Laryngocele in detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
Finding Sources
Searching PubMed
laryngocele diagnosis treatment
Searching the Web
RGUHS ENT laryngocele 50 marks Scott Brown Cummings recent advances 2024
Reading File
Reading File
Finding Sources
Reading Article
PMID: 33646512
Reading File
Reading File
Reading Article
PMID: 38877649
Loading Image
Loading Image
Reading File
Loading Image
Reading Article
PMID: 37602305
Reading Web Page
https://www.ijorl.com/index.php/ijorl/article/view/3552
LARYNGOCELE
A Comprehensive 50-Marks Answer (RGUHS Standard)
1. DEFINITION
A laryngocele is an abnormal dilatation of the saccule (appendix) of the laryngeal ventricle (sacculus laryngis / Morgagni's ventricle) filled with air, communicating with the interior of the larynx through its orifice at the anterior end of the ventricle.
The term was first introduced by Virchow in 1867.
Stell and Maran define it as "an air-containing sac communicating with the interior of the larynx" - Cummings Otolaryngology, p. 1127
2. SURGICAL ANATOMY OF THE LARYNGEAL SACCULE
The saccule (laryngeal appendix) is a blind, finger-like pouch that arises from the anterior end of the laryngeal ventricle (space between true and false vocal folds). It:
- Extends upward between the false vocal fold medially and the thyroid cartilage laterally
- Lies posterolateral to the epiglottis at the level of its petiole
- Contains numerous mucous glands (50-70 in number) that lubricate the true vocal folds
- Empties through an orifice in the anterior part of the ventricle
- Normal length: 6-8 mm in 75%; 10 mm or more in 25% (Broyles - study of 100 cadaver larynges)
ANATOMY DIAGRAM - LARYNGEAL VENTRICLE AND SACCULE
Epiglottis
|
False Vocal Fold (Ventricular Band)
|
[VENTRICLE of Morgagni]
/ \
[SACCULE] ←-→ [True Vocal Fold]
(Appendix of
the Ventricle)
|
Orifice (anterior)
|
Mucous glands
(lubrication of TVF)
3. CLASSIFICATION
A. By Contents (Cummings / Stell and Maran)
| Type | Contents | Orifice | Former Name |
