Here is your comprehensive neurosurgery preparation guide — instruments (simple to complex) and landmark trials, with images throughout.
🧠 NEUROSURGERY INSTRUMENTS — Simple to Complex
PART 1: BASIC / GENERAL INSTRUMENTS
1. Scalpel Handle (Bard-Parker Handle)
Category: Cutting & Dissecting
- Handle types: No. 3 (for blades 10, 11, 12, 15) and No. 4 (for larger blades 20–22)
- Used for skin incisions, fascial cuts, and scalp opening
- Blade No. 15 is most commonly used in neurosurgery for its precision
- Reference: The Neurosurgical Instrument Guide (Neupsy Key, Ch. 4)
2. Monopolar Electrocautery (Bovie)
Category: Cautery
- Also called: bovie, electric knife, cauterizer
- Uses high-frequency electrical current to coagulate or cut tissue
- Essential for scalp hemostasis
- Important: Avoid near neural structures — use bipolar instead
3. Raney Scalp Clips
Category: Hemostasis
- Spring-loaded clips applied to the skin edges after scalp incision
- Control scalp bleeding by compressing the diploic vessels
- Available in standard and pediatric sizes
4. Tissue Forceps (Adson / DeBakey)
Category: Grasping
- Adson (toothed): holds scalp and dura
- DeBakey (non-toothed): handles delicate tissues
- Used throughout the procedure for tissue manipulation
5. Needle Holder
Category: Suturing
- Standard (Mayo-Hegar) or neurosurgical design
- Holds curved suturing needles for dural closure, scalp closure
- Bayonet-shaped versions used for deep microscopic suturing
PART 2: POSITIONING & HEAD FIXATION
6. Mayfield Skull Clamp (Three-Pin Fixator)
Category: Head Fixation
- Rigid cranial stabilization device with 3 skull pins
- Essential for all intracranial procedures — prevents any head movement
- U-shaped metallic frame with adjustable knurled pressure knobs
- Pins penetrate scalp and outer cortex of skull
Mayfield three-pin skull clamp for rigid head fixation — standard for cranial and posterior fossa surgery
7. Sugita Head Frame / Radiolucent Head Ring
Category: Head Fixation
- Alternative fixation allowing intraoperative fluoroscopy without artefact
- Radiolucent carbon fiber options available
PART 3: CRANIAL ACCESS INSTRUMENTS
8. Hudson Brace (Hand Drill)
Category: Drilling (Manual)
- Manual cranial perforator — no power source required
- Used in settings without powered drills or emergencies
- Works with perforator bits and burrs
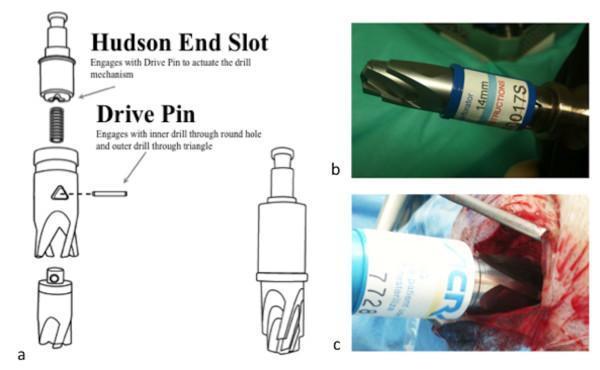
9. Perforator / Trephine
Category: Drilling
- Creates the initial burr hole in the skull
- Has a safety clutch mechanism that disengages when inner table is penetrated — prevents plunging into dura
Cranial perforator: (A) clutch mechanism diagram, (B) 14mm metallic bit, (C) intraoperative use during burr hole placement
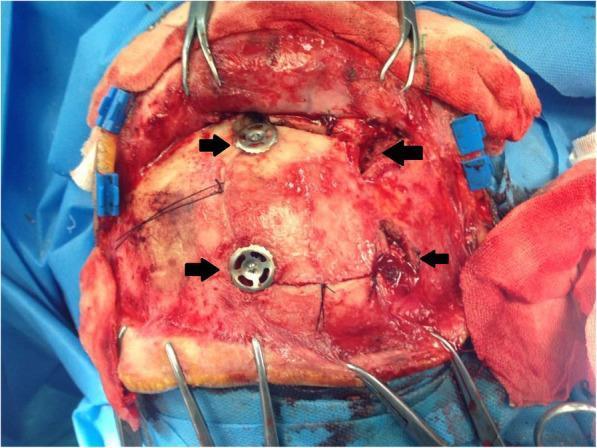
10. Galt Skull Trephine / Cortical Bone Trephine
Category: Drilling
- Circular saw for cutting round discs from skull
- Used for "keyhole" approaches and burr hole closure plugs
Four burr holes placed for bone flap craniotomy — standard technique for frontal craniotomies
11. Powered Craniotome (e.g., Midas Rex, Aesculap ELAN)
Category: Power Drill
- High-speed electric or pneumatic drill
- Attachments include:
- Craniotome (footplate saw): cuts between burr holes to create bone flap
- Barrel/Diamond burr: for fine bone drilling near dura/nerves
- Rosen burr: for general bone work
- WFNS standard equipment for all neurosurgical centers
12. Gigli Saw + Handles
Category: Bone Cutting
