How much pics i can upload
You can upload 1 image at a time per message. There's no hard cap on the total number of images across a conversation, but each message supports a single image attachment.
If you have multiple images to share, just send them in separate messages one by one!
Is there any limit for one day .
There is no daily limit on how many images you can upload in this chat. You can send as many images as you need, one per message, throughout the day.
Just keep sending them whenever you're ready!


IMG_2222.jpg
IMG_2223.jpg
Explain in detail
analyse_media
analyse_media
Diabetes in Pregnancy - Detailed Notes
PART 1
1. Carbohydrate Metabolism in Pregnancy
Insulin Resistance (IR) in pregnancy:
Pregnancy is a diabetogenic state because of hormones that cause insulin resistance:
- HPL (Human Placental Lactogen) - main culprit
- Estrogen, Progesterone, Prolactin (PRL), Cortisol
- hCG - does NOT cause insulin resistance
As gestation progresses, HPL secretion increases, increasing IR. Significant IR develops around 24-28 weeks of gestation.
Key placental transfer facts:
| Substance | Crosses Placenta? |
|---|---|
| Maternal insulin | NO |
| Maternal glucose | YES |
| Maternal thyroxine | YES |
- Fetus is entirely dependent on mother for glucose.
- Glycosuria is normal in pregnancy.
2. Pregnancy Complications of Diabetes
Fetal complications:
- Maternal glucose crosses placenta → fetus absorbs it → fetal hyperglycemia
- Fasting hypoglycemia (advice: avoid fasting)
- Post-prandial hypoglycemia (due to IR)
- Fasting/vomiting/diarrhea → Hypoglycemia → Acetone bodies → Ketosis
High-risk pregnancy mechanism:
Hyperglycemia → feto-toxic → ↑↑ Free radicals → cross placenta → Congenital malformations of fetus
3. Classification of Diabetes in Pregnancy
| Feature | Pre-gestational Diabetes | Gestational Diabetes (GDM) |
|---|---|---|
| Who | Diabetic female conceives | Normoglycemic female conceives |
| Blood sugar ↑ | From Day 1 | From 24-28 weeks |
| Free radicals | Form from day 1 | Begin forming after 24-28 wks (after organogenesis) |
| Congenital malformations | YES | NO (radicals form after organogenesis) |
| Resolves after delivery? | NO | YES - within 6 weeks |
4. Priscilla White Classification
Priscilla White Classification
|
--------------------------------
| |
Type A Non-Type A
Gestational Diabetes Pregestational Diabetes
|
-----------
A1 A2
GDM on diet GDM on Rx
(Insulin / Metformin)
Development of GDM:
- Usually at 24-28 weeks
- Can be seen earlier (<20 wks) → usually pre-GDM
- Confirmed: Repeat sugar level at 6 weeks postpartum
5. Investigations for GDM
- TIFFA (Targeted Imaging for Fetal Anomalies): Done in all GDM + Pre-GDM at 18-20 weeks
Management trigger:
- 2hr PP blood sugar ≥ 200 mg/dL → Always give Insulin (irrespective of GDM or Pre-GDM)
PART 2: Pregestational Diabetes
6. Criteria for Pregestational Diabetes
| Test | Cut-off |
|---|---|
| FBS | ≥ 126 mg/dL |
| 2hr PPBS | ≥ 200 mg/dL |
| RBS | ≥ 200 mg/dL |
| HbA1c | ≥ 6.5% |
- DIPSI Test: Recommended by Govt. of India at 1st ANC visit
7. HbA1c - Risk Assessment for Congenital Anomalies
| HbA1c | Risk of Gross Congenital Anomalies (GCA) |
|---|---|
| < 6.5% | No risk |
| > 6.5% | 3% risk |
| ≥ 10% | 15-20% risk |
- Goal of therapy: HbA1c < 6%
8. Investigations
- Initial: USG
- Screening: Level I USG
- Diagnostic: TIFFA
- Karyotyping: NOT done (detects chromosomal anomalies, not GCA)
9. Congenital Fetal Malformations
| Category | Most Common |
|---|---|
| System involved | CVS > CNS |
| Congenital malformation | VSD (Ventricular Septal Defect) > NTD (Neural Tube Defect) |
| Cardiac malformation | VSD |
| Most SPECIFIC cardiac anomaly | TGA (Transposition of Great Arteries) |
| Cardiac finding | HOCM (Hypertrophic Obstructive Cardiomyopathy) |
Caudal Regression Syndrome - classic malformation seen in diabetic mothers (shown in image).