|---|---|---|---|
| Laryngocele | Air | Patent | True laryngocele |
| Saccular Cyst (Mucocele) | Mucus | Blocked | Mucous retention cyst |
| Laryngopyocele | Pus | Blocked | Infected laryngocele |
B. By Location (DeSanto Classification - most used in RGUHS)
| Type | Description | Frequency |
|---|---|---|
| Internal (Intralaryngeal) | Confined within the thyroid cartilage framework; lies in the paraglottic space; sac expands medially, bulging the false fold and AE fold | 44% |
| External (Extralaryngeal) | Sac herniates through the thyrohyoid membrane, appears as neck swelling | 27% |
| Combined (Mixed) | Both internal and external components, passing through thyrohyoid membrane like an "hourglass" shape | 29% |
Almost 25% of laryngoceles are bilateral - Cummings, p. 2514
DIAGRAM 1: Classification by Location (from Cummings Textbook)
Fig. 60.29 - Classification scheme for laryngocele and saccular cyst:
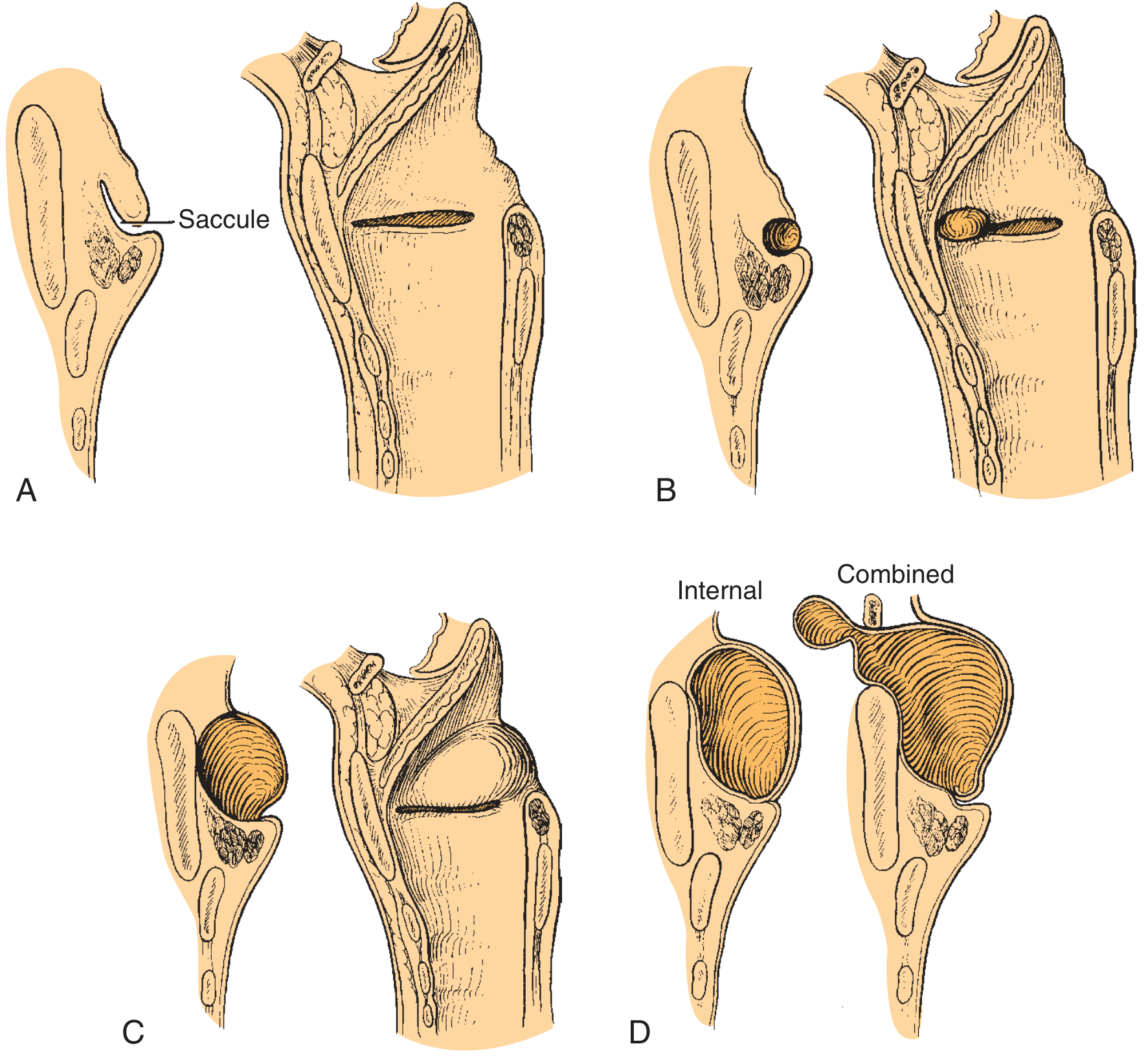
(A) Normal anatomy with saccule labeled. (B) Anterior saccular cyst - protrudes into vestibule. (C) Lateral saccular cyst - dissects into false fold and AE fold. (D) Internal vs. Combined laryngocele types.
4. INCIDENCE AND EPIDEMIOLOGY
- Rare condition - incidence approximately 1 in 2.5 million people per year
- More common in males (M:F = 5:1 to 8:1)
- Peak incidence: 5th-6th decade (around age 50)
- Bilateral in 25% of cases
- Associated with laryngeal carcinoma in 5-29% of cases (critical fact for RGUHS)
5. ETIOLOGY AND PREDISPOSING FACTORS
PRIMARY CAUSES
-
Increased intraluminal (transglottic) pressure - the most commonly cited cause:
- Trumpet players, trombonists
- Glass blowers
- Wind instrument players
- Forceful shouting/singers
-
Congenital - in infants; saccular disorders appearing congenitally
-
Idiopathic - Stell and Maran stated the relationship to occupational pressure "may have been overstated" since few patients in world literature had such hobbies. Many cases have no identifiable cause.