- Flexible wire saw passed through a burr hole guide
- Used to connect burr holes and free the bone flap
- Older technique largely replaced by powered craniotomes but still used when needed
13. Rongeurs (Bone Punches)
Category: Bone Removal
Multiple types used in neurosurgery:
| Rongeur Type | Use |
|---|
| Leksell Rongeur | Heavy-duty bone removal in laminectomy |
| Kerrison Rongeur | Thin footplate for narrow spaces; spinal canal decompression |
| Cushing Pituitary Rongeur | Pituitary/skull base bone biting |
| Love-Gruenwald Rongeur | Disc fragments and pituitary work |
| Hajek-Kofler Rongeur | Small bone piece removal from vertebrae |
PART 4: RETRACTORS
14. Brain Retractors (Yasargil / Leyla)
Category: Brain Retraction
- Malleable metal blades of varying widths (4mm, 6mm, 10mm, 17.5mm)
- Mounted on a flexible arm system (Leyla/Sugita bar) fixed to the table
- Used to gently hold brain tissue aside for deep exposure
- Important principle: Minimum retraction pressure to avoid retraction injury
15. Self-Retaining Retractors
Category: Soft Tissue Retraction
- Beckman-Eaton Retractor: laminectomy with hinged sharp-toothed blades
- Harvey-Jackson Retractor: spinal surgery
- Caspar Retractor: cervical spine
16. D'Errico-Adson Cerebellar Retractor
Category: Retraction
- 4×4 prongs, slightly angled
- Holds cerebellum during posterior fossa surgery
- Heavier than standard Adson forceps
PART 5: HEMOSTASIS & VASCULAR INSTRUMENTS
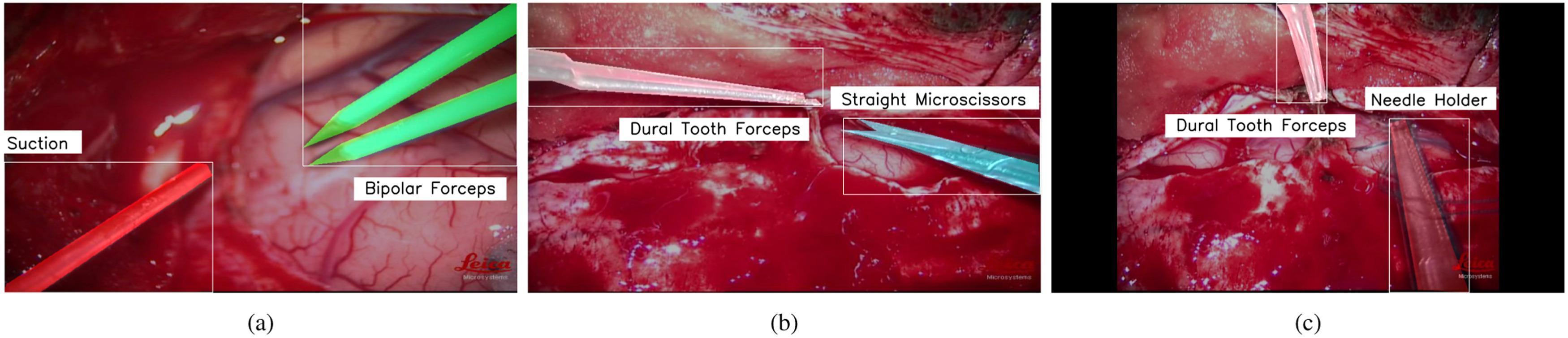
17. Bipolar Forceps (Malis / Yasargil)
Category: Bipolar Electrocautery — THE most important neurosurgical instrument
- Current passes only between the two tips — no spread to surrounding tissue
- Essential for coagulating vessels on the brain surface and in deep dissection
- Available in straight, bayonet, and angled configurations
- Tip sizes range from 0.3mm (micro) to 2mm
- Malis bipolar: most widely used; variable irrigation built in
Intraoperative segmentation: (a) suction tube (red) + bipolar forceps (green), (b) dural forceps + microscissors, (c) needle holder during dural suture
18. Aneurysm Clips
Category: Vascular Occlusion
- Permanent titanium or cobalt-alloy clips applied across aneurysm necks
- Types:
- Yasargil clips (most widely used): straight, curved, angled, fenestrated
- Sugita clips: strong closing force
- Scoville clips: older generation
- Applied with a clip applier (pistol-grip handle)
- Fenestrated clips: encircle a vessel while clipping the aneurysm
- Must be MRI-compatible (titanium)
Axial CT: hyperdense metallic aneurysm clip at the suprasellar region after ACoA aneurysm clipping
19. Micro-forceps (Bayonet Shaped)
Category: Microsurgical Grasping
- Bayonet design keeps hands out of the microscope's line of sight
- Toothed (0.5mm teeth) or non-toothed tips
- Used for dura, arachnoid, and tumour tissue handling
20. Suction Devices (Frazier / Yasargil)
Category: Suction
- Frazier suction tip: angled, with finger-controlled vent hole; most versatile
- Yasargil suction: used in microsurgery, thinner calibre
- Essential for maintaining bloodless field and aspirating CSF/blood
- Elsberg cannula and Adson cannula for ventricular access
PART 6: DISSECTION INSTRUMENTS
21. Periosteal Elevators (Cobb / Langenbeck)
Category: Bone Exposure
- Strips periosteum off skull/spine during exposure
- Raspatory (Langenbeck): scrapes bone surface
22. Dissectors / Microsurgical Dissectors
Category: Microsurgical Dissection