Prevention of GCA:
- Strict glucose control (HbA1c < 6.5% = nil risk)
- Switch to insulin before conception / on confirmation of pregnancy
- Folic acid 400 mcg/day
- Begin 1 month before conception
- Continue for 3 months post conception
PART 3: Other Complications of Pre-GDM
10. Other Complications
- PIH (Pregnancy Induced Hypertension)
- Polyhydramnios
- Infections (asymptomatic bacteriuria)
- ↑ IR throughout pregnancy
- Fetal macrosomia
11. Management (Antenatal Visits)
At each visit:
- Measure weight
- Check BP
- Urine dipstick for proteinuria
- Blood glucose monitoring:
- 2nd trimester: every 2 weeks
- 3rd trimester: every week
- Fundal examination: rule out diabetic retinopathy
Investigations:
| Type | Details |
|---|---|
| USG | Level I screening → TIFFA at 18-20 wks → Fetal ECHO at 22-24 wks (rule out VSD) |
| Urine | Routine + microscopy every trimester (rule out asymptomatic bacteriuria) ± culture & sensitivity |
| Fetal monitoring | Begin at 32 weeks: NST (weekly), BPS (weekly), Growth scan (3-weekly) |
| Growth scans | At least 2 scans: at 28-30 wks and 34-36 wks (minimum gap: 3 weeks) |
Umbilical Artery Doppler - indications:
- Diabetic vasculopathy
- Development of PIH
Note: All above investigations are done in GDM except Fetal ECHO (no CVS anomaly suspicion in GDM).
12. Treatment
Medical Management:
- Weight counselling
- Medical Nutrition Therapy (MNT) / diet modification
- Insulin - DOC (Drug of Choice) for diabetes in pregnancy
- Low-dose aspirin (to prevent PIH)
Obstetric Management:
- TOP/IOL (Termination / Induction of labour): ≥ 39 weeks
- Mode of delivery: Vaginal (preferred)
- Indication for C-section: Baby weight ≥ 4.5 kg
PART 4: Gestational Diabetes (GDM)
13. GDM Features
- Occurs due to ↑ IR in normoglycemic female
- Complications: Similar to Pre-GDM except no congenital anomalies (GCA)
- Follow-up: Same as Pre-GDM
- Investigations: Same as Pre-GDM except Fetal ECHO not done
14. DIPSI Criteria (Diagnosis of GDM)
Recommended by Govt. of India
Testing schedule:
- 1st test: at 1st antenatal visit
- Repeat: at 24-28 weeks (minimum gap from 1st = 4 weeks)
- If 1st visit is after 28 weeks: Only 1 test
Procedure:
- No fasting needed (universal screening)
- Irrespective of previous meals
- Give 75g glucose in 300 mL water (can add lime) - consume in 5-10 minutes
- Check 2-hour PP levels using plasma-calibrated glucometer
If patient vomits:
- Within 30 minutes → Repeat test on another day
- After 30 minutes → Continue test
These notes cover the complete topic of Diabetes in Pregnancy including pathophysiology, classification, complications, investigations, diagnosis (DIPSI), and management. Let me know if you want any section explained further or need MCQ-style revision points!
What is 40 40 20 rule to control GDM on diet
The 40-40-20 rule is a dietary distribution guideline used in Medical Nutrition Therapy (MNT) for controlling GDM. Here is what it means:
40-40-20 Rule for GDM Diet Control
This rule refers to the distribution of daily calorie intake across meals:
| Meal | Calorie Share |
|---|---|
| Breakfast | 40% |
| Lunch | 40% |
| Dinner | 20% |
The logic behind keeping dinner at only 20% is that insulin sensitivity is lowest at night, so a lighter dinner prevents nocturnal hyperglycemia.