-
Obstructive (Secondary):
- Laryngeal carcinoma obstructing the saccular orifice - most clearly documented organic cause
- This is the most important predisposing factor to rule out
- Post-laser surgery remnants buried in tissue
-
Post-tracheostomy - rare complication of surgical tracheostomy
FLOWCHART 1: PATHOPHYSIOLOGY OF LARYNGOCELE
INCREASED INTRALUMINAL PRESSURE
(occupational / idiopathic / tumour)
|
↓
Repeated positive pressure on saccular orifice
|
↓
Saccule dilates with air
|
┌─────┴──────┐
↓ ↓
Patent Orifice Blocked Orifice
| |
↓ ↓
LARYNGOCELE Mucus accumulates
(air-filled) |
SACCULAR CYST
(mucus-filled)
|
If infected → pus
|
LARYNGOPYOCELE
6. PATHOLOGY
- Wall lined by pseudostratified ciliated columnar epithelium (respiratory epithelium) - most common finding on HPE
- May show squamous metaplasia
- Contains mucous glands in the wall
- 3 of 50 reviewed cases showed Squamous Cell Carcinoma in the wall (Indian review, IJORL 2022)
7. CLINICAL FEATURES
Symptoms
The presentation depends on type (Internal / External / Combined):
A. Internal Laryngocele:
- Hoarseness (most common) - due to downward pressure on true vocal fold or premature closure of the vestibule at the false fold level during phonation
- Stridor (second most common)
- Dysphagia
- Sore throat
- Chronic cough
- Snoring
- Rarely - sudden acute dyspnoea (airway emergency)
B. External Laryngocele:
- Neck swelling - most common presentation (palpable in lateral neck at the level of the thyrohyoid membrane)
- Swelling increases on Valsalva maneuver or puffing
- Swelling reduces on compression (Bryce sign - gurgling heard on compression of the neck mass)
- May present as airway emergency if large
C. Combined Laryngocele:
- Features of both - hoarseness + neck swelling
- Most common type presenting clinically
D. Laryngopyocele:
- Acute onset fever
- Rapidly enlarging tender neck mass / sore throat
- Severe dyspnoea
- Airway emergency
Signs
| Sign | Description |
|---|---|
| Bryce's Sign | Gurgling sound heard when a neck mass (laryngocele) is compressed |
| Valsalva distension | Swelling increases with straining/puffing |
| Compressible swelling | Translucent, reducible neck mass |
| Submucosal bulge | Bulging of the false fold/AE fold on laryngoscopy |
8. INVESTIGATIONS
A. Laryngoscopy (Indirect / Fibreoptic / Direct)
- Shows submucosal bulge in the false vocal fold, AE fold, or supraglottis
- Mucosa over the swelling is intact and smooth
- Ventricle may show an opening
- Mandatory to rule out underlying carcinoma (5-29% association)