- Ball-tipped dissectors: gentle arachnoid and tumour dissection
- Penfield dissectors (No. 1–5): classic set for opening planes, coagulating vessels
- Rhoton dissectors: set of 8, gold standard for microscopic dissection
23. Microscissors
Category: Cutting (Microsurgical)
- Straight, curved, or angled; spring-handle design
- Used under microscope for arachnoid dissection, vessel work, tumour cutting
- Tenotomy scissors used for superficial dissection
24. Nerve Hook / Dura Hook
Category: Neural Dissection
- Krayenbuehl nerve hook: ball-tip for manipulating and lifting nerves
- Dura hook: elevates dura before incision
PART 7: BONE WORK — SPINAL
25. Kerrison Rongeur (Bone Punch)
Category: Spinal Decompression
- Most important spinal instrument
- Available in 1mm, 2mm, 3mm, 4mm, 5mm footplate sizes; up-biting or side-biting
- Used for laminectomy, foraminotomy, discectomy access
26. Pituitary Rongeurs (Love-Gruenwald / Cushing)
Category: Disc/Tumour Biting
- Grasping and removing disc material, pituitary tumour fragments
- Up-angled or straight jaws; various bite sizes
27. Inge Lamina Spreader / Caspar Retractor
Category: Spinal Distraction
- Spreads interlaminar space or disc space
- Caspar pins + distractor for cervical spine work
28. Osteotomes & Chisels (Neuro-Chisels)
Category: Bone Cutting
- Wire-type neuro-chisels: scrape, split, contour bone
- Used with mallet for skull base procedures
PART 8: COMPLEX / ADVANCED INSTRUMENTS
29. Ultrasonic Aspirator (CUSA — Cavitron Ultrasonic Surgical Aspirator)
Category: Tumour Resection
- Uses ultrasonic vibrations (23 kHz) to emulsify tumour tissue
- Simultaneously irrigates and aspirates the emulsified tissue
- Preserves blood vessels and nerves (higher tensile strength than tumour)
- Ideal for: gliomas, meningiomas, acoustic neuromas, spinal cord tumours
- Settings adjustable: aspiration, irrigation, ultrasonic power
CUSA being used for internal tumour debulking during L3-L4 schwannoma resection — capsular plane preserved
30. Neuronavigation (StealthStation / Brainlab Cranial)
Category: Image Guidance
- Frameless stereotactic system using pre-op MRI/CT
- Infrared or electromagnetic tracking of surgical instruments
- Real-time display of instrument position on 3D reconstructed imaging
- Used for: tumour approach planning, electrode placement, biopsy
31. Intraoperative Ultrasound (iUSG)
Category: Real-Time Imaging
- Probe placed directly on brain/dura during surgery
- Identifies tumour margins, residual tumour, ventricular position
- B-mode and Doppler modes available
- Immediate, no radiation, real-time feedback
32. Tubular Retractor / Neuroendoport (BrainPath, NICO Mysis)
Category: Minimally Invasive Access
- Cylindrical retractor inserted through small craniotomy
- Distributes retraction pressure evenly, reducing cortical injury
- Creates a surgical corridor to deep lesions (thalamus, basal ganglia, ventricles)
- Works with endoscope or microscope for visualization
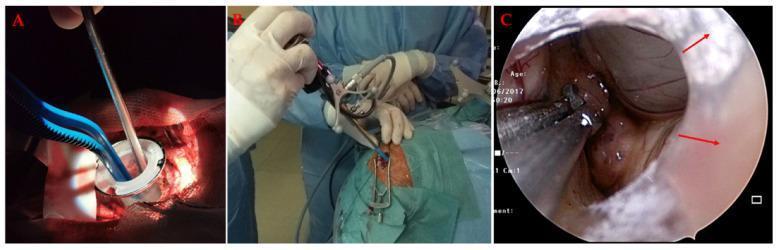
Neuroendoport: (A) tubular retractor through craniotomy with bipolar and aspirator, (B) endoscope introduction, (C) intraventricular tumour resection endoscopic view
PART 9: ENDOSCOPES IN NEUROSURGERY
33. Rigid Neuroendoscope (Karl Storz / Gaab Ventriculoscope)
Category: Endoscopy
- 0°, 30°, 70° angle of view scopes
- 6mm outer diameter typically; working channel for instruments
- Used for:
