Give detail about antidepressants
Reading File
Finding Sources
Searching PubMed
"antidepressants"[MeSH Terms] AND "depression"[MeSH Terms]
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Here is a detailed, comprehensive overview of antidepressants organized by class, mechanism, indications, and key clinical considerations.
Antidepressants - Detailed Overview
General Mechanism
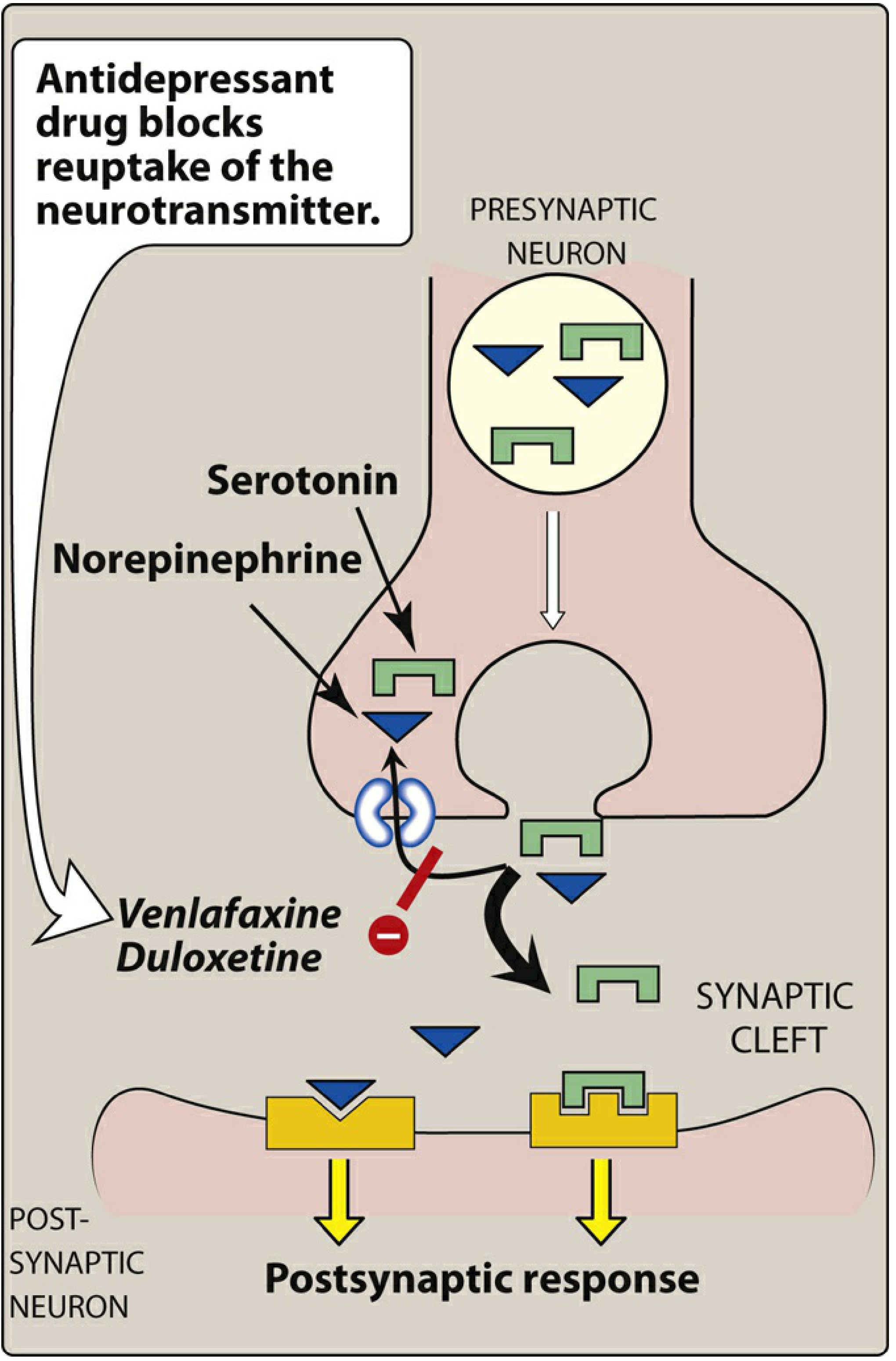
The core principle shared by most antidepressants is increasing monoamine neurotransmitter availability in the synapse. The "amine hypothesis" of depression posits that depressive illness is associated with a deficiency of noradrenergic or serotonergic transmission. Antidepressants largely work by blocking the reuptake transporter (presynaptic plasma transporter) that would normally clear these neurotransmitters from the synaptic cleft.