- Direct laryngoscopy: even a large cyst may disappear under general anesthesia (cyst compresses/collapses)
B. CT Scan Neck (GOLD STANDARD)
- Best investigation - defines type, size, extent, and contents
- Internal laryngocele: air-filled space in paraglottic space within thyroid framework
- External laryngocele: air-filled space herniating through thyrohyoid membrane
- Combined: both components; "hourglass" at thyrohyoid membrane
- Enhancing wall = infection (laryngopyocele)
- Soft tissue density = mucus-filled saccular cyst
- Valsalva maneuver during CT improves visualization
CT SCAN IMAGE - Internal Laryngocele (Cummings, Fig. 104.15)
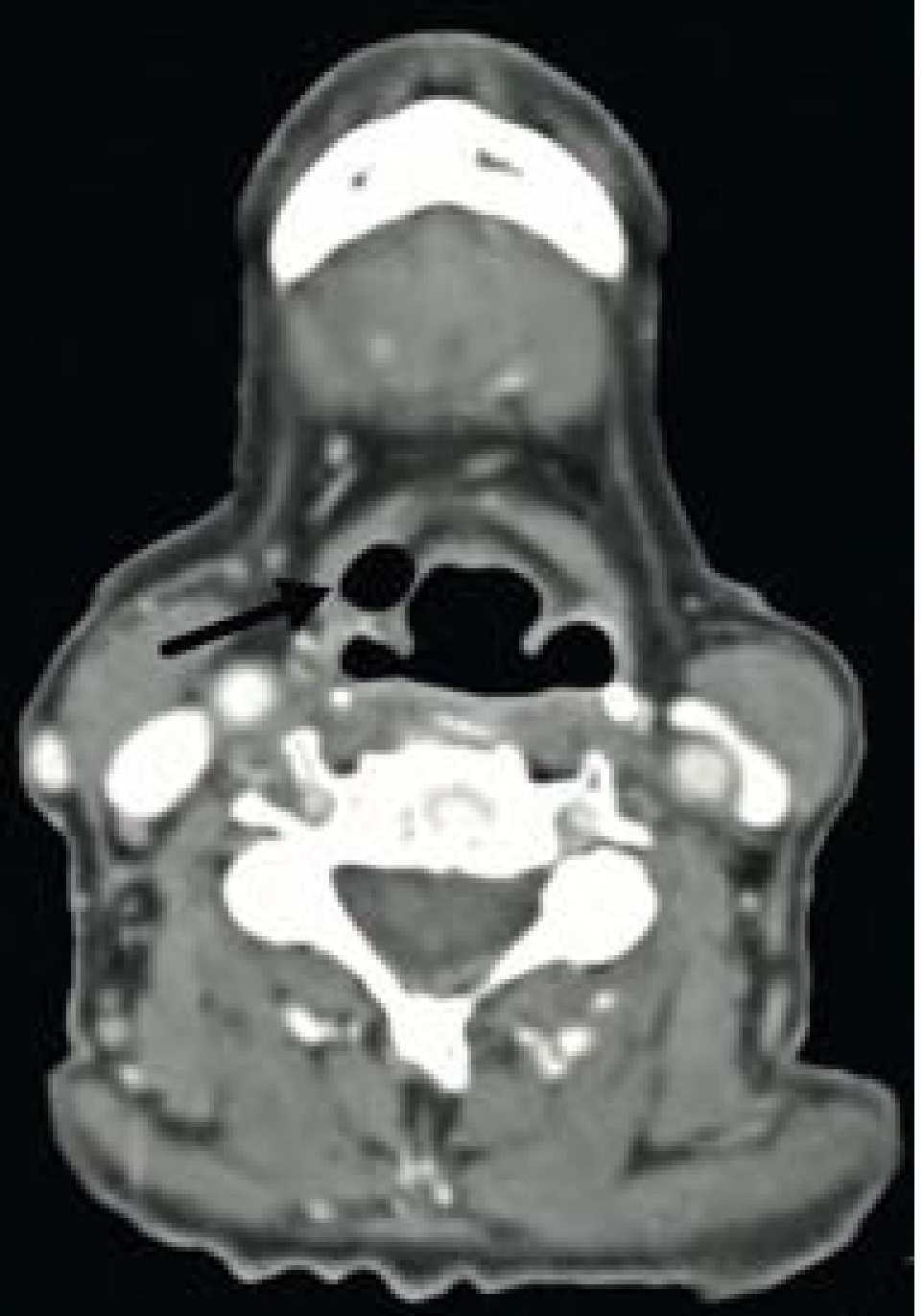
CT scan showing the air-filled laryngocele (arrow) located in the right paraglottic space, exerting mass effect on the right piriform sinus.
CT SCAN IMAGE - Pre and Post-operative CT (Cummings, Fig. 60.33)
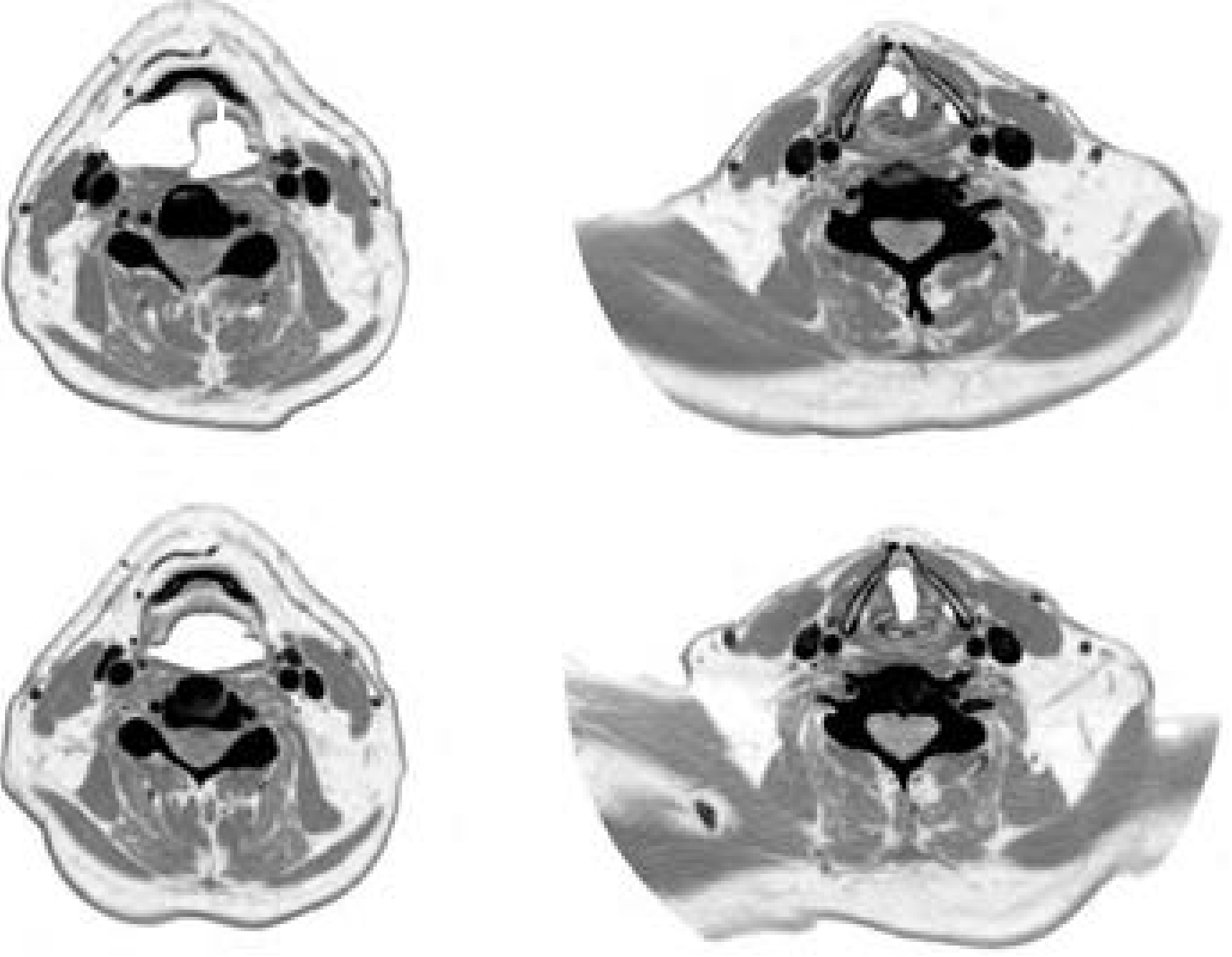
Pre-operative: large air-filled sac pushing epiglottis to one side. Post-operative: resolution after excision.
C. MRI Neck
- Useful when CT equivocal
- Air-filled lesions: signal void
- Fluid-filled lesions: high signal on T2
- Better soft tissue detail
D. Plain X-ray Neck (Lateral)
- A-P and lateral views may show air shadow in the neck
- Of historical interest; superseded by CT
E. Ultrasound
- Compressible cystic structure
- Can help differentiate from solid masses
- Limited utility compared to CT
FLOWCHART 2: DIAGNOSTIC APPROACH TO LARYNGOCELE
Patient with neck swelling / hoarseness
|
↓
Clinical Examination
(Bryce sign, Valsalva response)
|
↓
Indirect / Fibreoptic Laryngoscopy
(submucosal bulge, rule out carcinoma)
|
┌───────────┴───────────┐
↓ ↓
Supraglottic bulge Normal
(false fold/AE fold/ (consider other Dx)
ventricular swelling)
|
↓
CT SCAN NECK (with Valsalva)
|
┌─────────┼──────────┐
↓ ↓ ↓
Air-filled Fluid-filled Enhancing
(Laryngocele) (Saccular wall
Cyst) (Laryngopyocele)
|
↓
Define Type: Internal / External / Combined
|
↓
Direct Laryngoscopy + Biopsy
(MANDATORY to exclude carcinoma)
|
↓
MANAGEMENT
9. DIFFERENTIAL DIAGNOSIS
| Condition | Distinguishing Feature |
|---|---|
| Branchial cyst | Anterior to SCM at angle of jaw; no Bryce sign; CT - lateral neck mass; no change with Valsalva |
| Thyroglossal duct cyst | Midline; moves with tongue protrusion |
| Cystic hygroma | Multilocular; transilluminant; CT - lymphatic spaces |
| Lateral pharyngeal pouch | Mucosal-lined diverticulum of pharynx; barium swallow confirms |
| Ranula | Floor of mouth; plunging type may go into neck |
| Cold abscess | History of TB; systemic features |
| Lipoma | Soft, mobile, non-compressible |