- ETV (Endoscopic Third Ventriculostomy) — treatment of obstructive hydrocephalus
- Choroid plexus cauterization (CPC)
- Intraventricular tumour biopsy/resection
- Colloid cyst removal
- Aqueductoplasty
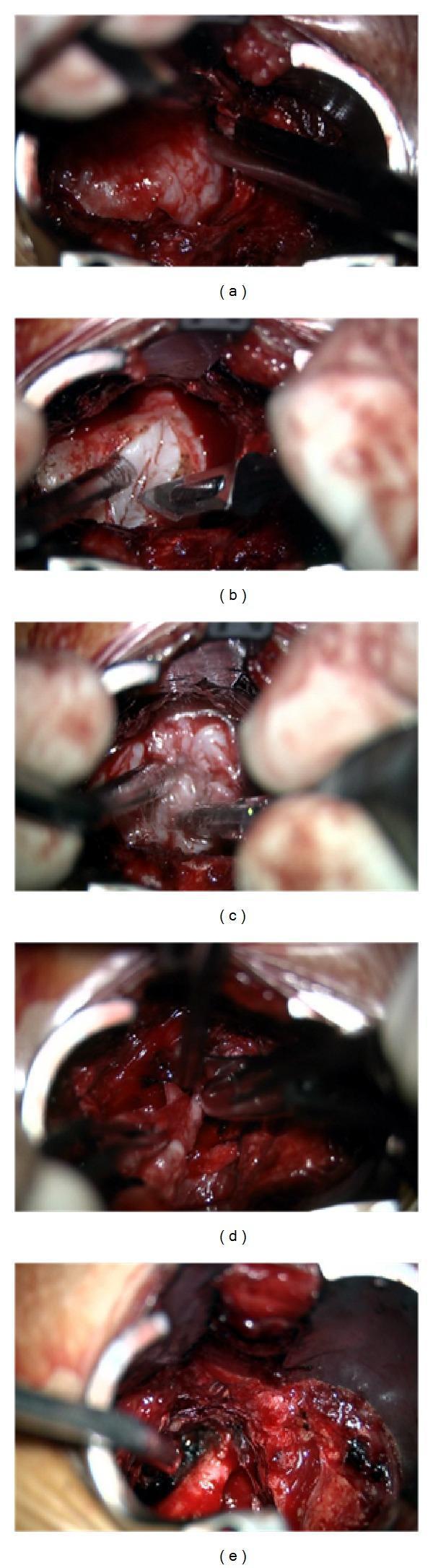
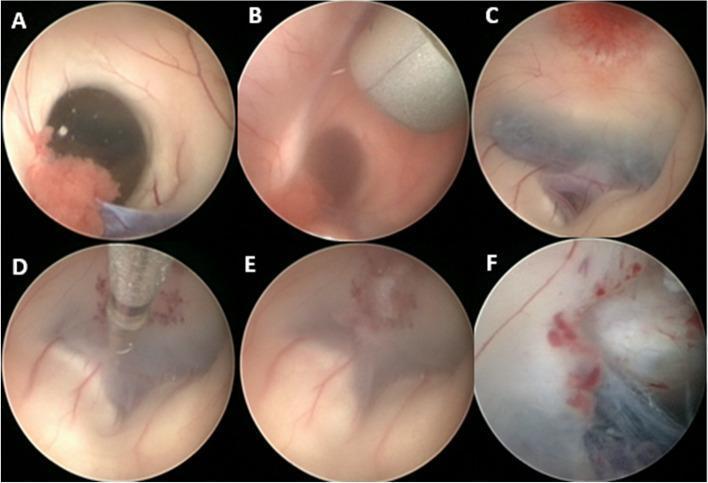
ETV: (A-B) external view of ventriculoscope advancing through foramen of Monro; (C) third ventricle floor; (D) forceps creating ostium; (E) completed fenestration; (F) Liliequist membrane opening
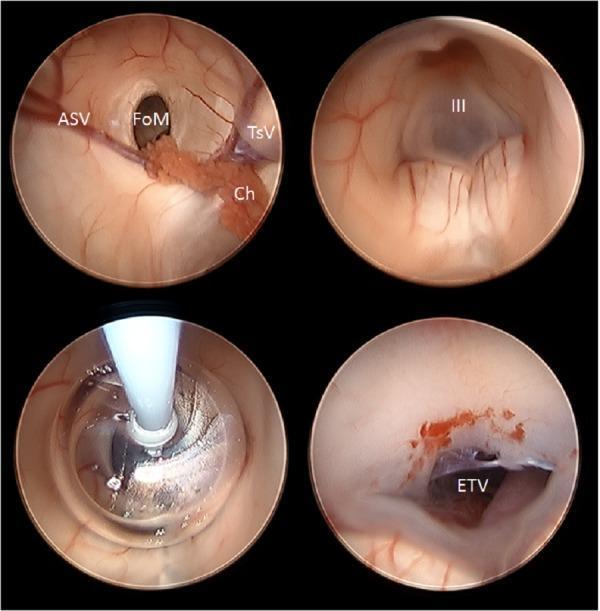
ETV steps: landmark identification at FoM, floor visualization, NeuroBalloon dilation, completed stoma
34. Flexible Neuroendoscope
Category: Endoscopy
- Steerable tip for navigating complex ventricular anatomy
- Used in multiloculated hydrocephalus, ventricular septations
- Combined with rigid scope (biportal technique)
35. Endonasal Endoscope (Extended Endoscopic Skull Base)
Category: Endoscopy — Skull Base
- 4mm, 18cm working length rigid scope (0° and 30°)
- Fully endoscopic transsphenoidal pituitary surgery (replaced microscopic TSS at most centres)
- Extended approaches: tuberculum sellae, clival, cribriform plate
- Working instruments: curved curettes, angled pituitary rongeurs, endonasal bipolar, micro-Doppler
- Advantages: panoramic view, no lip/nose retraction, bilateral nostril approach
36. Keyhole Endoscopy / Eyebrow Approach
Category: Minimally Invasive Cranial
- Small (25×15mm) supraorbital craniotomy
- Endoscope provides wide-angle visualization despite small opening
- Limitations: instrument crowding with robotic platforms
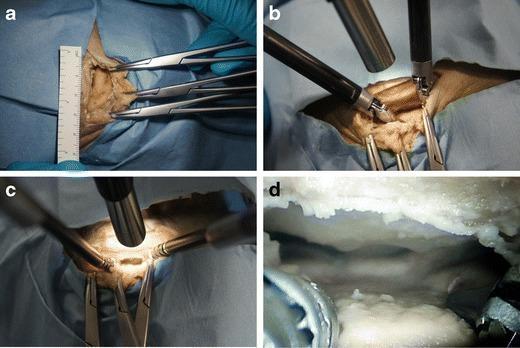
Keyhole craniotomy (25×15mm): (a) initial defect, (b-c) instrument crowding with robotic endoscopes, (d) restricted visualization when endoscope placed external to craniotomy
PART 10: OPERATING MICROSCOPES
37. Surgical Microscope (Zeiss OPMI Pentero / Kinevo 900; Leica M530)
Category: Visualization — The most important neurosurgical tool
- Provides 5–25× magnification for microsurgery
- Coaxial illumination — light travels exactly along the line of sight
- Features:
- Motorized zoom, focus, X-Y positioning
- Mouthswitch / footswitch control — hands-free operation
- Integrated fluorescence modules:
- 5-ALA (BLUE 400) fluorescence for glioma resection
- ICG (indocyanine green) for vessel/bypass patency
- Heads-up display with neuronavigation overlay
- Dual-surgeon heads (observer tube)
- Zeiss Kinevo 900: robotic-assisted microscope with 3D visualization and QEVO mode (non-contact microscopium at various magnifications)
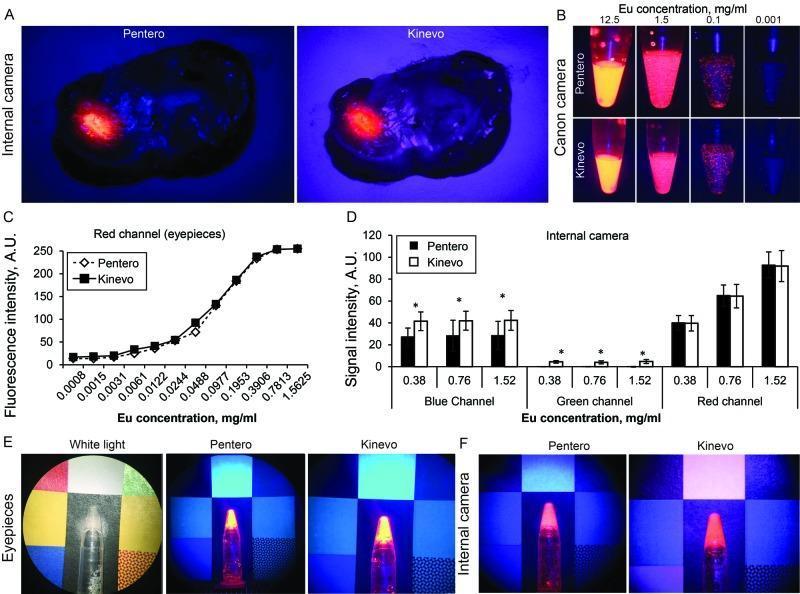
Zeiss Pentero vs Kinevo 900: Section A = mouse brain tumour under BLUE 400 mode; Section B-D = dye vial comparisons showing Kinevo's enhanced blue/green channel performance
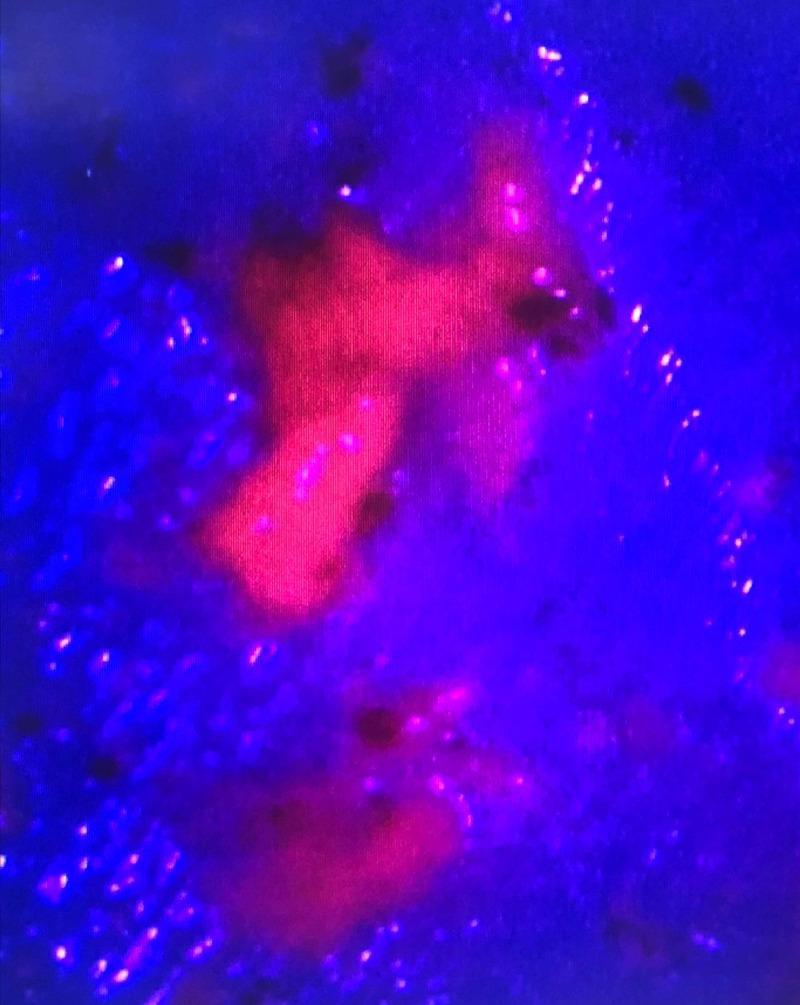
5-ALA guided surgery: intense pink-red fluorescence from high-grade glioma (PpIX accumulation), normal brain appears deep blue under 410nm excitation
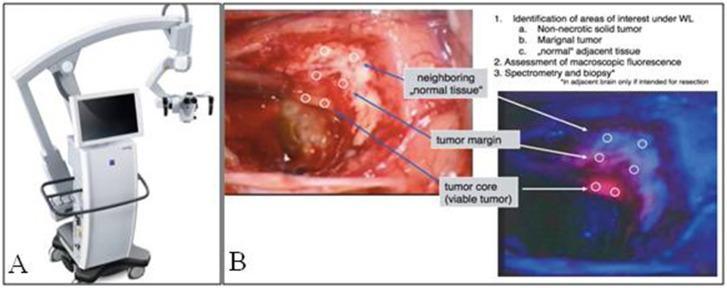
Fluorescence-guided surgery: white light (tumour margin unclear) vs 5-ALA fluorescence (tumour core bright red, infiltrative margin dimmer, normal tissue blue)
38. 3D Exoscope (VITOM 3D / Synaptive Modus V)
Category: Visualization (Advanced)
- Camera mounted on robotic arm above surgical field — replaces microscope
- Surgeon views on a 3D monitor with polarized glasses
- Wide 16:9 field of view; ergonomic advantages (no leaning into eyepieces)
- Supports 4K and 3D recording for teaching
