Diffusion tand second gas effect for 5 marks with millers as reference
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
I now have everything needed from Miller's. Here is the complete, exam-ready answer:
Diffusion Hypoxia and Second Gas Effect
Reference: Miller's Anesthesia, 10th Edition (Miller's) - Chapter 18
Second Gas Effect
Background - The Concentration Effect (prerequisite concept)
When an inhaled anesthetic makes up a large fraction of the inspired gas mixture, its rapid uptake into pulmonary blood reduces alveolar gas volume. Because volume shrinks rather than concentration alone falling, the alveolar partial pressure of that gas drops less than the fractional amount taken up. This is the concentration effect - at the extreme of 100% inspired gas, uptake reduces volume without reducing partial pressure at all.
"The higher the inspired anesthetic concentration, the less it diminishes because of uptake (the concentration effect)."
- Miller's Anesthesia, 10e, Key Points, p. 1919
Definition
The second gas effect is the phenomenon by which the rapid uptake of a high-concentration "first gas" (N2O) simultaneously increases the alveolar concentration and partial pressure of any co-administered "second gas" (e.g., a volatile agent like isoflurane, or O2), thereby accelerating the uptake of that second gas into blood.
Mechanism (Miller's Fig. 18.8)
Consider the classic example given in Miller's:
- Inspired mixture: 66% N2O, 33% O2, 1% isoflurane
- Cardiac output: 5 L/min
- Initial N2O uptake rate: ~1550 mL/min (very rapid due to high concentration and large partial pressure gradient)
When approximately 50% of the inspired N2O is rapidly taken up into pulmonary blood:
- The total alveolar gas volume shrinks by ~33%
- To maintain alveolar volume (constant FRC + expiratory volumes), additional fresh inspired gas rushes in from the circuit - this is the "augmented ventilation" component
- The net result: alveolar N2O falls only from 66% → 49.25% (much less than the 50% uptake fraction)
- Simultaneously, alveolar O2 rises from 33% → 49.25% and alveolar isoflurane rises from 1.0% → 1.5%
This concentration of the second gases (isoflurane, O2) in the alveolus increases their partial pressure gradients into pulmonary blood, accelerating their uptake.
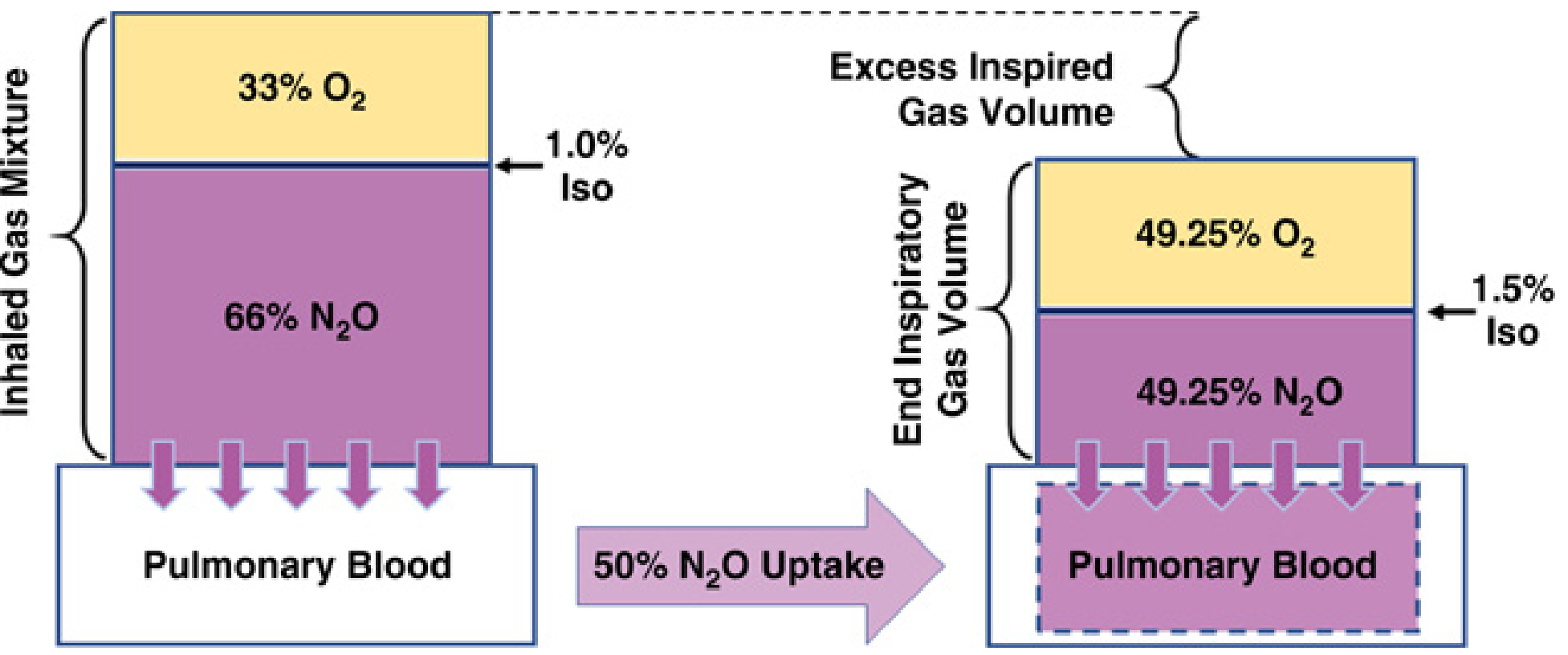
FIG. 18.8 from Miller's Anesthesia, 10e, p. 1952-1953 - Concentration and second gas effects
Two Components of the Second Gas Effect
As per Miller's, the second gas effect works via two mechanisms:
| Component | Mechanism |
|---|---|
| Concentration effect on second gas | Shrinkage of alveolar volume concentrates isoflurane and O2 |
| Augmented ventilation | Inflow of fresh gas to replace absorbed N2O brings in more second gas from the circuit |
Clinical Significance
- Speeds induction: The rise in alveolar partial pressure of the volatile agent is faster when N2O is co-administered at high concentrations