Additional Dietary Guidelines in GDM
- Total calories: ~30-35 kcal/kg/day (based on pre-pregnancy weight)
- Carbohydrate restriction: 40-45% of total calories (complex carbs preferred)
- Protein: ~20-25%
- Fat: ~30-35%
- Frequent small meals are preferred over 3 large meals to avoid post-prandial glucose spikes
- No simple sugars / refined carbohydrates
- High fiber diet - slows glucose absorption
Goal of Dietary Control (A1 GDM)
- FBS < 95 mg/dL
- 2hr PP < 120 mg/dL
- If targets not met on diet alone → escalate to insulin (move from A1 to A2 GDM)
Note: This rule is specifically relevant for the Priscilla White Class A1 (GDM controlled on diet alone). If diet fails to control blood sugar, the patient is reclassified as A2 and started on insulin or metformin.
Let me know if you want MCQ points or more detail on any aspect!
What is sacral agenesis
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Sacral Agenesis (Caudal Regression Syndrome)
Definition
Sacral agenesis is a rare congenital anomaly in which part or all of two or more sacral (and sometimes lumbar) vertebral bodies are absent. It occurs early in fetal development due to failure of ossification of the lowest vertebral segments.
It is the hallmark malformation associated with maternal diabetes (especially poorly controlled pre-gestational diabetes).
- Comprehensive Clinical Nephrology, 7th Ed
Alternate Name
Caudal Regression Syndrome - the broader term that encompasses sacral agenesis along with associated lower limb and visceral anomalies.
Cause / Pathogenesis
| Factor | Detail |
|---|---|
| Primary association | Maternal Type 1 diabetes (poorly controlled) |
| Mechanism | Hyperglycemia → ↑↑ free radicals → cross placenta → disrupt caudal mesoderm development in early embryogenesis |