- Fluorescence modules available
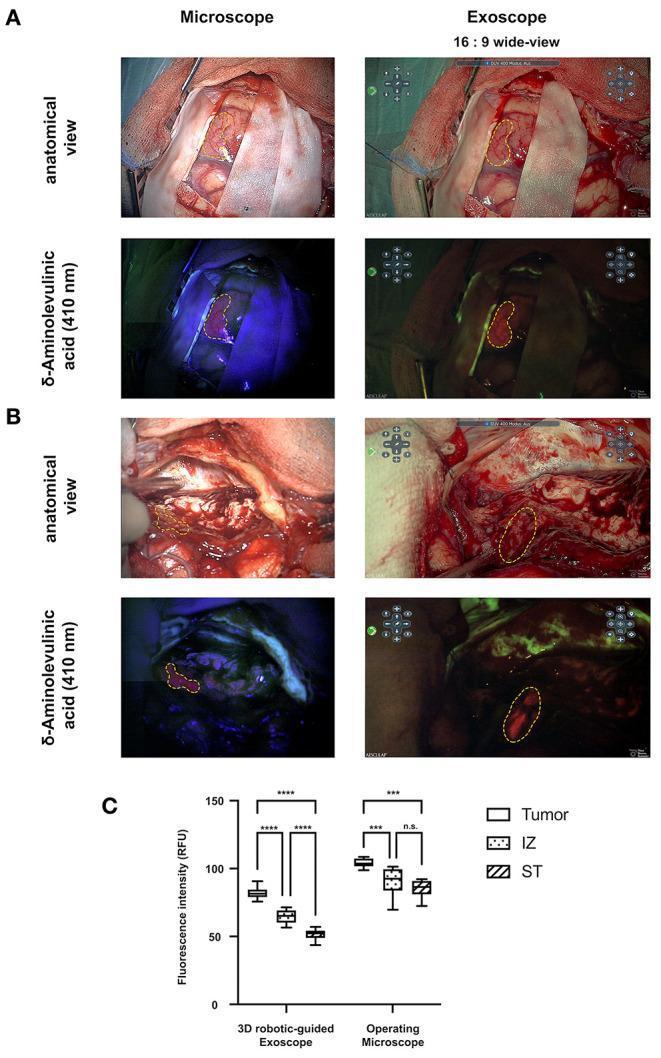
- Limitation: lower fluorescence intensity vs microscope (see Zeiss Pentero comparison above)
Exoscope vs OM: wide-field 16:9 digital view (exoscope) vs higher fluorescence intensity in OM; quantitative fluorescence comparison in tumour, infiltration zone, and normal tissue
PART 11: SPECIALIZED INSTRUMENTS
39. Stereotactic Frame (Leksell / CRW)
Category: Stereotaxy
- Attaches to skull with 4 pins; creates a 3D coordinate reference
- Used for:
- Stereotactic biopsy (target accuracy <1mm)
- DBS (deep brain stimulation) lead placement
- Radiosurgery (Gamma Knife requires Leksell frame)
40. DBS Electrode & Implantable Pulse Generator
Category: Functional Neurosurgery
- Targets: subthalamic nucleus (STN), globus pallidus interna (GPi), VIM thalamus
- Placed with stereotactic frame + microelectrode recording (MER)
- Used for: Parkinson's, essential tremor, dystonia, OCD
41. Gamma Knife (Leksell Gamma Knife)
Category: Radiosurgery
- 192 cobalt-60 sources focused to a single isocenter
- Single-fraction radiosurgery — no incision
- Indications: acoustic neuroma, meningioma, brain metastases, AVM, trigeminal neuralgia
42. Intraoperative Neurophysiological Monitoring (IONM)
Category: Monitoring
- Instruments: MEP (motor evoked potential) electrodes, SSEP, EEG, EMG
- Real-time cortical/subcortical stimulation probe (e.g., Ojemann cortical stimulator)
- Essential for eloquent area surgery, spine deformity
43. Fluoroscopy C-Arm / O-Arm
Category: Intraoperative Imaging
- C-arm: 2D fluoroscopy for pedicle screw confirmation, shunt placement
- O-arm (Medtronic): 3D intraoperative CT — updates neuronavigation mid-surgery
🏆 IMPORTANT CLINICAL TRIALS IN NEUROSURGERY
SECTION A: CEREBROVASCULAR — HEMORRHAGE
1. STICH I (2005) — Lancet
Full name: Surgical Trial in Intracerebral Haemorrhage I
| Parameter | Detail |
|---|
| Question | Early surgery vs conservative treatment for spontaneous supratentorial ICH |
| Design | RCT; 1,033 patients, 83 centres, 27 countries |
| Result | No significant benefit of early surgery overall (GOS at 6 months) |
| Subgroup | Superficial (lobar) haematomas with no IVH showed trend toward benefit |
| Outcome measure | Glasgow Outcome Scale |
| Conclusion | Initial conservative treatment is reasonable for most supratentorial ICH |
2. STICH II (2013) — Lancet
| Parameter | Detail |
|---|
| Question | Early surgery for lobar ICH (superficial, no IVH) vs initial conservative |
| Design | RCT; 601 patients |
| Result | No significant benefit overall, BUT a predefined "within-protocol" analysis showed favour for surgery in patients with poor prognosis |
| Significance | Confirmed that lobar ICH without IVH may have marginal surgical benefit |
| Modern impact | Led to MISTIE III and ENRICH trials targeting minimally invasive evacuation |
3. MISTIE III (2019) — Lancet
| Parameter | Detail |
|---|
| Question | Minimally invasive surgery + rt-PA for ICH evacuation |
| Result | Mortality benefit confirmed; functional improvement when clot reduced to <15mL |
| Instrument | Stereotactic catheter + thrombolytic |
4. DECRA (2011) — NEJM
Full name: Decompressive Craniectomy Trial for Diffuse TBI
| Parameter | Detail |
|---|
| Question | Bifrontal decompressive craniectomy vs standard care for refractory ICP in TBI |
| Design | RCT; 155 patients |
| Result | Craniectomy reduced ICP but led to worse functional outcomes (GOSE) |
