sphenoid + basioccipital
- Posterior wall = C1-C2 vertebrae
- Lateral wall = Eustachian tube orifice (torus tubarius) with the Fossa of Rosenmüller (lateral pharyngeal recess) - most common site of nasopharyngeal carcinoma
- Adenoid (pharyngeal tonsil) on posterior wall
- Passavant ridge: formed by superior pharyngeal constrictor during swallowing/speech
2. Oropharynx (posterior to oral cavity, from soft palate to hyoid bone)
- Contains: soft palate, uvula, anterior and posterior tonsillar pillars (palatoglossus + palatopharyngeus), palatine tonsils (between pillars in tonsillar fossa), posterior pharyngeal wall, base of tongue (lingual tonsil, circumvallate papillae)
- Waldeyer ring: lymphoid tissue ring - adenoids (nasopharynx), tubal tonsils (ET orifice), palatine tonsils, lingual tonsil
- Peritonsillar space: potential space between tonsillar capsule and superior pharyngeal constrictor - site of peritonsillar abscess; surgical access by needle aspiration or incision and drainage
3. Hypopharynx / Laryngopharynx (from hyoid bone to lower border of cricoid cartilage)
- Piriform fossae (sinuses): lateral recesses on either side of the laryngeal inlet; lined by mucosa over inner surface of thyroid cartilage; common site of hypopharyngeal cancer and foreign body impaction
- Posterior pharyngeal wall: C3-C6 vertebrae
- Postcricoid region: posterior to the cricoid
Pharyngeal Musculature
- Superior, middle, inferior pharyngeal constrictors (overlap like stacked cups; innervated by pharyngeal plexus - CN IX, X)
- Stylopharyngeus (CN IX alone): elevates pharynx
- Salpingopharyngeus (CN X): opens ET during swallowing
- Palatopharyngeus (CN X): elevates and closes nasopharynx
Killian Dehiscence (Pharyngeal Pouch)
Triangular weakness between thyropharyngeus (oblique fibers) and cricopharyngeus (horizontal fibers) of inferior pharyngeal constrictor. The cricopharyngeus is the principal component of the upper esophageal sphincter (UES). A pharyngeal (Zenker's) diverticulum herniates posteriorly through this gap. Surgery: cricopharyngeal myotomy ± diverticulectomy (open or endoscopic stapler via rigid esophagoscopy).
Larynx
The larynx is the upper airway, attached below to the trachea and above to the hyoid bone via the thyrohyoid membrane.
Cartilage Framework
| Cartilage | Description | Clinical Note |
|---|---|---|
| Thyroid | Largest; two laminae fused at laryngeal prominence (Adam's apple); angle 90° (male), 120° (female) | Palpable landmark; framework for cricothyrotomy |
| Cricoid | Only complete ring; connects thyroid anteriorly via cricothyroid joints | Cricothyroidotomy site: between thyroid and cricoid cartilages |
| Epiglottis | Leaf-shaped, elastic cartilage; attached to thyroid and hyoid | Diverts bolus laterally into piriform fossae during swallowing |
| Arytenoids (paired) | Sit on posterior cricoid; vocal process (anterior) + muscular process (posterior) | Vocal process anchors posterior vocal cord; muscular process rotates for abduction/adduction |
| Corniculate + cuneiform | Small cartilages forming aryepiglottic fold contour | Clinical landmark in laryngoscopy |
Laryngeal Inlet and Internal Spaces
- Laryngeal inlet: tilted posteriorly; bounded by epiglottis (anterior), aryepiglottic folds (lateral), interarytenoid notch (posterior)
- Vestibule: from inlet to false (vestibular) folds
- False vocal folds (vestibular folds): mucosa over vestibular ligament; no phonation function
- Laryngeal ventricle (sinus of Morgagni): recess between true and false cords; the saccule extends superiorly from its anterior end
- True vocal folds (cords): from vocal process of arytenoid to inner surface of thyroid cartilage; consist of epithelium + Reinke's space + vocal ligament + vocalis muscle; vibrate at fundamental frequency during phonation
- Subglottis: below true cords to lower border of cricoid; narrowest part of infant airway (ring of cricoid)
Laryngeal Compartments
- Supraglottis: from laryngeal inlet to plane through laryngeal ventricle
- Glottis: true vocal folds + anterior and posterior commissures (1 cm above and below free edge)
- Subglottis: from lower border of glottis to lower border of cricoid
Laryngeal Muscles
All intrinsic laryngeal muscles are innervated by the recurrent laryngeal nerve (RLN) (CN X branch), EXCEPT the cricothyroid (external branch of superior laryngeal nerve).