| Embryologic defect | Incomplete tubularization of neural tube + inadequate mesodermal invagination → arrest of vertebral arch / sacral formation |
| Drug cause | Minoxidil (rare maternal drug exposure) |
| Genetic | Familial cases linked to Currarino syndrome |
| Timing | Occurs during organogenesis (1st trimester) - which is why Pre-GDM (not GDM) causes it |
Key exam point: GDM does NOT cause congenital malformations because hyperglycemia starts at 24-28 weeks, AFTER organogenesis is complete.
Classification (Renshaw / Partial-Complete)
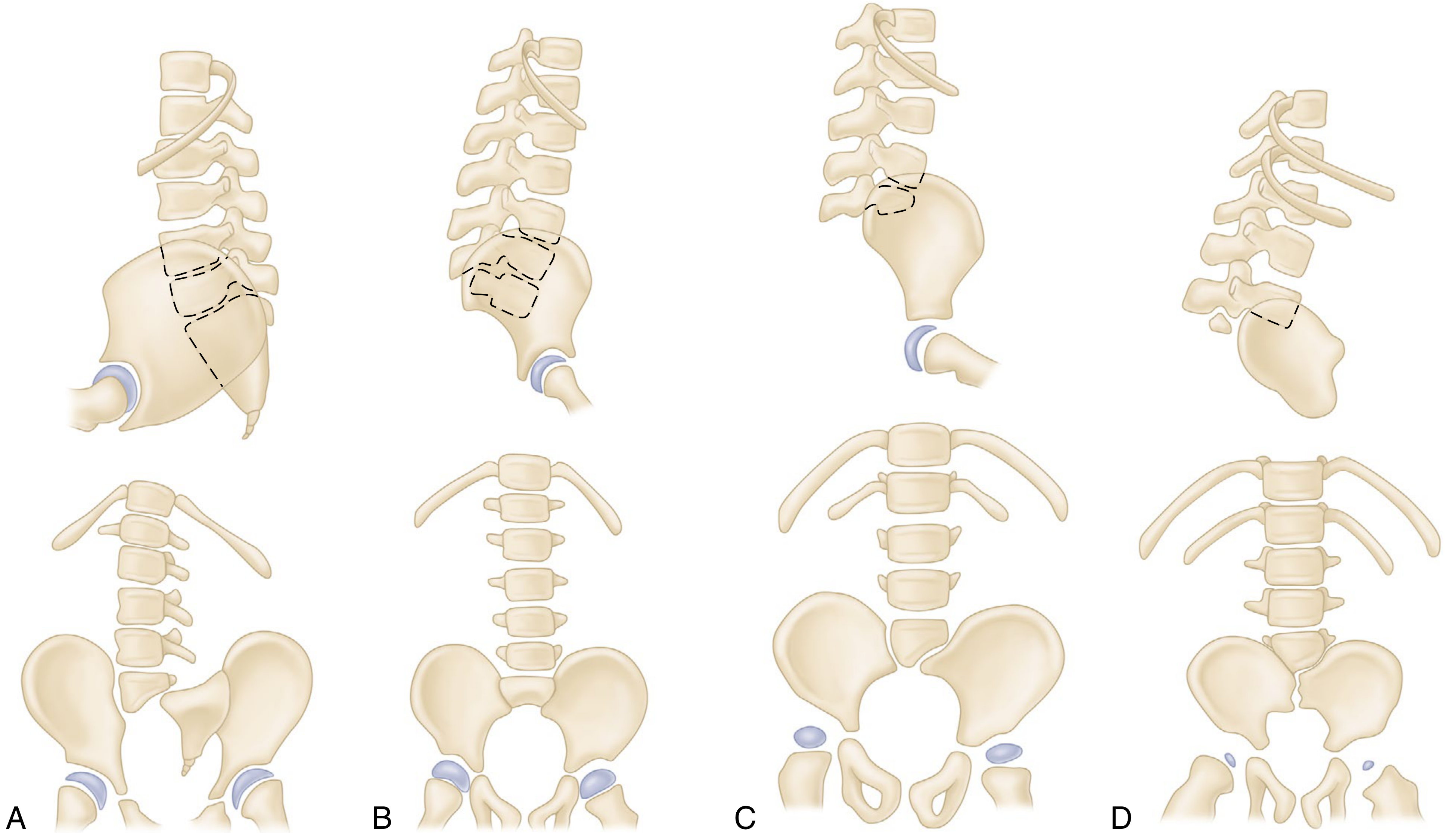
| Type | Description |
|---|---|
| Type I | Total or partial unilateral sacral agenesis |
| Type II | Partial sacral agenesis, bilateral symmetric, stable articulation with normal/hypoplastic S1 |
| Type III | Variable lumbar + total sacral agenesis; ilia articulate with lowest vertebra |
| Type IV | Variable lumbar + total sacral agenesis; lowest vertebra rests above fused ilia |
- Campbell's Operative Orthopaedics, 15th Ed
Clinical Features
Musculoskeletal:
- Characteristic "sitting Buddha" posture of lower limbs
- Foot deformities
- Knee flexion contractures with popliteal webbing
- Hip flexion contractures
- Dislocated hips
- Spinal-pelvic instability
- Scoliosis
- Bone prominence at the last vertebral segment (visible on inspection of back)
- Gross motion between vertebral prominence and pelvis
Neurological:
- Motor power intact down to level of lowest vertebra with pedicles
- Sensation is preserved at up to 3 dermatome levels lower than functional motor control
- Even severe cases may retain some function
Visceral:
- Genitourinary anomalies (very common)
- Neurogenic bladder → urinary incontinence, recurrent UTIs
- Anorectal anomalies
- Stool incontinence
Outcome:
- Significant orthopedic disability (similar to paraplegia)
- Mental function is typically preserved
Antenatal Diagnosis
Ultrasound findings:
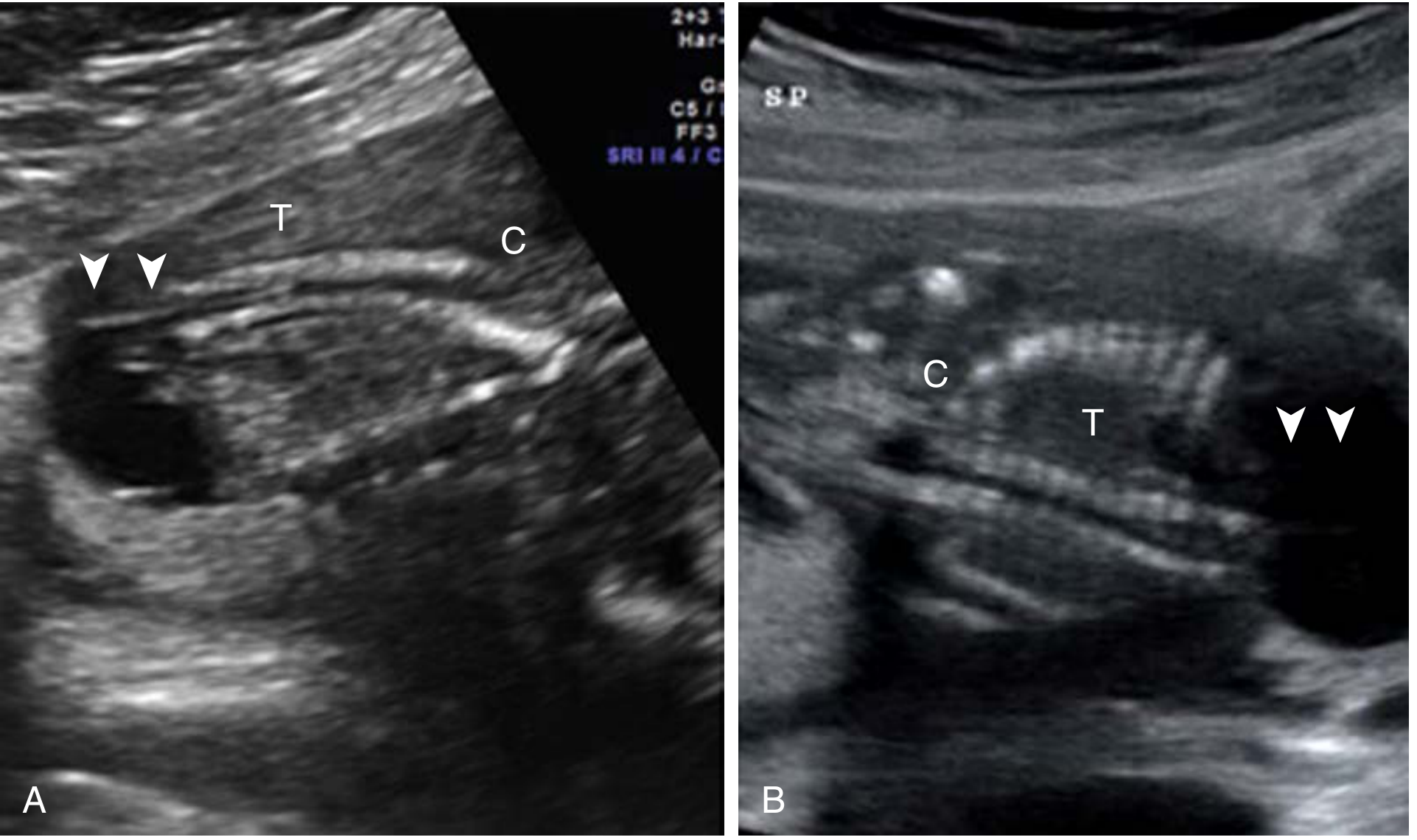
- Abrupt termination of spine at lumbosacral region on USG
- Echolucent mass caudal to defect (accumulated fetal urine)
- In axial view: cord insertion seen anteriorly but spine absent posteriorly
- 3D fetal MRI or 3D skeletal imaging used for confirmation
Screening:
- Detected on TIFFA / targeted anomaly scan at 18-20 weeks
- Amniocentesis + microarray / NIPT considered for karyotype
- Karyotyping is NOT the primary tool (it detects chromosomal anomalies, not GCA)
HbA1c Risk Correlation
| HbA1c | Risk of GCA (including sacral agenesis) |
|---|---|
| < 6.5% | Nil |
| > 6.5% | 3% |
| ≥ 10% | 15-20% |
Prevention
- Strict glycemic control before conception (HbA1c < 6.5%)
- Switch to insulin before/at conception
- Folic acid 400 mcg/day starting 1 month before conception
Quick Exam Summary
| Point | Fact |
|---|---|
| Also called | Caudal Regression Syndrome |
| Caused by | Pre-gestational diabetes (NOT GDM) |
| Mechanism | Hyperglycemia → free radicals → teratogenesis in 1st trimester |
| Classic posture | "Sitting Buddha" |
| Most specific cardiac anomaly in diabetic mother | TGA |
| Mental function | Preserved |
| Detected by | USG / TIFFA at 18-20 weeks |
Explain fetal monitoring
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive data. Here is the full detailed explanation:
Fetal Monitoring - Complete Explanation
Fetal monitoring is the ongoing assessment of fetal well-being during antenatal period and labor, using a combination of clinical and electronic tests. It relies on the principle that fetal neurologic status is closely coupled to cardiovascular reflex responses.
Why Fetal Monitoring?