| Conclusion | Decompressive craniectomy for diffuse TBI does not improve functional outcome and may increase unfavourable outcomes |
5. RESCUEicp (2016) — NEJM
| Parameter | Detail |
|---|
| Question | Decompressive craniectomy vs medical treatment for refractory ICP in TBI |
| Design | RCT; 408 patients |
| Result | Craniectomy reduced mortality (26.9% vs 48.9%) but increased vegetative state rates; more patients survived with disability |
| Conclusion | Craniectomy is life-saving but survivors more likely to be severely disabled or vegetative — informed consent critical |
SECTION B: CEREBROVASCULAR — ANEURYSM & AVM
6. ISAT (2002, updated 2005) — Lancet ⭐ Most cited neurosurgery trial
Full name: International Subarachnoid Aneurysm Trial
| Parameter | Detail |
|---|
| Question | Endovascular coiling vs neurosurgical clipping for ruptured intracranial aneurysms |
| Design | RCT; 2,143 patients, 42 centres (UK/Europe) |
| Primary outcome | Death or dependency (mRS 3–6) at 1 year |
| Result | Coiling: 23.7% dead/dependent vs Clipping: 30.6% — 7.4% absolute risk reduction (p=0.0001) |
| 7-year follow-up | Survival advantage maintained; higher epilepsy risk with clipping; higher rebleed risk with coiling |
| Limitation | Only aneurysms deemed suitable for BOTH techniques enrolled |
| AHA Guideline | For aneurysms amenable to both, endovascular coiling should be considered (Class I, Level B) |
7. BRAT (2012) — J Neurosurg
Full name: Barrow Ruptured Aneurysm Trial
| Parameter | Detail |
|---|
| Question | Microsurgical clipping vs coil embolization for ruptured cerebral aneurysms |
| Design | RCT; 470 patients; single centre (Barrow Neurological Institute) |
| Result | Coiling: fewer poor outcomes at 1 year (mRS >2: 23.2% vs 33.7% for clipping) |
| 6-year follow-up | Outcomes equalized — no significant difference at long-term follow-up |
| Rebleed | Higher in coiling group |
| Significance | Complementary to ISAT; confirmed coiling short-term benefit but clipping durability advantage |
8. ARUBA (2014) — Lancet
Full name: A Randomized trial of Unruptured Brain AVMs
| Parameter | Detail |
|---|
| Question | Medical management alone vs interventional therapy for unruptured brain AVMs |
| Design | RCT; 226 patients, 39 sites, 9 countries; stopped early |
| Result | Medical management: 10.1% risk of stroke/death vs Intervention: 30.7% (HR 3.70, p<0.0001) |
| Conclusion | Medical management superior to interventional therapy for unruptured AVMs in the short term |
| Controversy | Short follow-up (33 months); natural history of AVM risk continues lifelong — long-term benefit of intervention may emerge |
SECTION C: ISCHEMIC STROKE — THROMBECTOMY
9. MR CLEAN (2015) — NEJM ⭐
Full name: Multicenter Randomized Clinical trial of Endovascular Treatment for Acute Ischemic Stroke in the Netherlands
| Parameter | Detail |
|---|
| Question | Endovascular thrombectomy (IA treatment) + standard care vs standard care alone for large vessel anterior circulation stroke |
| Design | RCT; 500 patients, 16 centres, Netherlands |
| Time window | Within 6 hours of symptom onset |
| Primary outcome | mRS at 90 days |
| Result | Functional independence 32.6% (intervention) vs 19.1% (control) — adjusted OR 1.67 |
| Significance | First Level 1A evidence for mechanical thrombectomy in large vessel stroke |
| Impact | Led to early termination of 4 other concurrent trials (ESCAPE, EXTEND-IA, REVASCAT, SWIFT PRIME) |