| Muscle | Action |
|---|---|
| Posterior cricoarytenoid (PCA) | Only abductor of vocal cords; opens airway |
| Lateral cricoarytenoid (LCA) | Adductor (closes airway) |
| Thyroarytenoid (vocalis) | Shortens/thickens vocal cord |
| Interarytenoid (transverse + oblique) | Adducts arytenoids; closes posterior glottis |
| Cricothyroid | Lengthens/tenses vocal cord (pitch control) |
Laryngeal Innervation
- Superior laryngeal nerve (SLN) from vagus:
- Internal branch: sensory above cords (laryngeal inlet, epiglottis, piriform fossa) - pierces thyrohyoid membrane
- External branch: motor to cricothyroid muscle; at risk during thyroid surgery (affects pitch)
- Recurrent laryngeal nerve (RLN):
- Right: hooks under right subclavian artery
- Left: hooks under arch of aorta, runs in tracheoesophageal groove
- Enters larynx just posterior to cricothyroid joint under lower border of inferior pharyngeal constrictor
- Supplies all intrinsic laryngeal muscles except cricothyroid + sensory below vocal cords
- At major risk during thyroid, parathyroid, and anterior cervical spine surgery
Blood Supply
- Superior laryngeal artery (from superior thyroid artery): enters via thyrohyoid membrane with internal SLN
- Inferior laryngeal artery (from inferior thyroid artery): with RLN
Fascial Spaces and Deep Neck
Pharyngeal and laryngeal anatomy cannot be separated from deep neck spaces:
- Retropharyngeal space: between posterior pharyngeal wall and prevertebral fascia; from skull base to T1-T2; conduit for infection spread from neck to mediastinum
- Parapharyngeal space: prestyloid (contains ICA, IJV, CN IX-XII, sympathetic chain); poststyloid fat space
- Danger space (space 4): between alar and prevertebral fascia; extends from skull base to diaphragm - rapid spread of deep neck infection to mediastinum
Surgical Advances Summary
| Domain | Advance |
|---|---|
| Skull base | Endoscopic endonasal approaches (expanded EEA) to anterior/middle skull base; navigation/image-guided surgery; robotic-assisted skull base |
| Ear | Endoscopic ear surgery (EES/TEES - transcanal endoscopic ear surgery); cochlear implantation; bone-anchored hearing aids (BAHA); fully implantable hearing devices; robot-assisted cochlear implant electrode insertion |
| Nose/sinuses | FESS with intraoperative CT navigation; balloon sinuplasty; drug-eluting sinus stents; biologic therapies (dupilumab) for CRS with nasal polyps as alternative to surgery |
| Throat/airway | Transoral robotic surgery (TORS) for oropharyngeal cancer; microlaryngoscopy with cold instruments vs. CO₂ laser vs. KTP laser; office-based laser procedures under topical anesthesia; laryngeal framework surgery (thyroplasty, arytenoid adduction) for vocal cord paralysis |
- Cummings Otolaryngology, Chapters 126-127, 175; Gray's Anatomy for Students, Chapters 8 and related; Scott-Brown's Otorhinolaryngology
Key Surgical Mnemonics / High-Yield Points
- Only abductor of the vocal cord = Posterior CricoArytenoid (PCA) - bilateral RLN palsy = adducted cords = stridor/airway emergency
- Most vulnerable ossicle = Long process of incus (single blood supply)
- MacEwen triangle = guide to mastoid antrum (posterior to Spine of Henle, inferior to temporal line)
- Kiesselbach plexus (Little's area, anterior septum) = site of 90% of epistaxis
- Cribriform plate = thinnest skull base bone; torn in anterior head trauma → CSF rhinorrhea + anosmia
- Geniculate ganglion = dehiscent in 25% of ears; site of viral tropism (Ramsay Hunt syndrome = herpes zoster oticus)
- Killian dehiscence = weak posterior pharynx between thyropharyngeus and cricopharyngeus = Zenker's diverticulum
- Pharyngeal plexus innervation: all pharyngeal muscles except stylopharyngeus (CN IX alone)
- Left RLN longer course (hooks aortic arch) = more commonly injured/compressed by mediastinal lesions/thyroid goiter
- Sphenopalatine artery = terminal branch of internal maxillary artery = workhorse of posterior epistaxis surgery
Create a detailed surgical anatomy atlas with labeled cross-sections and 3D visualization
Reading File
Reading File
Running Command
mkdir -p /home/daytona/workspace/ent-atlas && ls /home/daytona/workspace/ent-atl…
Continue from where its left
This is a shared conversation. Sign in to Orris to start your own chat.