ECG
Asking for Preferences
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Searching PubMed
pericarditis ECG diagnosis
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
I now have everything needed for a comprehensive, well-sourced answer. Let me compile it.
ECG Findings in Pericarditis
Why the ECG Changes Happen
The pericardium itself is electrically silent - ECG changes in pericarditis actually reflect subepicardial myocardial inflammation (epicarditis), which is why the term "perimyocarditis" is often more accurate. This also explains why ECG changes are seen in only ~60% of pure pericarditis cases, but in >90% when there is concomitant myocarditis. - Braunwald's Heart Disease, 10e
The 4 Stages of ECG Evolution
These changes evolve over days to weeks, though not every patient progresses through all four stages:
| Stage | PR Segment | ST Segment | T Wave |
|---|---|---|---|
| 1 (Acute) | Depressed (esp. II, aVF, V4-V6) | Diffuse elevation (I, V5, V6); ST:T ratio >0.25 | Upright |
| 2 | Isoelectric or depressed | Returns to baseline | Flattening/decreased amplitude |
| 3 | Isoelectric or depressed | Isoelectric | Diffuse T-wave inversion (I, V5, V6) |
| 4 (Resolution) | Isoelectric | Isoelectric | Normal |
- Tintinalli's Emergency Medicine
Key ECG Features - Stage 1 (What You'll See in Acute Presentation)
1. Diffuse ST Elevation
- Present in most leads: I, II, III, aVF, V2-V6
- Shape is concave upward ("saddle-shaped") - this is a key differentiator from STEMI
- Absent in aVR (which shows ST depression instead)
- Most pronounced in the lateral precordial leads (V5-V6)
2. PR Segment Depression
- Seen especially in leads II, aVF, V4-V6
- Caused by atrial injury current from epicardial inflammation spreading to the superficial atrial myocardium