The goal is to detect fetal hypoxia, acidosis, and uteroplacental insufficiency early enough to intervene. In high-risk pregnancies (diabetes, hypertension, IUGR, post-term), fetal monitoring is intensified.
As noted in our previous discussion on diabetes in pregnancy, fetal monitoring begins at 32 weeks in Pre-GDM/GDM patients, with NST and BPS done weekly.
Methods of Fetal Monitoring
1. Non-Stress Test (NST)
Principle: A healthy fetus with an intact CNS will show acceleration of heart rate with its own movements. FHR (Fetal Heart Rate) acceleration = sign of fetal well-being.
Criteria for REACTIVE NST (Normal/Reassuring):
- At least 2 FHR accelerations in a 20-30 minute period
- Each acceleration must:
- Rise ≥ 15 beats/min above baseline
- Last ≥ 15 seconds
Modification for preterm (<32 weeks):
- Acceleration of ≥ 10 beats/min lasting ≥ 10 seconds (smaller accelerations are normal in younger fetuses)
| Result | Meaning |
|---|---|
| Reactive | Normal - fetus is well oxygenated |
| Non-reactive | Abnormal - may indicate hypoxia, CNS depression, sleep cycle, or drug effect |
Non-reactive NST - causes:
- Fetal sleep cycle (most common - normal cause)
- Prematurity
- Fetal growth restriction (FGR)
- Maternal medications (narcotics, magnesium sulfate)
- CNS abnormality or prior CNS injury
- True fetal compromise
Important: A non-reactive NST with preserved FHR variability and no decelerations is most likely a sleep cycle, NOT fetal compromise. Always back up with BPP.
False negative rate: 1.9 per 1000 fetuses (fetal death within 1 week of a reactive NST).
Frequency in diabetes (from notes): Weekly from 32 weeks.
2. Biophysical Profile Score (BPS/BPP)
Principle: Multiple parameters together are better predictors of fetal well-being than any single parameter.
5 Variables - each scored 2 (normal) or 0 (abnormal):
| Variable | Normal (Score = 2) | Abnormal (Score = 0) |
|---|---|---|
| NST | Reactive (≥2 accelerations) | Non-reactive |
| Fetal Breathing Movements (FBM) | ≥1 episode of ≥30 sec in 30 min | Absent or < 30 sec |
| Fetal Movements (FM) | ≥3 discrete body/limb movements in 30 min | < 3 movements |
| Fetal Tone (FT) | ≥1 episode of active limb extension + return to flexion | Absent or slow return |
| Amniotic Fluid Volume (AFV) | Single deepest pocket ≥ 2 cm in 2 perpendicular planes | Pocket < 2 cm |
Maximum total score = 10
Interpretation of BPP Score:
| Score | Interpretation | Action |
|---|---|---|
| 8-10 | Normal, no fetal compromise | Routine care |
| 6 | Equivocal | Repeat in 24 hrs; consider delivery if at term |
| 4 | Suspected fetal compromise | Delivery in most cases |
| 0-2 | Strong evidence of fetal compromise | Immediate delivery |
Modified BPP: NST + Amniotic fluid volume only (simpler, faster screening).
3. Amniotic Fluid Volume (AFV) Assessment
Principle: Decreased amniotic fluid (oligohydramnios) in an anatomically normal fetus = fetal oliguria = redistribution of blood flow away from kidneys = uteroplacental insufficiency.
Measurement technique (for BPP):
- Transducer held vertical to maternal abdomen
- Measure the maximum vertical depth of a clear fluid pocket
- Rotate 90° to confirm it is a true 3D pocket
- The 2×2 pocket rule: pocket must be ≥ 2 cm deep in at least 2 intersecting planes
Amniotic Fluid Index (AFI): Sum of deepest pockets in all 4 quadrants.
- Normal AFI: 8-24 cm
- Oligohydramnios: AFI < 5 cm
- Polyhydramnios: AFI > 24 cm
Avoid using continuous color Doppler when measuring - can falsely suggest oligohydramnios by mistaking cord loops for fluid.
