Notes of skin layers all
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive content from multiple authoritative textbooks. Let me compile the complete notes on skin layers.
Skin Layers - Complete Notes
Overview
The skin (integument) is the body's largest organ, accounting for 15-20% of total body weight and presenting 1.5-2 m² of surface area. It consists of three main layers:
- Epidermis - outer epithelial layer (ectodermal origin)
- Dermis - underlying connective tissue layer (mesodermal origin)
- Subcutaneous tissue / Hypodermis - deepest layer of loose connective tissue and fat
1. EPIDERMIS
The epidermis is a stratified squamous keratinized epithelium composed mainly of keratinocytes, with three less abundant cell types: melanocytes, Langerhans cells, and Merkel cells.
- Thin skin (everywhere except palms/soles): epidermis is 75-150 μm thick
- Thick skin (palms and soles): epidermis is 400-600 μm thick
- Epidermis is avascular - cells receive nutrients by diffusion from dermis
- Turnover time: 15-30 days depending on age and body region
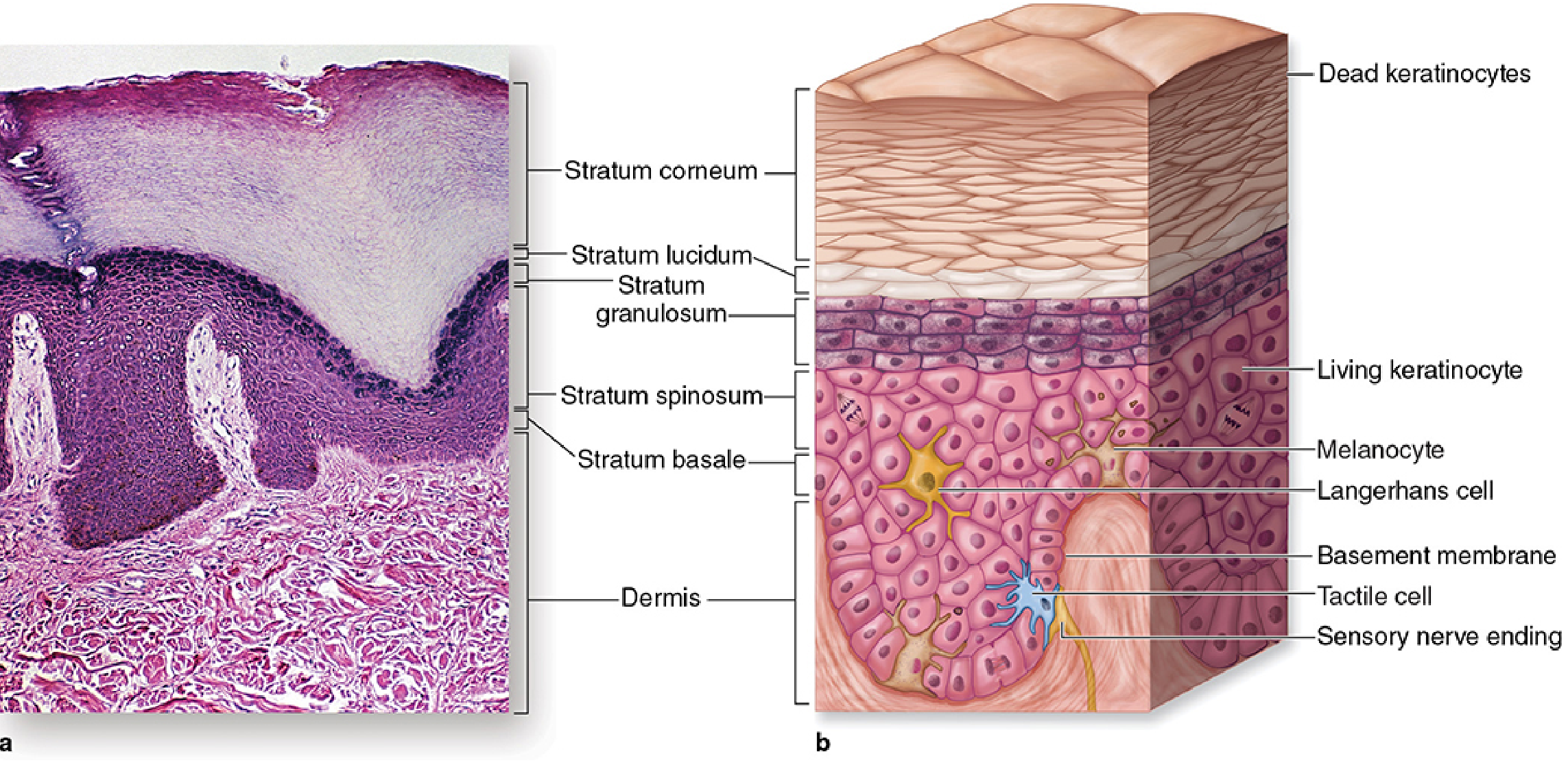
The 5 Layers (Strata) of the Epidermis
From deepest to most superficial (remember: "Come, Let's Get Sun-burned" or S-B-S-G-L-C):
Layer 1: Stratum Basale (Basal Layer)
Also called Stratum Germinativum
- Single layer of cuboidal to low columnar cells on the basement membrane
- Contains stem cells - intense mitotic activity
- Cells are basophilic (dark-staining due to closely spaced nuclei)
- Contains melanin granules transferred from neighboring melanocytes
- Keratinocytes connected to each other by desmosomes; attached to basal lamina by hemidesmosomes
- Begins synthesis of keratin intermediate filaments (~10 nm diameter)
- As new keratinocytes form, they migrate upward into the next layer
- Also houses Merkel cells (mechanoreceptors) and melanocytes
Layer 2: Stratum Spinosum (Spinous/Prickle Cell Layer)
- Several cells thick; cells are larger than basal cells
- Cells exhibit numerous cytoplasmic spines (short processes extending from cell to cell)
- Spines connected to adjacent cell spines by desmosomes
- The desmosome junction appears as a thickening called the node of Bizzozero
- Cells appear "spiny" in H&E because cells shrink during preparation, expanding intercellular spaces
- Continues synthesis of keratin filaments (tonofibrils)
- In the upper spinous layer, cells begin producing keratohyalin granules and lamellar bodies (membrane-coating granules containing glycolipids)
- Langerhans cells (antigen-presenting dendritic cells) are found here
Layer 3: Stratum Granulosum (Granular Layer)
- 3-5 cell layers thick