10. ESCAPE, EXTEND-IA, SWIFT PRIME, REVASCAT (2015) — NEJM
All confirmed MR CLEAN results — together they transformed stroke management:
- Number needed to treat (NNT): ~5 for one additional independent outcome
- All showed benefit of stentriever-based thrombectomy within 6h
- ESCAPE showed benefit up to 12h with good collaterals
11. DAWN (2018) & DEFUSE-3 (2017) — NEJM
| Parameter | Detail |
|---|
| Question | Thrombectomy in late window (6–24h for DAWN; 6–16h for DEFUSE-3) |
| Patient selection | Perfusion imaging mismatch (DWI/PWI or CT perfusion) |
| Result | Significant benefit maintained — extended window approved |
| Impact | Transformed stroke eligibility criteria worldwide |
SECTION D: SPINE
12. SPORT Trials (2006/2007) — NEJM ⭐
Full name: Spine Patient Outcomes Research Trial
| Trial | Condition | Finding |
|---|
| SPORT Disc | Lumbar disc herniation | Surgery shows greater early improvement; outcomes converge at 2 years as many conservatively treated patients improve |
| SPORT Spondylolisthesis | Lumbar degenerative spondylolisthesis | Surgery significantly superior to conservative at all time points; benefits sustained at 2 years |
| SPORT Stenosis | Lumbar spinal stenosis | Surgery superior for symptom relief vs non-operative at 2 years |
| Outcome measures | SF-36 (PCS/MCS), Oswestry Disability Index (ODI), VAS | |
| Key lesson | Surgical benefit most pronounced in intent-to-treat analysis for spondylolisthesis; contamination between groups in disc herniation RCT weakened significance | |
13. NECK Trial (Cervical Radiculopathy)
| Parameter | Detail |
|---|
| Focus | ACDF vs conservative management for cervical disc disease |
| Outcome | VAS pain scale; surgery shows faster resolution |
SECTION E: BRAIN TUMOURS
14. STUPP Protocol / EORTC 26981 (2005) — NEJM ⭐
Full name: EORTC-NCIC Trial for Glioblastoma
| Parameter | Detail |
|---|
| Question | Radiotherapy alone vs RT + concurrent/adjuvant temozolomide (TMZ) for newly diagnosed GBM |
| Design | RCT; 573 patients |
| Result | Median OS: 14.6 months (RT+TMZ) vs 12.1 months (RT alone); 2-yr survival 26.5% vs 10.4% |
| MGMT | MGMT promoter methylation predicts benefit from TMZ |
| Significance | Established standard of care for GBM: maximal safe resection + RT + TMZ |
15. 5-ALA (Stummer) Trial (2006) — Lancet Oncology
| Parameter | Detail |
|---|
| Question | 5-aminolevulinic acid (oral) guided resection vs white-light resection for GBM |
| Design | RCT; 322 patients |
| Result | 5-ALA group: 65% complete resection vs 36% white light (p<0.0001); 6-month PFS improved |
| Instrument impact | Established 5-ALA fluorescence as standard for GBM surgery |
| EU approval | 5-ALA (Gliolan) approved for malignant glioma resection |
16. RTOG 9802 (2012) — NEJM
| Parameter | Detail |
|---|
| Question | RT alone vs RT + PCV chemotherapy for high-risk low-grade glioma |
| Result | RT + PCV: median OS 13.3 years vs 7.8 years for RT alone |
| Significance | PCV chemotherapy adds significant survival benefit in IDH-mutant low-grade glioma |
17. NORDnordic Trial / INOVATYON (Elderly GBM)
- Hypofractionated RT (40Gy/15fr) equivalent to standard 60Gy in elderly patients
- TMZ alone non-inferior to RT alone in elderly unmethylated GBM
SECTION F: HYDROCEPHALUS & OTHER
18. MOMS Trial (2011) — NEJM
Full name: Management of Myelomeningocele Study
| Parameter | Detail |
|---|
| Question | Prenatal vs postnatal surgical repair of myelomeningocele |