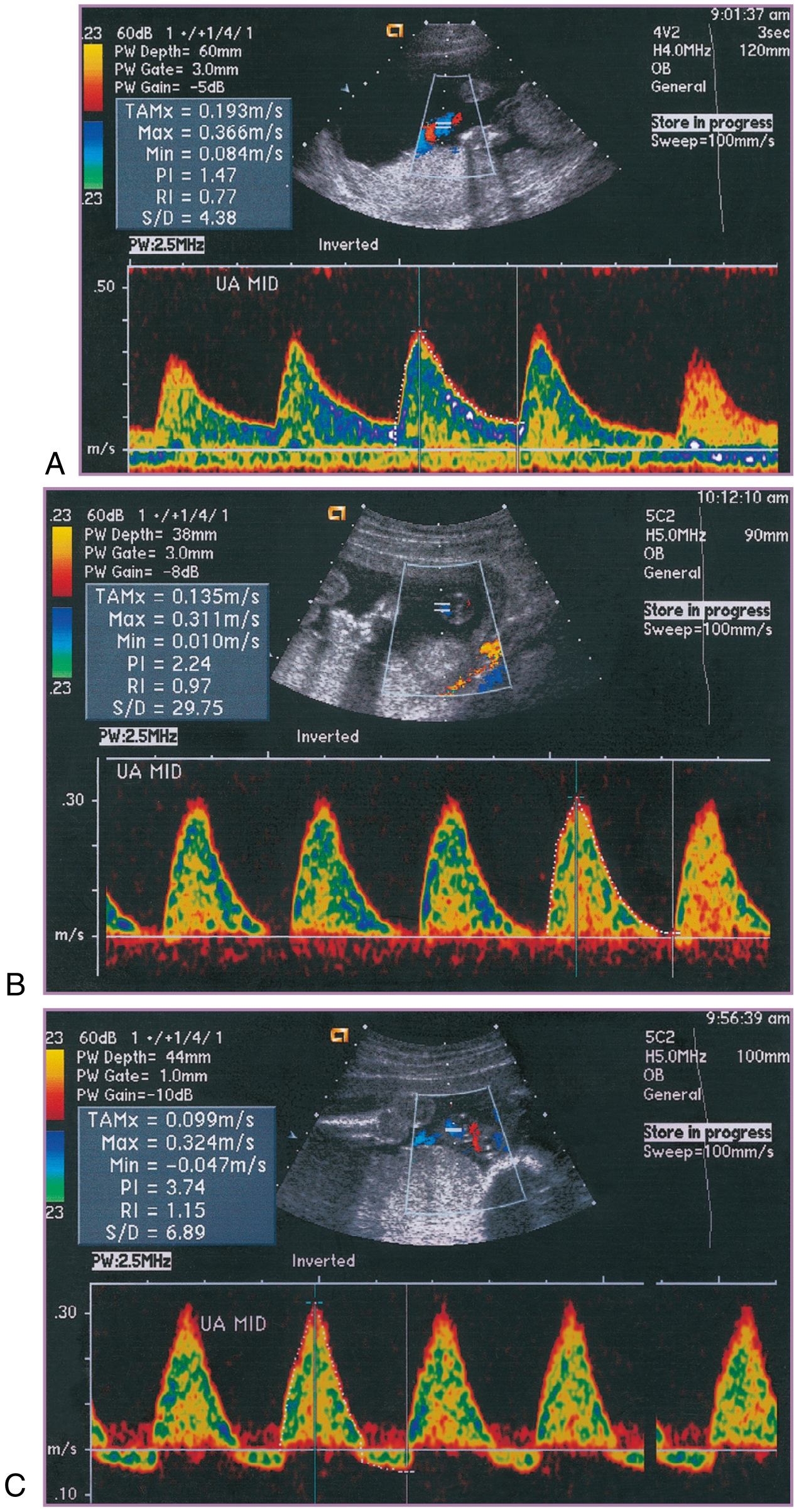
4. Umbilical Artery Doppler Velocimetry
Principle: Umbilical arteries carry no somatic branches - they purely mirror downstream placental resistance. Normally, resistance falls progressively through pregnancy as more placental vessels develop.
Indications in diabetes (from notes):
- Diabetic vasculopathy
- Development of PIH
Progression of abnormality:
| Stage | Finding | Significance |
|---|---|---|
| Normal | Positive end-diastolic flow, falling resistance through pregnancy | Well-being |
| Early compromise | Elevated S/D ratio (↑ resistance) | Placental dysfunction |
| Worsening | AEDV - Absent End-Diastolic Velocity | Severe compromise |
| Critical | REDV - Reversed End-Diastolic Velocity | Imminent fetal death, deliver immediately |
S/D ratio (Systolic/Diastolic): Falls normally from 1st to 3rd trimester.