- Contains numerous intensely basophilic keratohyalin granules (visible by LM) - these contain filaggrin and loricrin
- Contains lamellar bodies (Odland bodies) - discharge their lipid contents into intercellular space forming the water barrier of skin
- Cells begin to exhibit apoptotic nuclear morphology (DNA fragmentation) - terminal differentiation
- pH is approximately neutral (~7.17)
- As cells move upward, nucleus and organelles break down
- The stratum lucidum exists just above this layer in thick skin only
Layer 4: Stratum Lucidum (Clear Layer)
Thick skin only (palms and soles)
- Thin, translucent, pale-staining band of flattened cells
- Limited to thick skin; considered a subdivision of the stratum corneum
- Cells lack nuclei and organelles; filled with eleidin (a transformation product of keratohyalin)
- Located between stratum granulosum and stratum corneum
Layer 5: Stratum Corneum (Cornified/Horny Layer)
- Outermost, most superficial layer
- Composed of dead, flat, anucleate keratinocytes completely filled with keratin filaments
- Cells are called corneocytes or squames
- Plasma membrane thickened and reinforced by cross-linked proteins (cornified envelope)
- Intercellular spaces filled with lipids discharged from lamellar bodies - forms the permeability barrier against water loss
- pH acidic: 4.5-6.0 at the surface (acid mantle)
- Cells are regularly shed (desquamation) via proteolytic degradation of desmosomes
- Controlled by kallikrein-related serine peptidases (KLK5, 7, 14) in a pH-dependent manner
- Inhibited by LEKTI (lymphoepithelial Kazal-type inhibitor, encoded by SPINK5) at neutral pH
- At acidic pH near surface, LEKTI releases KLKs, which degrade desmosomes, causing shedding
- Mutation in SPINK5 causes Netherton syndrome
Clinical note: Average stratum corneum thickness does not change with age, but barrier function declines. Skin of palms/soles may form corns and calluses from chronic friction.
Non-Keratinocyte Cells of the Epidermis
| Cell | Location | Origin | Function |
|---|---|---|---|
| Melanocytes | Stratum basale | Neural crest | Synthesize melanin (UV protection); transfer melanosomes to ~10-30 keratinocytes via dendritic processes |
| Langerhans cells | Stratum spinosum | Bone marrow (monocyte lineage) | Antigen-presenting cells (APCs); part of adaptive immunity |
| Merkel cells | Stratum basale | Neural crest | Low-threshold mechanoreceptors; sense gentle touch; synapse with unmyelinated afferent nerve fibers |
Melanin synthesis: Tyrosinase converts tyrosine → DOPA → melanin polymer. Melanin accumulates in melanosomes (Golgi-derived vesicles), which are transferred to keratinocytes.