| Design | RCT; 183 patients |
| Result | Prenatal repair: reduced need for VP shunting at 12 months (40% vs 82%); improved motor outcomes; increased maternal risk |
| Significance | Established fetal surgery for MMC as superior to postnatal repair |
| Recent review (PMID 41342964, 2025) | Confirms neurosurgical outcomes improvements with prenatal repair; evolving techniques |
19. CLEAR III (2017) — Lancet
| Parameter | Detail |
|---|
| Question | Intraventricular rt-PA via EVD for IVH |
| Result | Clot clearance improved but no significant difference in mRS at 180 days |
| Finding | Lower mortality and higher proportion of good outcomes in clot clearance subgroup |
SECTION G: FUNCTIONAL NEUROSURGERY
20. SANTE Trial (2010)
Full name: Stimulation of the Anterior Nucleus of the Thalamus for Epilepsy
| Parameter | Detail |
|---|
| Question | ANT-DBS for drug-resistant epilepsy |
| Result | 40.4% median reduction in seizure frequency vs 14.5% control |
| Approval | FDA-approved 2018 for partial-onset seizures |
21. Cavernous Sinus / Radiosurgery trials (LINAC, Gamma Knife for AN)
- CONSULT, CISRAF trials: SRS vs microsurgery for vestibular schwannoma (acoustic neuroma)
- SRS achieves tumour control in 90–95%; microsurgery offers definitive resection
- Facial nerve preservation equivalent in experienced centres
SUMMARY TABLE — Key Neurosurgery Trials
| Trial | Year | Topic | Key Finding |
|---|
| ISAT | 2002 | Ruptured aneurysm | Coiling > Clipping (7.4% ARR in death/dependency) |
| BRAT | 2012 | Ruptured aneurysm | Short-term coiling benefit; long-term outcomes equal |
| ARUBA | 2014 | Unruptured AVM | Medical Rx > Intervention (3.7× lower stroke/death risk) |
| MR CLEAN | 2015 | Ischemic stroke LVO | Thrombectomy: 32.6% vs 19.1% functional independence |
| DAWN/DEFUSE-3 | 2017-18 | Late-window stroke | Thrombectomy benefit extends to 24h with perfusion mismatch |
| STICH I | 2005 | ICH evacuation | No benefit of early surgery overall |
| STICH II | 2013 | Lobar ICH | Marginal benefit for superficial lobar ICH |
| DECRA | 2011 | TBI decompression | Craniectomy lowers ICP but worsens functional outcomes |
| RESCUEicp | 2016 | TBI decompression | Craniectomy reduces mortality; increases survival with disability |
| STUPP | 2005 | GBM | RT+TMZ standard of care; OS 14.6 vs 12.1 months |
| 5-ALA Trial | 2006 | GBM resection | 5-ALA: 65% vs 36% complete resection |
| SPORT | 2006-07 | Lumbar spine | Surgery > conservative especially for spondylolisthesis |
| MOMS | 2011 | Myelomeningocele | Prenatal repair reduces shunting need (40% vs 82%) |
| SANTE | 2010 | Epilepsy DBS | ANT-DBS: 40% seizure reduction |
Key Reference Sources Used
- WFNS Basic Sets of Neurosurgical Instruments (Aesculap/WFNS Official Document)
- The Neurosurgical Instrument Guide (Neupsy Key — Ellenbogen, Sekhar, Lam)
- Principles of Neurosurgery (Ellenbogen, Sekhar)
- Youmans and Winn Neurological Surgery, 7th Edition
- Crucial trials in neurosurgery — Neurosurgical Review, Springer Nature (2024)
- ISAT: Lancet 2002 (PMID 16139655)
- MR CLEAN: NEJM 2015
- MOMS follow-up SR: PMID 41342964 (2025)
Tip for exams: The ISAT trial, STUPP protocol, MR CLEAN, DECRA/RESCUEicp, ARUBA, and SPORT are the highest-yield trials. For instruments, focus on the bipolar forceps, Mayfield clamp, Malis dissectors, Yasargil aneurysm clips, CUSA, and the operating microscope as the cornerstones of modern neurosurgical practice.