5. Fetal Heart Rate (FHR) Monitoring / Cardiotocography (CTG)
Used in labor. Assesses fetal heart rate patterns continuously.
Key FHR parameters:
| Parameter | Normal |
|---|---|
| Baseline FHR | 110-160 bpm |
| Variability | 6-25 bpm (moderate variability = reassuring) |
| Accelerations | ≥15 bpm rise for ≥15 sec (reactive) |
| Decelerations | Absent / early only (late/variable = concerning) |
Types of decelerations:
| Type | Timing relative to contraction | Cause | Significance |
|---|---|---|---|
| Early | Mirror contraction (simultaneous) | Head compression | Benign |
| Late | After peak of contraction | Uteroplacental insufficiency | Pathological |
| Variable | No fixed relationship | Cord compression | May be pathological if persistent |
FHR Classification (ACOG):
- Category I (Normal): Baseline 110-160, moderate variability, no late/variable decels
- Category II (Indeterminate): Does not fit I or III
- Category III (Abnormal): Sinusoidal pattern OR absent variability with recurrent late/variable decelerations → immediate action
6. Growth Scan (Fetal Biometry on USG)
Purpose: Detect macrosomia or IUGR.
In diabetic pregnancy (from notes):
- Done 3-weekly (to rule out polyhydramnios and macrosomia)
- At least 2 growth scans:
- At 28-30 weeks
- At 34-36 weeks
- Minimum gap between scans: 3 weeks
Parameters measured:
- BPD (Biparietal Diameter)
- HC (Head Circumference)
- AC (Abdominal Circumference)
- FL (Femur Length)
- Estimated Fetal Weight (EFW)
Summary Table: Fetal Monitoring Schedule in Diabetes
| Test | When | Frequency |
|---|---|---|
| NST | From 32 weeks | Weekly |
| BPS (Biophysical Score) | From 32 weeks | Weekly |
| Growth scan | 28-30 wks & 34-36 wks | 3-weekly (min 2 scans) |
| Umbilical artery Doppler | If vasculopathy / PIH | As indicated |
| TIFFA | 18-20 weeks | Once |
| Fetal ECHO | 22-24 weeks (Pre-GDM only) | Once |
Key Exam Points
| Point | Fact |
|---|---|
| NST starts at | 32 weeks in diabetic pregnancy |
| Reactive NST | ≥2 accelerations of ≥15 bpm for ≥15 sec |
| Most common cause of non-reactive NST | Fetal sleep cycle (normal) |
| BPP maximum score | 10 |
| Score 8-10 | Normal |
| Score ≤4 | Deliver |
| Most ominous Doppler finding | REDV (Reversed End-Diastolic Velocity) |
| Oligohydramnios on BPP | Deepest pocket < 2 cm |
| Fetal ECHO NOT done in | GDM (only Pre-GDM) |
- Creasy & Resnik's Maternal-Fetal Medicine, Principles and Practice
Make summary of cvs from ghai textbook of peditrics
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Unfortunately, Ghai's Textbook of Pediatrics is not available in the medical library. The library only has two pediatric books:
- The Harriet Lane Handbook (Johns Hopkins, 23rd ed.)
- Red Book 2021 (Committee on Infectious Diseases)
What I Can Do Instead
Here are your options:
1. CVS summary from a different pediatric source - I can pull CVS (Cardiovascular System) content from Harriet Lane Handbook or any other available cardiology textbook (e.g., Braunwald's Heart Disease).
2. CVS summary based on Ghai topics from my training knowledge - I can write a detailed topic-wise summary covering what Ghai covers in its CVS chapter (congenital heart diseases, rheumatic fever, cardiac failure in children, etc.) based on my knowledge of the book's content.
3. Upload your Ghai PDF - If you have a PDF of the relevant Ghai CVS chapter, you can upload it and I will extract and summarize it for you.
Which would you prefer? Or if you want all key CVS pediatric topics (ASD, VSD, TOF, PDA, rheumatic fever, cardiac failure) summarized in detail, I can do that right away from available sources combined with Ghai-style content.
This is a shared conversation. Sign in to Orris to start your own chat.