| Laryngeal carcinoma | Fixed, irregular, associated with hoarseness |
| Parapharyngeal space tumor | Displaces tonsil medially; CT/MRI defines |
10. MANAGEMENT
A. Conservative (Observation)
- Asymptomatic small internal laryngoceles may be followed if causing no symptoms
- Not used for external or combined laryngoceles
FLOWCHART 3: MANAGEMENT ALGORITHM FOR LARYNGOCELE
CONFIRMED LARYNGOCELE (CT defined)
|
┌─────────────┼─────────────┐
↓ ↓ ↓
INTERNAL EXTERNAL COMBINED
Small Larger Large
| | |
↓ ↓ ↓
┌────────────┐ ┌──────────────┐ ┌────────────────┐
│Endoscopic │ │ EXTERNAL │ │ Endoscopic OR │
│Excision or │ │ TRANSCERVICAL│ │ External │
│Marsupialization│ APPROACH │ │ approach │
└────────────┘ └──────────────┘ └────────────────┘
|
Recurrence
|
External
approach
LARYNGOPYOCELE → URGENT IV Antibiotics
→ Airway management (tracheostomy if needed)
→ Drain when settled
→ Definitive excision
B. Surgical Management
ENDOSCOPIC APPROACH (Minimally Invasive)
Indications:
- Small internal laryngoceles
- All types in expert hands (Hogikyan and Bastian, 1996 - 7 large cysts removed endoscopically)
- Preferred for combined laryngoceles in recent practice
Technique - Endoscopic Marsupialization:
- Direct laryngoscopy under GA
- Identify the bulge of the false fold
- CO2 laser or microdebrider/cold steel incision of the mucosa over the lesion
- Marsupialize the sac - create a large opening
- Send tissue for biopsy
Technique - Endoscopic Excision (Complete):
- Direct laryngoscopy under GA
- Excise the false fold
- Follow the cyst wall - even if it extends over thyroid cartilage into the neck
- Deliver entire cyst intact or piecemeal
- The cyst may be collapsed/decompressed first if large, then wall excised progressively
Instruments used:
- CO2 laser (Martinez Devesa et al., 2002 - CO2 laser management)
- Microdebrider
- Cold steel (cupped forceps, scissors)
- Coblation/plasma (Zhang et al., 2023 - new technique)
Advantages of endoscopic approach:
- No external scar
- Shorter hospital stay
- Outpatient in 4/7 patients (Bastian series)
- No tracheotomy needed in most
- Complete excision possible for combined laryngoceles
Disadvantage:
- Marsupialization alone has 4.8x higher recurrence than complete excision (Purnell et al., Systematic Review 2022, PMID 33646512)
EXTERNAL TRANSCERVICAL APPROACH
Indications:
- External or combined laryngoceles
- Recurrent laryngoceles after endoscopic failure
- Large lesions inaccessible endoscopically
- When malignancy suspected
Thyrotomy / Transcervical Technique (DeSanto approach):
- Horizontal cervical incision at level of thyrohyoid membrane