- Effect greater in arterial blood than expired gas: Due to ventilation-perfusion heterogeneity
- Influenced by blood solubility of volatile agents and by the rate of N2O uptake
- Demonstrated in humans and confirmed by mathematical modeling studies
- The effect is "significant at relatively low rates of N2O uptake" and is greater in arterial blood than in expired gas (Miller's, p. 1948)
Diffusion Hypoxia
Definition
Diffusion hypoxia (also called Fink effect) is a clinical phenomenon that occurs during the first 5-10 minutes after discontinuation of N2O anaesthesia, in which rapid outgassing of N2O from blood into the alveoli causes dilution of alveolar oxygen, potentially producing arterial hypoxemia.
"Diffusion hypoxia is another sequelae of rapid outgassing from the tissues of patients anesthetized with N2O. During the initial 5 to 10 minutes after discontinuation of anesthesia, the flow of N2O from blood into the alveoli can be several liters per minute, resulting in dilution of alveolar oxygen."
- Miller's Anesthesia, 10e, p. 1977
Mechanism
This is essentially the reverse of the concentration/second gas effect:
- At the end of anaesthesia, N2O diffuses rapidly out of blood back into alveoli (several liters/minute)
- This large volume of N2O in the alveolus dilutes alveolar O2 (reduces FiO2 and PAO2)
- It also dilutes alveolar CO2 (reduces PACO2), thereby blunting the hypercapnic respiratory drive
- Residual anaesthetic-induced respiratory depression is also present at this time
Triple-Hit Mechanism Leading to Desaturation
As described in Miller's, three factors combine:
| Factor | Effect |
|---|---|
| Residual CNS/respiratory depression from anaesthesia | Reduced respiratory drive and effort |
| Reduced alveolar FO2 (N2O dilution of O2) | Lower PAO2 → lower PaO2 |
| Reduced alveolar PCO2 | Blunted hypercapnic drive → hypoventilation |
The combination results in hypoventilation and oxyhemoglobin desaturation.
Prevention
Miller's states this outcome is "avoided by routinely providing supplemental O2 for the first 5 to 10 minutes of recovery, together with vigilant attention to respiration and oxygenation."
It is also listed in Miller's Box 76.3 as a factor contributing to postoperative arterial hypoxemia (p. 1977).
Summary Comparison
| Feature | Second Gas Effect | Diffusion Hypoxia |
|---|---|---|
| Timing | Induction phase | Recovery phase (first 5-10 min) |
| Direction of N2O movement | Blood ← Alveolus (uptake) | Blood → Alveolus (outgassing) |
| Effect on volatile agent/O2 | Increases alveolar concentration | Decreases alveolar O2 |
| Clinical relevance | Faster induction | Hypoxemia risk |
| Prevention/use | Clinically useful (faster onset) | Give supplemental O2 at emergence |
Source: Miller's Anesthesia, 2-Volume Set, 10th Edition - Chapter 18 (Inhaled Anesthetic Pharmacokinetics), pp. 1945-1953 and p. 1977
This is a shared conversation. Sign in to Orris to start your own chat.