Metastatic lung disease radiology and for 10 mark precise and for radiology pg exam
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
I now have all the material needed for a thorough, exam-focused 10-mark answer. Here is the complete response:
Metastatic Lung Disease - Radiology (10 Marks)
Source: Grainger & Allison's Diagnostic Radiology; Schwartz's Principles of Surgery, 11e
Definition & Routes of Spread
Secondary (metastatic) lung tumours reach the lung via four pathways:
- Haematogenous - most common; tumour cells lodge in pulmonary capillaries and grow as discrete nodules
- Lymphatic - gives lymphangitic carcinomatosis
- Direct extension - from hilar nodes, pleura, or a primary bronchial carcinoma into adjacent tissue
- Endobronchial - rare; submucosal deposits cause airway obstruction
Common primary sites: Breast, gastrointestinal tract, kidney, testis, head and neck, and bone/soft-tissue sarcomas.
Radiological Patterns
1. Discrete Pulmonary Nodules (Haematogenous Metastases)
The hallmark pattern. Key features:
| Feature | Detail |
|---|---|
| Number | Multiple (occasionally solitary, seen in 2-3% of all series) |
| Distribution | Peripheral and basal - most evident on CT |
| Shape | Usually spherical and well-defined |
| Edge | Irregular in adenocarcinoma ("spiculated" or corona radiata sign) |
| Calcification | Rare, except in osteosarcoma and chondrosarcoma |
| Cavitation | Seen in squamous cell carcinoma metastases (e.g. from head and neck primary) |
| Growth rate | Explosive doubling in choriocarcinoma/osteosarcoma (<30 days); very slow in thyroid carcinoma |
CXR: Detects most nodules >1 cm. High-kV technique used to reveal lesions behind heart, diaphragm, and mediastinum.
CT: MDCT shows nodules >3 mm. Below 6 mm, differentiation from granulomas (TB, histoplasmosis) is unreliable.
- With multiple non-calcified nodules on plain CXR: probability of metastases >90% (near 100% in non-endemic areas).
- For CT-only visible nodules <1 cm: probability may fall to 50%, depending on community prevalence of infectious granulomas.
2. Cannon-ball Metastases
- Term used for large, round, well-defined bilateral pulmonary nodules
- Classically associated with: renal cell carcinoma, testicular germ cell tumours, choriocarcinoma
- Easily visible on plain CXR
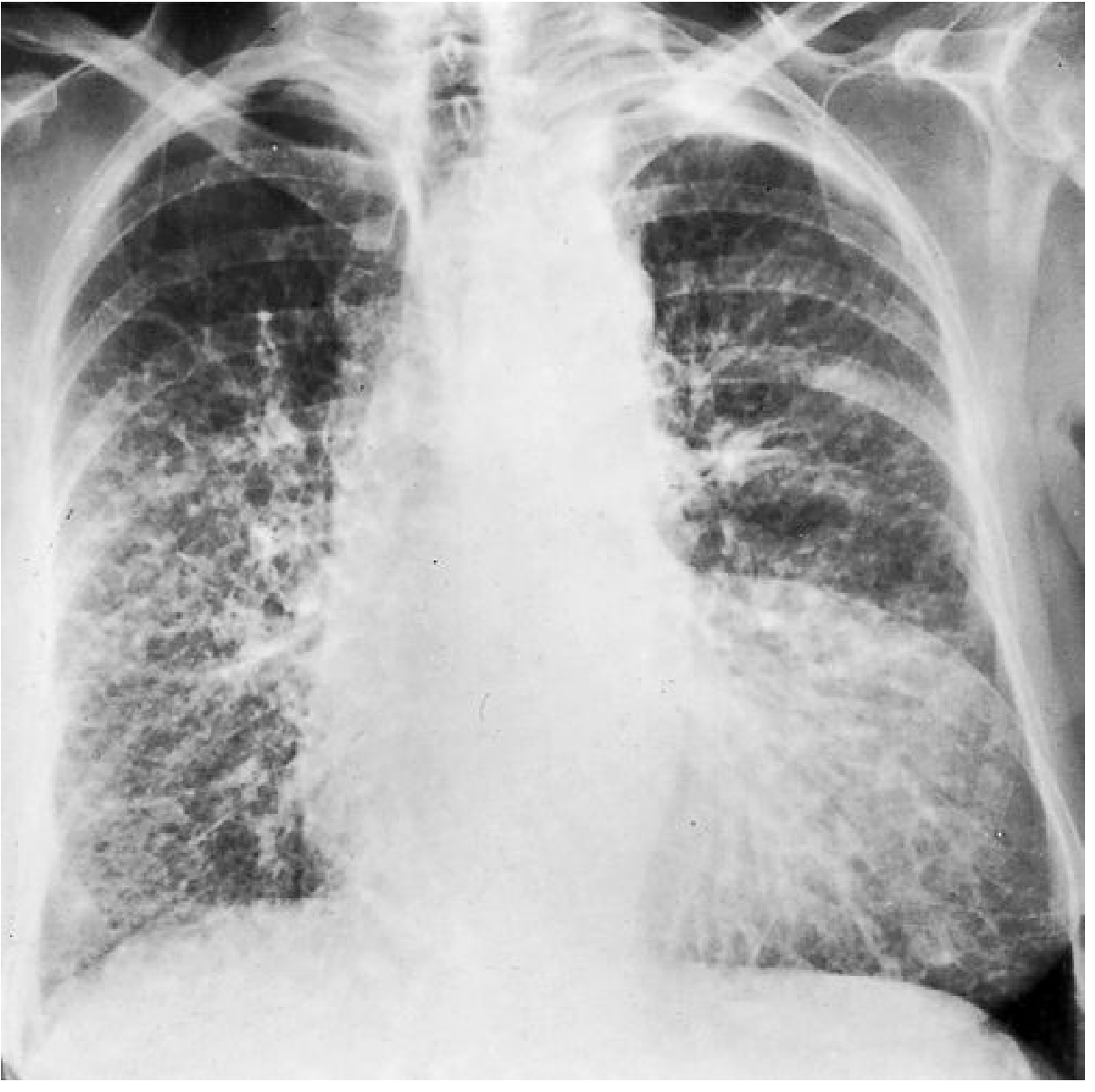
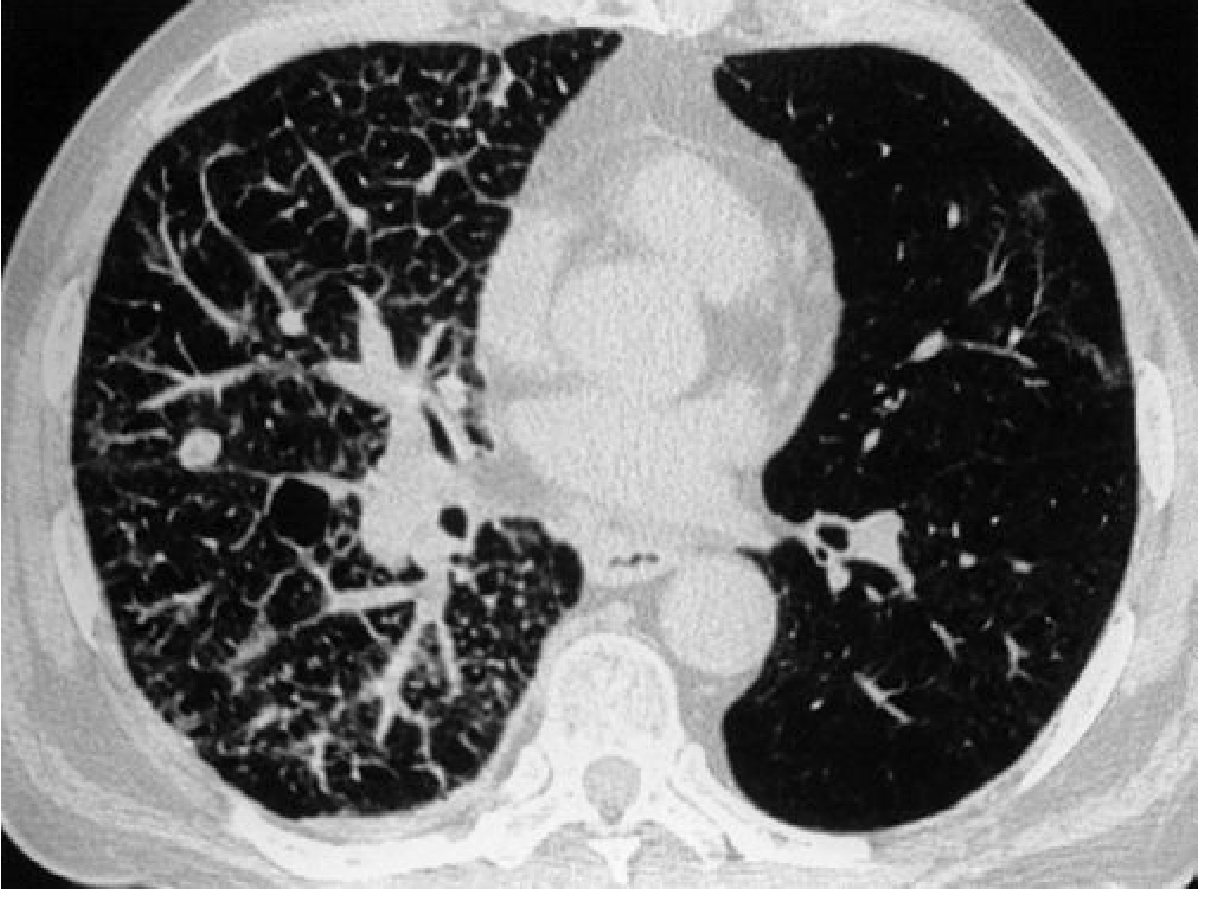
3. Lymphangitic Carcinomatosis
Permeation of pulmonary lymphatics and adjacent interstitial tissue by neoplastic cells.