2. DERMIS
The dermis is the layer of connective tissue supporting the epidermis, binding it to the subcutaneous tissue. It reaches up to 4 mm thick on the back.
Dermal-Epidermal Junction
- The dermis surface is very irregular, with dermal papillae that interdigitate with epidermal ridges/pegs
- Reinforces adhesion between layers, especially in skin under frequent pressure
- A basement membrane (containing type IV collagen, laminin) always lies between the basal epidermal layer and dermis
- Damage to the dermal-epidermal junction causes bullous pemphigoid (autoimmune); damage to intercellular keratinocyte junctions causes pemphigus
Two Sublayers of the Dermis
Papillary Layer (superficial)
- Thin, loose connective tissue
- Contains types I and III collagen fibers, fibroblasts, scattered mast cells, dendritic cells, and leukocytes
- Anchoring fibrils of type VII collagen insert into basal lamina to bind dermis to epidermis
- Rich in capillaries forming the subpapillary plexus just below epidermis
- Contains sensory nerve endings
Reticular Layer (deep)
- Much thicker; dense irregular connective tissue
- Mainly bundles of type I collagen (thicker and denser than papillary)
- Rich network of elastic fibers (providing skin elasticity)
- Abundant proteoglycans (rich in dermatan sulfate) among the fibers
- Fewer cells than papillary layer
- Damage to this layer results in permanent scarring
Aging changes: Thickening and cross-linking of collagen, loss of hyaluronan and GAGs, loss of elastic fibers (especially from UV exposure - "solar elastosis") causes skin fragility, loss of suppleness, and wrinkling.
Vascular Supply of the Dermis
- Subpapillary plexus - between papillary and reticular dermis; capillary branches extend into dermal papillae
- Deep plexus - near dermis-subcutaneous tissue interface; larger vessels
- Arteriovenous anastomoses (shunts) - between the two plexuses; regulate thermoregulation (constrict to conserve heat; dilate to lose heat)
Nerve Supply of the Dermis
- Sensory afferent fibers network in papillary dermis and around hair follicles
- Autonomic fibers supply smooth muscle of blood vessels and arrector pili muscles, and sweat glands
- Key receptors:
- Meissner's corpuscles - light touch (dermal papillae)
- Pacinian corpuscles - deep pressure and vibration (deep dermis/hypodermis)
- Ruffini endings - sustained pressure and skin stretch
- Free nerve endings - pain, temperature
3. SUBCUTANEOUS TISSUE (Hypodermis)
- Lies beneath the dermis
- Loose connective tissue + pads of adipocytes
- Binds skin loosely to underlying tissues (muscles, fascia)
- Corresponds to the superficial fascia of gross anatomy
- Functions:
- Energy storage (fat)
- Thermal insulation
- Mechanical cushioning (shock absorption)
- Route for blood vessels, lymphatics, and nerves entering the skin
Summary Table: Epidermal Layers
| Layer | # Cells | Key Features | Special Contents |
|---|---|---|---|
| Stratum basale | 1 layer | Mitosis, stem cells, columnar/cuboidal, basophilic | Melanocytes, Merkel cells, hemidesmosomes |
| Stratum spinosum | Several layers | Spiny processes, desmosomes, node of Bizzozero | Langerhans cells, lamellar bodies begin |
| Stratum granulosum | 3-5 layers | Keratohyalin granules (basophilic), water barrier forms | Lamellar bodies discharged |
| Stratum lucidum | Few layers | Translucent, no nuclei, eleidin | Thick skin ONLY |
| Stratum corneum | Many layers | Anucleate, fully keratinized, acid mantle (pH 4.5-6) | Corneocytes, keratin, lipid barrier |
Functions of Skin
| Function | Mechanism |
|---|---|
| Protection | Physical barrier, melanin (UV), immune cells (Langerhans cells), antimicrobial acid mantle |
| Sensory | Many mechanoreceptors, thermoreceptors, nociceptors |
| Thermoregulation | Sweat glands, dermal vasculature, AV shunts, subcutaneous fat insulation |
| Metabolic | Synthesis of Vitamin D3 (from UV action on precursor); fat storage |
| Water balance | Permeability barrier (lipids in stratum corneum) prevents excessive water loss |
| Immune | Langerhans cells, dermal dendritic cells, lymphocytes - innate and adaptive |
Sources:
- Junqueira's Basic Histology - Text and Atlas, 17e, Ch. 18 (Skin)
- Histology: A Text and Atlas with Correlated Cell and Molecular Biology
- Fitzpatrick's Dermatology, Vol. 1 & 2
- Dermatology 2-Volume Set, 5e
- K.J. Lee's Essential Otolaryngology (Skin Anatomy)
All about vicryl
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
I now have comprehensive data from multiple authoritative surgical and dermatology textbooks. Let me compile the complete notes.