- Elevation of subplatysmal flaps
- Identify the saccular herniation through thyrohyoid membrane
- Follow the external sac through the membrane
- Transect as close as possible to the saccular orifice in the ventricle
- Some surgeons remove a portion of the upper thyroid cartilage for better access (though not always necessary)
- Layered closure
Thyroid Chondroplastic Flap (El-Naggar et al., 2021 - Eur Arch Otorhinolaryngol):
- Modified external approach using a thyroid cartilage flap for better exposure
- Allows better access to deep internal component
- Good for combined laryngoceles
ROBOTIC-ASSISTED SURGERY (RECENT ADVANCE)
- Transoral Robotic Surgery (TORS)
- Used for combined and large laryngoceles
- Systematic review (Purnell et al., 2022): Robotic vs endoscopic - no significant difference in tracheostomy rates, complications, or recurrence
- Robotic approach had longer hospital stay and more NGT use
- Not routinely used; reserved for complex cases
C. Management of Laryngopyocele (Infected Laryngocele)
- Urgent airway management - intubation or emergency tracheostomy if needed
- IV antibiotics (amoxicillin-clavulanate / cefuroxime / metronidazole)
- CT scan to confirm diagnosis and rule out deep space abscess
- Incision and drainage - after antibiotic stabilization
- Definitive excision - 4-6 weeks after infection settles (transcervical approach preferred)
11. COMPLICATIONS
Complications of the Disease
- Acute airway obstruction - life-threatening; if large combined laryngocele or infected
- Dysphagia - from large mass effect
- Aspiration pneumonia - from chronic aspiration
- Association with laryngeal carcinoma (5-29%)
Complications of Surgery
- Recurrence - more common with marsupialization (22.22%) vs. complete excision (4.76%)
- Infection / laryngopyocele
- Damage to recurrent laryngeal nerve (external approach)
- Haematoma / seroma (external approach)
- Airway compromise - requiring tracheostomy (approx. 18.95% complication rate - Purnell 2022)
- Subcutaneous emphysema
- Wound infection
12. PROGNOSIS
- Excellent with complete surgical excision
- No recurrence in most series with total excision
- Recurrence higher with marsupialization only
- Must follow-up with repeat laryngoscopy to rule out underlying carcinoma
13. WHAT STELL AND MARAN SAY (Key Points for RGUHS)
As quoted in Cummings:
"Stell and Maran believe that the relationship of laryngocele to occupational activities requiring high transglottic pressures may have been overstated, because few reported patients with such disorders in world literature had such hobbies."