- PR depression in lead aVR (PR elevation in aVR) is highly specific for pericarditis
- Can be the sole ECG manifestation in some cases
3. Reciprocal Changes - Absent
- Unlike STEMI, pericarditis does NOT produce reciprocal ST depression in other leads (except aVR/V1)
4. No Q Waves - pericarditis does not cause pathologic Q waves
5. If large effusion develops: Low QRS voltage + electrical alternans (beat-to-beat QRS axis alternation due to the heart swinging within the effusion)
ECG from Braunwald's Heart Disease - Acute Pericarditis
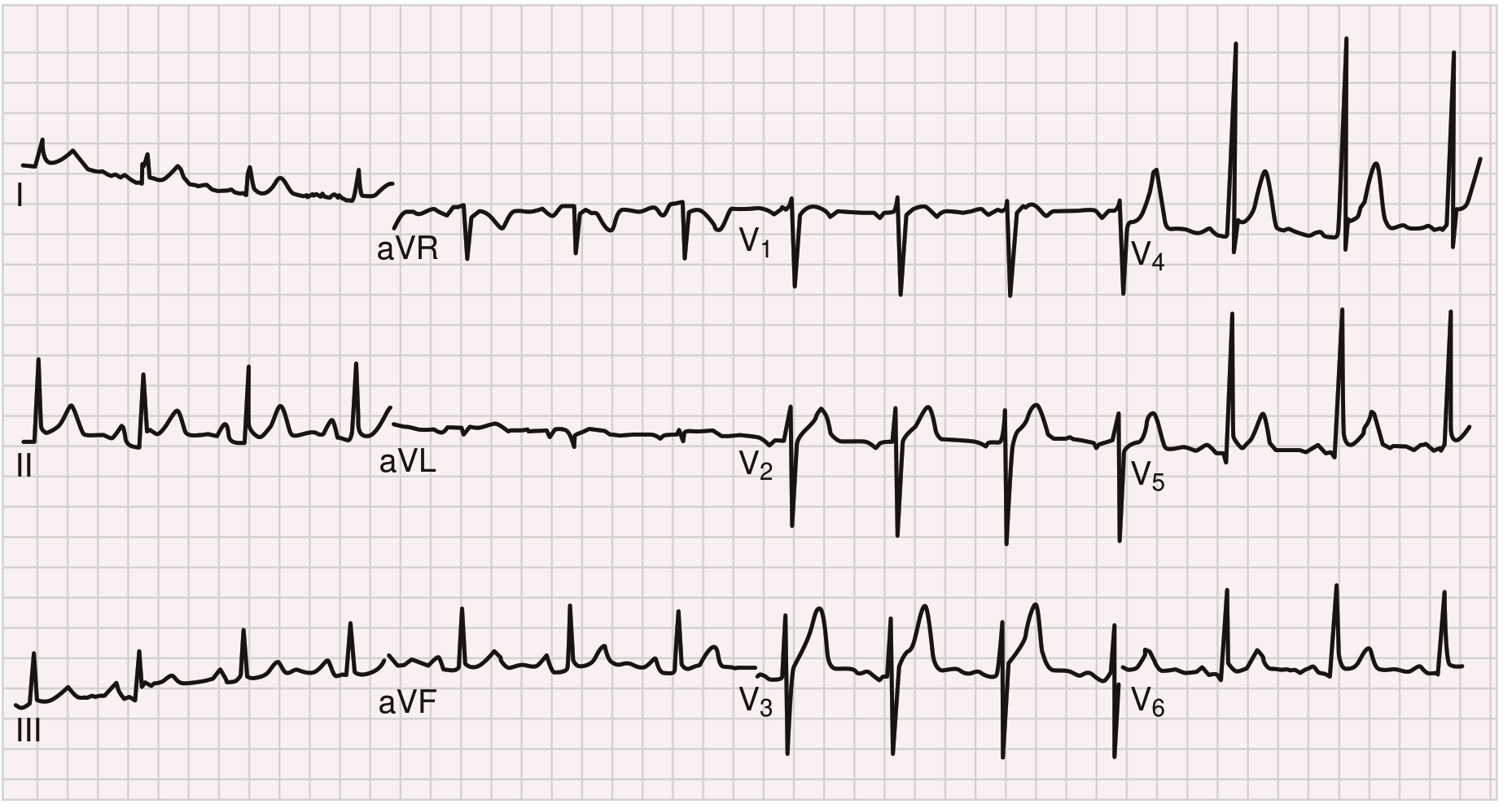
Note the diffuse ST-segment elevation and PR-segment depression across multiple leads.
The 4-Stage Evolution (Tintinalli's - Serial ECGs)
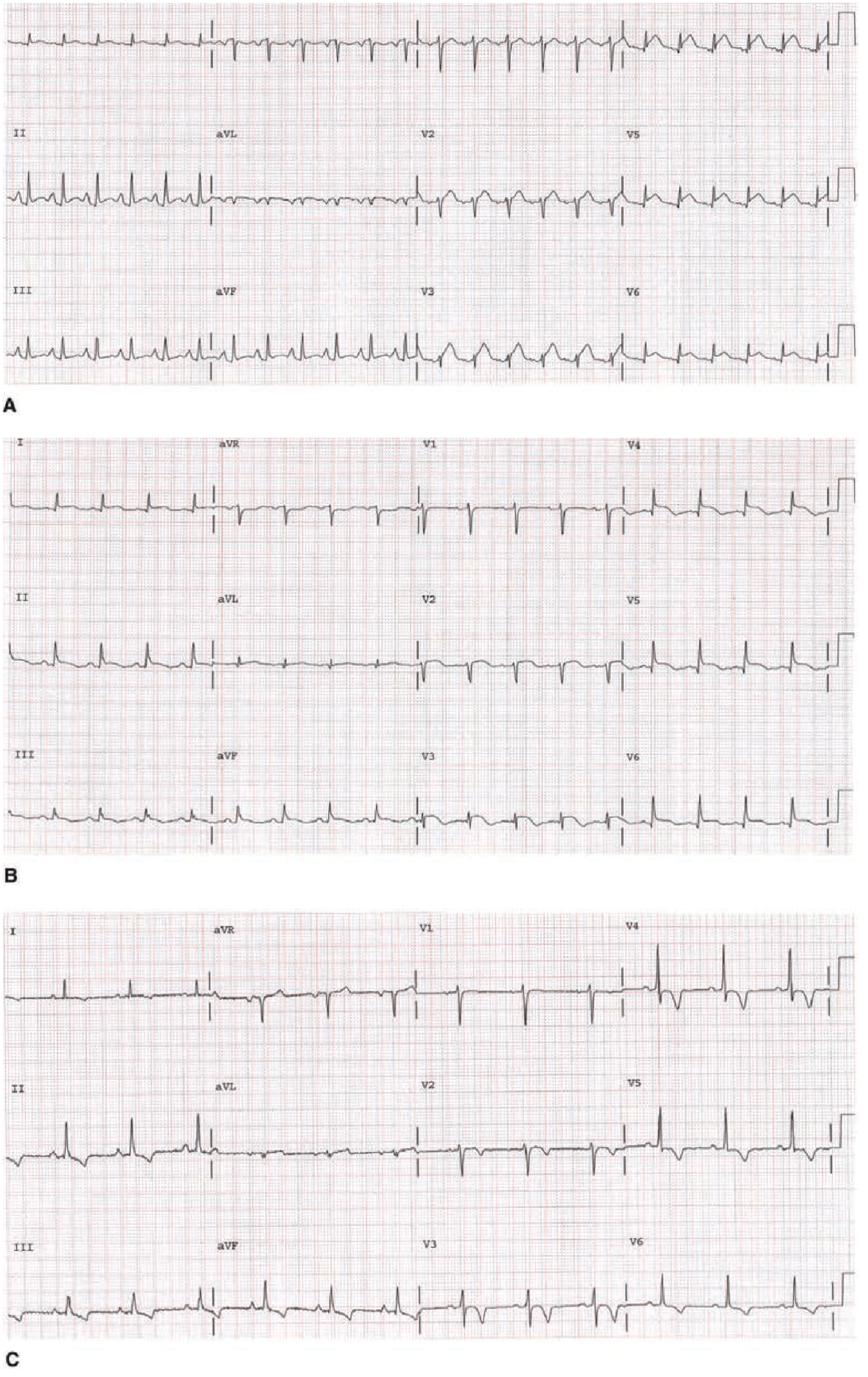
- A (Stage I): Diffuse ST elevation + PR depression in I, II, III, aVF
- B (Stage II): ST segments returning toward isoelectric
- C (Stage III): T-wave inversion throughout, ST now normal
How to Differentiate from STEMI and Early Repolarization
This is the most clinically important distinction.
| ECG Feature | Acute Pericarditis | Early Repolarization | STEMI |
|---|---|---|---|
| PR depression | Yes | No | No |
| ST shape | Concave (saddle) | Concave | Usually convex (tombstone) |
| ST distribution | Widespread (all leads) | Precordial + inferior | Localized (territory-specific) |
| Reciprocal ST depression | No | No | Common |
| T-wave inversion | After ST normalizes | No | Before ST normalizes |
| ST/T ratio in V6 | >0.25 | <0.25 | Variable |
| Q waves | No | No | Possible |
- Fuster and Hurst's The Heart, 15th Edition
The ST/T Ratio (Spodick's Ratio in V6)
Measure from the J point and T-wave peak in lead V6 (or lead I):
- ST amplitude ÷ T-wave amplitude > 0.25 → pericarditis likely (sensitivity >85%, specificity >80%, LR+ ~4)