Vicryl (Polyglactin 910) - Complete Notes
1. Basic Identity
| Property | Details |
|---|---|
| Generic name | Polyglactin 910 |
| Brand names | Vicryl®, Polysorb® (also Novosyn®) |
| Manufacturer | Ethicon Inc. (Johnson & Johnson) |
| Year introduced | 1974 |
| Class | Synthetic, braided, absorbable suture |
| Material | Copolymer of glycolide (90%) and L-lactide (10%) |
| Coating | Polyglactin 370 + calcium stearate (lubricant to ease passage through tissue) |
2. Chemical Composition
- Copolymer of lactide and glycolide in a ratio of 90:10
- The water-repelling properties of the lactide component delay penetration of water and slow the loss of tensile strength compared to polyglycolic acid (Dexon)
- Coating with polyglactin 370 and calcium stearate serves as a lubricant, allowing the suture to pass more easily through tissue and making it more pliable for knot tying
3. Physical Configuration
- Structure: Braided multifilament
- Color: Undyed (white/off-white) or dyed violet (violet dye usually dissipates, but occasionally may be visible through skin - some surgeons avoid violet for subcuticular use)
- Sizes available: Full range from 10-0 to #2 (USP scale)
4. Tensile Strength Profile
The key feature distinguishing Vicryl from earlier absorbables:
| Time Point | Tensile Strength Retained |
|---|---|
| 2 weeks (14 days) | ~65-75% |
| 3 weeks (21 days) | ~50% |
| 4 weeks (28 days) | ~40% |
| 30 days | ~5% |
- Defined as absorbable because it loses half its tensile strength within 2 months of placement
- Stronger tensile strength retention vs. polyglycolic acid (Dexon), which retains only 20% at 3 weeks
- Weaker than PDS (polydioxanone), which retains ~70% at 2 weeks and ~50% at 4 weeks
5. Absorption / Degradation
- Mechanism: Hydrolysis (not enzymatic degradation like catgut)
- Water penetrates the suture and breaks down the ester bonds in the polymer chain
- This makes absorption more predictable and less variable between patients vs. catgut
- Timeline:
- Hydrolysis is minimal until 5-6 weeks
- Complete absorption: 60-90 days (some sources say up to 90 days)
- Bailey & Love: complete at 60-90 days
- Dermatology 2-Volume Set: generally complete by 90 days
- Contrast: Polyglycolic acid (Dexon) may still be absorbing at 120 days
6. Tissue Reactivity
- Mild tissue reaction (much less than catgut/chromic gut)
- As an absorbable suture, Vicryl produces slightly more inflammatory response than non-absorbable sutures generally, but far less than natural sutures
- Because it is braided (multifilament), it has higher capillarity than monofilament sutures - fluid and bacteria can be trapped between strands, giving it slightly higher infection risk vs. monofilaments like Monocryl or PDS
- Good knot security due to low memory (braided structure)
7. Handling Characteristics
- Easy handling - one of Vicryl's most praised features
- Holds knots well due to braided structure (low memory)
- Does not tear tissue
- Coated surface allows smooth passage through tissue
- More pliable than monofilament sutures like PDS - easier to tie
- Passes through tissue easily despite braided design
8. Clinical Uses
General Surgery
- Bowel anastomoses (gastrointestinal surgery) - ureterovesical, ureteroileal, and other anastomoses
- Fascial and muscle closure
- Subcutaneous fat approximation
- Vascular ligatures (vessel ligation)
- Has become the "workhorse" suture for many general surgical applications
- Subcuticular wound closures (undyed form preferred)
Dermatology / Plastic Surgery
- Most popular buried absorbable dermal suture in cutaneous surgery
- Deep dermal layer closure (subcutaneous buried interrupted suture)
- Running cutaneous suture when used on the surface (removed in 5-14 days)
- Excellent for vermilion lip - does not irritate mucosa, causes less inflammation than silk
- Subcutaneous fat closure: 2-0 Vicryl
- Skin subcuticular closure: 4-0 Vicryl
Ophthalmology
- Ophthalmic surgery (fine sizes, e.g. 6-0)
- Eyelid procedures, periorbital closures
Urology
- Bladder, ureter, and renal pelvis closures