They emphasize:
- The idiopathic nature of most laryngoceles
- The importance of ruling out carcinoma BEFORE surgery
- Classification by DeSanto (internal/external/combined)
- External approach preferred historically for combined lesions
14. SCOTT BROWN'S CONTRIBUTIONS
Scott Brown's Otorhinolaryngology emphasizes:
- Laryngopyocele as a surgical emergency
- The importance of CT with Valsalva maneuver
- Endoscopic CO2 laser as first-line for internal laryngoceles
- Association with carcinoma - perform biopsy before excision
- Histopathology - respiratory epithelium lining
15. DHINGRA (Diseases of ENT - Indian Standard)
- Defines laryngocele as air-containing dilatation of the saccule
- Classification: Internal, External, Mixed
- Investigations: CT neck (investigation of choice)
- Treatment: Surgical excision (external approach for mixed, endoscopic for internal)
- Points out: "bryce sign" and valsalva distension as clinical features
- Biopsy mandatory to rule out malignancy
16. HAZARIKA (Textbook of ENT)
- Emphasizes classification, pathological anatomy
- Notes the hourglass shape of combined laryngocele at thyrohyoid membrane
- Diagnostic points: Bryce sign, indirect laryngoscopy, CT
- Management: CO2 laser endoscopic excision for internal, external approach for combined
- Histopathology: squamous / respiratory epithelium lining
17. ZAKIR HUSSAIN (Key Points for RGUHS)
- Definition and classification similar to standard texts
- Clinical features: dyspnoea, hoarseness, neck swelling with valsalva increase
- Diagnostic: CT scan gold standard
- Surgery: choice of approach depends on type
- Important differentials - emphasizes lateral pharyngeal diverticulum vs laryngocele
18. RECENT ADVANCES (2020-2024)
A. Minimally Invasive Approaches
-
Transoral Robotic Surgery (TORS)
- Purnell et al. (J Robotic Surg, 2022) - Systematic review of 30 studies, 95 patients
- No significant difference from endoscopic approaches in outcomes
- Endoscopic complete excision preferred over marsupialization (4.8x lower recurrence)
- [Systematic Review, PMID 33646512]
-
Coblation/Plasma Technology
- Zhang et al. (Exp Ther Med, 2023) - internal laryngocele treated with plasma ablation
- No tracheostomy required; satisfactory outcomes
- Represents emerging minimally invasive endoscopic technique
- [PMID 37602305]
-
Thyroid Chondroplastic Flap
- El-Naggar et al. (Eur Arch Otorhinolaryngol, 2021) - new external approach
- Better exposure of saccular base
- Lower recurrence
- [PMID 33638087]
B. Bilateral Combined Laryngocele - Emerging Recognition
- Alkheder et al. (ENT Journal, 2024) - bilateral combined laryngocele: 77 documented cases in world literature
- Predominantly males (~57 years)
- CT confirmation of bilateral involvement critical
- Tracheostomy often needed before definitive surgery
- [PMID 38877649]
C. Laryngocele as Airway Emergency
- Trivedi et al. (BMJ Case Reports, 2022) - undiagnosed laryngocele causing airway emergency
- Laryngopyocele presenting as acute upper airway obstruction
- Importance of early diagnosis; risk of fatal airway compromise
- [PMID 35272990]
D. Association with Laryngeal Carcinoma - Updated Data
- 5-29% of laryngoceles associated with ventricular carcinoma
- PET-CT emerging as tool when malignancy suspected with laryngocele
- Mandatory biopsy before excision remains standard of care
E. Imaging Advances
- Valsalva CT protocol - Madhavan et al. (AJNR, 2019) - improves visualization; Valsalva maneuver during CT distends the sac maximally
- MRI with dynamic sequences gaining role
- Ultrasound-guided aspiration - palliative in frail patients not fit for surgery
19. SUMMARY TABLE (High-Yield for RGUHS)
| Parameter | Internal | External | Combined |
|---|---|---|---|
| Location | Paraglottic space | Neck (through thyrohyoid membrane) | Both |
| Presentation | Hoarseness | Neck swelling | Both |
| Bryce sign | Absent | Present | Present |
| Valsalva | No visible change | Neck mass increases | Increases |
| CT finding | Air in paraglottic space | Air in lateral neck | Hourglass |
| Surgery | Endoscopic excision | External transcervical | Endoscopic or external |
| Recurrence risk | Low | Low | Moderate |
FLOWCHART 4: COMPLETE CLINICAL APPROACH SUMMARY
LARYNGOCELE
|
├── DEFINITION: Air-filled dilatation of saccule of Morgagni's ventricle
|
├── ANATOMY: Saccule → anterior ventricle → between false fold and thyroid cart.