- < 0.25 → early repolarization more likely (LR- ~0.2)
This is the key bedside tool when it is unclear whether you are looking at pericarditis or a normal variant.
T-Wave Inversion Timing
In pericarditis, T-wave inversion occurs after the ST segment normalizes (Stage 3). In STEMI, T-wave inversion appears before or concurrent with ST normalization. This temporal difference is diagnostically useful on serial ECGs. - Goldman-Cecil Medicine
Special Cases Where Classic ECG Changes Are Absent or Atypical
- Uremic pericarditis - typically NO ECG changes, because the epicardium is not involved in the inflammatory process
- Post-MI pericarditis (Dressler syndrome) - ECG changes may be atypical or masked by the underlying MI pattern
- Large pericardial effusion - may suppress voltages and produce electrical alternans instead of the classic ST changes
Diagnostic Criteria for Acute Pericarditis
Diagnosis requires 2 of 4 criteria:
- Typical chest pain (pleuritic, relieved by leaning forward)
- Pericardial friction rub
- Characteristic ECG changes
- Pericardial effusion on echo
ECG changes alone are not required. - Goldman-Cecil Medicine
Quick Summary Card
PERICARDITIS ECG - KEY POINTS
- Diffuse ST elevation (concave/saddle-shaped) in most leads
- PR depression (especially II, aVF, V4-V6)
- ST elevation in aVR absent (ST depression in aVR instead)
- NO reciprocal changes, NO Q waves
- 4-stage evolution over days-weeks
- ST/T ratio >0.25 in V6 = pericarditis vs early repolarization
- T inversion appears AFTER ST normalizes (not before - unlike STEMI)
- Low voltage + electrical alternans = suspect large effusion
Sources: Goldman-Cecil Medicine; Braunwald's Heart Disease; Tintinalli's Emergency Medicine; Fuster and Hurst's The Heart, 15th Ed; Rosen's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.