- Anastomoses in intra-abdominal urologic surgery
Obstetrics & Gynecology
- Anterior colporrhaphy
- Uterine closure, fascial repair
ENT / Head & Neck Surgery
- Mucosal closures
- Subcuticular skin closures (rhinoplasty - 6/0 polyglactin)
9. Vicryl Variants
Vicryl Rapide®
- Partially hydrolyzed form of polyglactin 910 (pre-treated to speed absorption)
- Tensile strength:
- ~50% at 5 days
- 0% at 14 days
- Absorption: Complete in ~6 weeks (42 days)
- Key advantage: Does not need to be removed - spontaneously dislodges in 7-14 days
- Indications:
- Wound edge approximation where only 1-2 weeks of support needed
- Mucosa (oral, tongue, genital)
- Pediatric skin closure (avoids painful removal)
- Percutaneous use where suture removal is inconvenient or painful
- Dermabrasion, skin grafts
- Lingual/tongue lacerations
- Subcuticular closures in ENT (rhinoplasty, parathyroid, parotid surgery)
10. Tensile Strength Comparison with Other Absorbables
| Suture | Type | 2 weeks | 3 weeks | 4 weeks | Full Absorption |
|---|---|---|---|---|---|
| Vicryl | Braided | 65-75% | 50% | 40% | 60-90 days |
| Vicryl Rapide | Braided | ~0% | 0% | 0% | ~6 weeks |
| Dexon (PGA) | Braided | 63% | 20% | - | 90-120 days |
| Monocryl | Monofilament | 30-40% | - | - | 90-120 days |
| PDS II | Monofilament | 74% | - | 50% | ~180 days |
| Maxon | Monofilament | 81% | - | 59% | ~180 days |
| Chromic gut | Monofilament | ~0-30% | 0% | 0% | 70-90 days |
11. Contraindications / When NOT to Use Vicryl
- Tissues requiring prolonged support (e.g., high-tension fascial repairs, hernia mesh - PDS or Maxon preferred)
- Cardiovascular prostheses or vascular graft anastomoses (non-absorbable preferred)
- Infected wounds - braided structure increases bacterial colonization risk vs. monofilament
- When prolonged approximation under stress is needed
- Fascia closure in laparotomy - fast absorbables carry risk of dehiscence, evisceration, and incisional hernia (PDS preferred for abdominal fascial mass closure)
12. Advantages Over Predecessors
| Feature | Catgut | Vicryl |
|---|---|---|
| Tissue reactivity | High | Mild |
| Absorption predictability | Unpredictable (enzymatic) | Predictable (hydrolysis) |
| Tensile strength profile | Lost 7-10 days (plain) | 50% at 3 weeks |
| Patient variability | High | Low |
| Infection risk (vs. catgut) | Moderate-high | Low |
13. Suture Gauge / Size Selection (USP Scale)
| USP Size | Metric Size | Diameter Range | Common Use |
|---|---|---|---|
| 6-0 | 0.7 | 0.07 mm | Ophthalmology, face, fine work |
| 5-0 | 1 | 0.10-0.149 mm | Face, periorbital |
| 4-0 | 1.5 | 0.15-0.199 mm | Subcuticular skin, scalp |
| 3-0 | 2 | 0.20-0.249 mm | Deep dermis, subcutaneous fat |
| 2-0 | 3 | 0.30-0.349 mm | Deep subcutaneous fat, muscle |
| 0 | 3.5 | 0.35-0.399 mm | Fascia, thick tissue |
| 1-2 | 4-5 | 0.40+ mm | Heavy tissue, bowel, abdominal wall |
14. Key Points Summary
- Synthetic braided absorbable suture (copolymer glycolide 90% + L-lactide 10%)
- Absorbed by hydrolysis - predictable, patient-independent
- Maintains 75% tensile strength at 2 weeks, 50% at 3 weeks
- Full absorption in 60-90 days
- Mild tissue reactivity - significantly less than catgut
- Excellent knot security (braided = low memory)
- Coated with polyglactin 370 + calcium stearate for smooth tissue passage
- The most popular buried absorbable suture in cutaneous surgery
- Available as Vicryl Rapide (faster absorption, no removal needed, self-dissolves in 7-14 days)
- Available dyed violet (usually dissipates) or undyed
- Workhorse suture for general, urologic, gynecologic, and dermatologic surgery
Sources:
- Dermatology 2-Volume Set, 5e - Ch. on Suture Materials
- Bailey & Love's Short Practice of Surgery, 28th Ed. - Table 7.2
- Campbell-Walsh-Wein Urology, 3-Volume Set - Suture Materials
- Fitzpatrick's Dermatology, Vol. 1 & 2 - Suture Materials
- The Harriet Lane Handbook, 23rd Ed. - Absorbable Sutures Table
- Roberts & Hedges' Clinical Procedures in Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.