|
├── CLASSIFICATION
| ├── By contents: Laryngocele / Saccular Cyst / Laryngopyocele
| └── By location: Internal (44%) / External (27%) / Combined (29%)
|
├── AETIOLOGY: Increased pressure / Idiopathic / Carcinoma obstruction
|
├── CLINICAL FEATURES
| ├── Internal: Hoarseness, stridor, dysphagia
| ├── External: Neck swelling + Bryce sign + Valsalva
| └── Laryngopyocele: Fever + Airway emergency
|
├── INVESTIGATIONS
| ├── Laryngoscopy: submucosal bulge, rule out Ca
| ├── CT Neck (GOLD STANDARD): type, contents, extent
| └── Direct laryngoscopy + Biopsy (mandatory)
|
├── TREATMENT
| ├── Internal → Endoscopic complete excision (CO2 laser / Coblation)
| ├── External → External transcervical approach
| ├── Combined → Endoscopic ± External
| └── Pyocele → IV antibiotics → I&D → Definitive excision
|
├── COMPLICATIONS: Airway obstruction / Carcinoma association / Recurrence
|
└── RECENT ADVANCES
├── TORS (Robotic surgery)
├── Plasma/Coblation ablation
├── Thyroid chondroplastic flap
└── Valsalva CT protocol
REFERENCES
- Cummings Otolaryngology - Head and Neck Surgery (7th ed.) - Chapter 60: Saccular Disorders, Laryngocele and Saccular Cysts, p. 1127-1130; Chapter 104: Imaging of Laryngocele, p. 2514
- Scott Brown's Otorhinolaryngology and Head and Neck Surgery (8th ed.) - Benign laryngeal lesions
- Stell and Maran's Head and Neck Surgery - Laryngocele; quoted in Cummings for occupational pressure controversy
- K.J. Lee's Essential Otolaryngology (11th ed.) - p. 924-925
- Dhingra - Diseases of Ear, Nose and Throat - Laryngocele chapter
- Hazarika - Textbook of Ear, Nose and Throat - Laryngocele
- Purnell PR, Haught E, Turner MT - "Minimally invasive treatment of laryngoceles: a systematic review and pooled analysis." J Robot Surg, 2022. [PMID 33646512] - demonstrates endoscopic complete excision superior to marsupialization; no significant difference between robotic and endoscopic approaches
- Alkheder A et al. - "Bilateral Combined Laryngocele: Comprehensive Review of the Literature." Ear Nose Throat J, 2024. [PMID 38877649] - Virchow's 1867 description; 77 cases in world literature; bilateral laryngocele management
- Zhang J et al. - "Laryngocele: Report of two rare cases and review of the literature." Exp Ther Med, 2023. [PMID 37602305] - Plasma/coblation as new minimally invasive technique
- Trivedi S et al. - "Undiagnosed laryngocele: an airway emergency." BMJ Case Rep, 2022. [PMID 35272990] - Laryngopyocele as life-threatening emergency
- El-Naggar A et al. - "Thyroid chondroplastic flap for resection of laryngoceles." Eur Arch Otorhinolaryngol, 2021. [PMID 33638087] - Modified external approach
- K.U. et al. - "Laryngocele: a case report and review of 50 cases from literature." IJORL, 2022 - Indian series; SCC in 3/50 cases; neck swelling most common presentation
RGUHS Exam Tip: For a 50-mark question, cover Definition + Anatomy + Classification + Etiology + Clinical Features + Investigations + Differential Diagnosis + Treatment (endoscopic + external + pyocele) + Complications + Recent Advances. Draw the DeSanto classification diagram and the management flowchart for 10-15 marks of visual credit.
This is a shared conversation. Sign in to Orris to start your own chat.