Primary tumours: Carcinoma of bronchus, breast, stomach, and prostate.
Mechanism:
- Bilateral symmetric pattern - from haematogenous emboli spreading via vessel walls into perivascular interstitium
- Unilateral/localised pattern - from direct hilar node extension or pleural invasion
Radiological findings:
| Modality | Findings |
|---|---|
| CXR | Fine reticulonodular shadowing; thickened septal (Kerley B) lines; fissure thickening (subpleural oedema); pleural effusion (~30%) |
| HRCT | Non-uniform, nodular thickening of interlobular septa; irregular thickening of bronchovascular bundles centrally; scattered parenchymal nodules; patchy airspace shadowing; aerated acini subtended by thickened septa (key difference from pulmonary oedema) |
Key differentiating point from pulmonary oedema on HRCT: Many acini subtended by the thickened septa remain normally aerated in lymphangitic carcinomatosis.

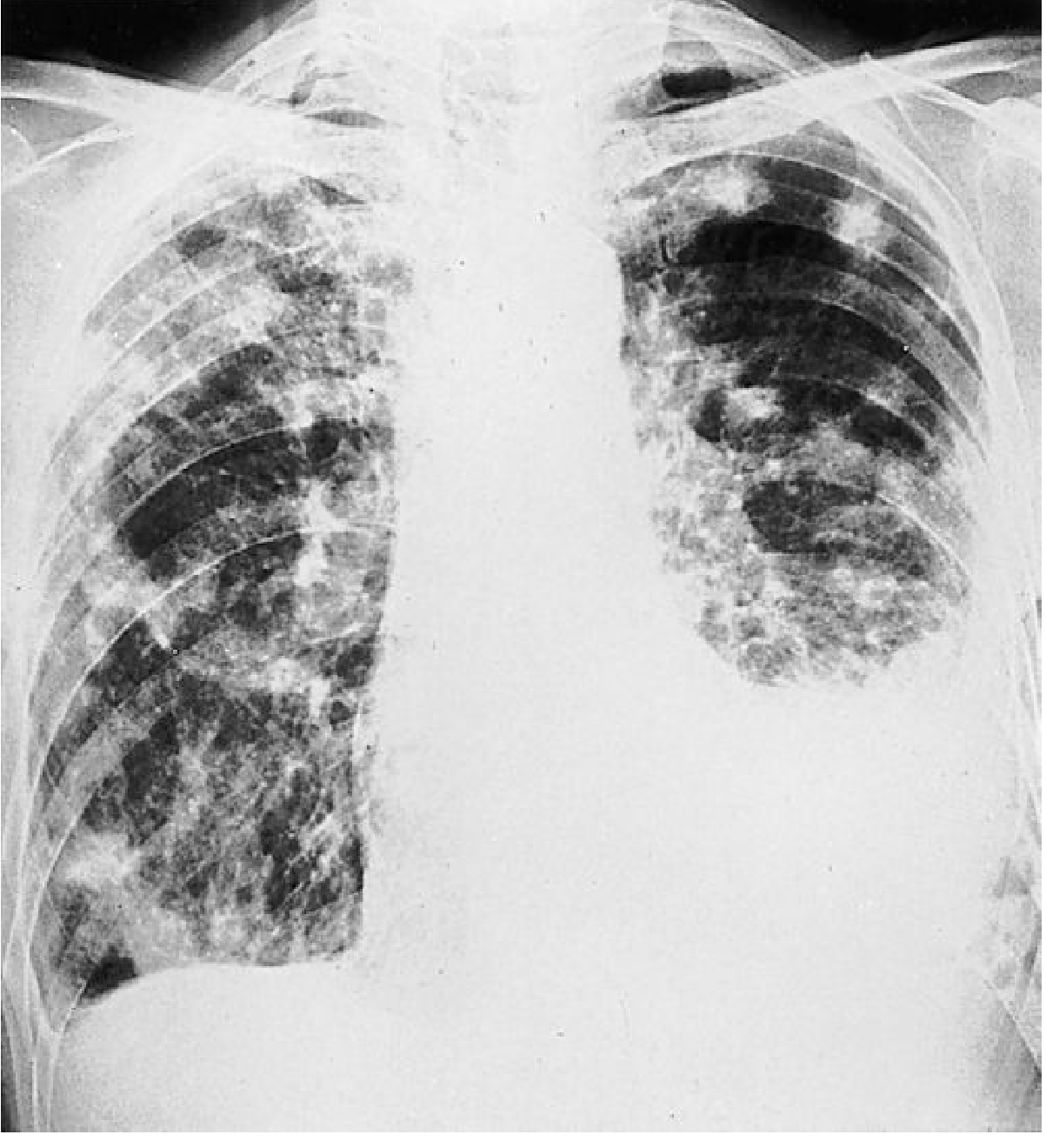
4. Miliary Metastases
- Innumerable tiny nodules mimicking miliary tuberculosis throughout both lungs
- No large masses, no lymphatic obstruction
- Rarest pattern of metastatic spread
- Primary tumours: thyroid carcinoma, renal carcinoma, bone sarcomas, choriocarcinoma
5. Endobronchial Metastases
- Rare; submucosal deposits cause airway obstruction as dominant radiological feature
- Leads to collapse, consolidation, or obstructive pneumonitis distal to the deposit
- Primary tumours: melanoma, renal, colorectal, breast carcinoma
6. Tumour Emboli
- Radiologically recognisable pulmonary arterial hypertension from tumour emboli blocking small pulmonary arteries
- Tumours: hepatoma, breast, kidney, stomach, prostate, choriocarcinoma
- Rare but high-yield PG MCQ association
7. Pleural Effusion
- Pleural effusion may accompany any pattern
- Especially common with lymphangitic spread (~30%)
- May also result from lymphatic obstruction, direct pleural seeding, or hypoalbuminaemia
Summary Table - High-Yield for PG Exam
| Pattern | Key Primary Tumours | Key Radiological Clue |
|---|---|---|
| Multiple discrete nodules | Breast, kidney, colon, sarcoma | Peripheral, basal, bilateral, well-defined |
| Cannon-ball | RCC, testis, choriocarcinoma | Large rounded bilateral nodules |
| Cavitating nodule | Squamous cell carcinoma | Thick-walled cavity |
| Calcified nodule | Osteosarcoma, chondrosarcoma | Dense calcification in nodule |
| Lymphangitic carcinomatosis | Breast, stomach, prostate, bronchus | Kerley B lines + reticulonodular shadowing; HRCT = septal thickening |
| Miliary | Thyroid, RCC, choriocarcinoma | TB-like tiny bilateral nodules |
| Endobronchial | Melanoma, RCC, colorectal, breast | Collapse/consolidation distal to obstruction |
| Tumour emboli | Hepatoma, choriocarcinoma | Pulmonary hypertension pattern |
Role of Imaging Modalities
- CXR (PA + lateral, high-kV): First-line; detects nodules >1 cm; misses lesions behind cardiac shadow, diaphragm, hilum
- MDCT: Detects lesions >3 mm; gold standard for staging and follow-up; essential for lymphangitic pattern (HRCT)
- PET-CT: FDG uptake; best for detecting distant metastases and monitoring treatment response
- MRI: Not routine for pulmonary metastases; useful for chest wall/pleural invasion assessment
Solitary Pulmonary Nodule in a Known Malignancy
Features favouring metastasis:
- Smooth, round borders on CT
- Temporal proximity to the primary lesion
- History of RCC, sarcoma, germ cell tumour
Features favouring new primary lung cancer:
- Spiculated edge
- History of head and neck (94%), lung (92%), bladder (89%), or uterine (74%) carcinoma - these carry highest risk of new primary
Schwartz's Principles of Surgery, 11e, p. 19-16
Sources:
- Grainger & Allison's Diagnostic Radiology, Chapter 8 (Lung Metastases, Lymphangitic Carcinomatosis, Unusual Patterns)
- Schwartz's Principles of Surgery, 11e, Chapter 19 (Metastatic Lesions to the Lung)
This is a shared conversation. Sign in to Orris to start your own chat.