Onset of therapeutic effect is typically 2-4 weeks for all classes, even though neurotransmitter changes begin immediately. This lag is thought to reflect downstream neuroplastic adaptations (receptor desensitization, neurogenesis).
Classification & Major Drug Classes
Class Dosage Reference Table
| Class | Generic (Brand) | Daily Dose (mg) |
|---|---|---|
| SSRI | Fluoxetine (Prozac) | 20-80, or 90 weekly |
| Sertraline (Zoloft) | 50-200 | |
| Paroxetine (Paxil) | 20-50 | |
| Citalopram (Celexa) | 20-40 | |
| Escitalopram (Lexapro) | 10-20 | |
| Fluvoxamine (Luvox) | 50-300 | |
| SNRI | Venlafaxine (Effexor XR) | 37.5-225 |
| Duloxetine (Cymbalta) | 20-60 | |
| Desvenlafaxine (Pristiq) | 50 | |
| Levomilnacipran (Fezima) | 40-120 | |
| TCA | Amitriptyline | 75-150 |
| Imipramine (Tofranil) | 75-200 | |
| Nortriptyline (Pamelor) | 75-100 | |
| Desipramine (Norpramin) | 75-200 | |
| Clomipramine (Anafranil) | 25-250 | |
| MAOI | Phenelzine (Nardil) | 15-90 |
| Tranylcypromine (Parnate) | 30-60 | |
| Isocarboxazid (Marplan) | 10-60 | |
| Atypicals | Bupropion (Wellbutrin) | 150-450 |
| Mirtazapine (Remeron) | 15-60 | |
| Trazodone (Desyrel) | 150-400 | |
| Vortioxetine (Trintellix) | 5-20 | |
| Vilazodone (Viibryd) | 10-40 |
- Creasy & Resnik's Maternal-Fetal Medicine, Table 67.3
1. Selective Serotonin Reuptake Inhibitors (SSRIs)
Mechanism: Block the serotonin transporter (SERT) on presynaptic terminals, increasing serotonin concentration in the synapse. They have minimal effect on norepinephrine or dopamine transporters.
Drugs: Fluoxetine, sertraline, paroxetine, citalopram, escitalopram, fluvoxamine, vilazodone
FDA-Approved Indications (by drug):
| Indication | SSRI(s) Approved |
|---|---|
| Major Depressive Disorder | All SSRIs (adults); fluoxetine (pediatric) |
| Generalized Anxiety Disorder | Escitalopram, paroxetine |
| OCD | Fluoxetine, fluvoxamine, paroxetine, sertraline (adults + pediatric) |
| Panic Disorder | Fluoxetine, paroxetine, sertraline |
| PTSD | Paroxetine, sertraline |
| Social Anxiety Disorder | Paroxetine, sertraline |
| Bulimia Nervosa | Fluoxetine (60 mg/day) |
| Premenstrual Dysphoric Disorder (PMDD) | Fluoxetine, paroxetine, sertraline |
- Kaplan & Sadock's Synopsis of Psychiatry, Table 21-15
Key points:
- All SSRIs are equally effective for depression; choice depends on pharmacokinetics, side effects, and individual response
- Fluvoxamine is NOT FDA-approved as an antidepressant in the US (marketing decision), but is used as such globally
- SSRIs are first-line for most indications due to favorable safety profiles vs. TCAs/MAOIs
Adverse Effects of SSRIs:
- GI: Nausea, diarrhea, GI upset (most common, especially early)
- Sexual dysfunction: Anorgasmia, decreased libido (very common; up to 30-50%)
- CNS: Insomnia, agitation, restlessness, drowsiness
- Weight: Initial weight loss possible, but long-term weight gain with chronic use
- Anticholinergic (mainly paroxetine): Dry mouth, constipation, sedation
- Platelet dysfunction: Impaired aggregation - increased bleeding risk; avoid with NSAIDs/anticoagulants without GI protection
- Hyponatremia/SIADH: Especially in elderly or those on diuretics
- Endocrine: Increased prolactin, galactorrhea, mammoplasia (reversible)
- Glucose disturbance: Acute hypoglycemia; monitor diabetics
- Rash: About 4% of patients; rarely progresses to pulmonary involvement
2. Serotonin-Norepinephrine Reuptake Inhibitors (SNRIs)
Mechanism: Block both SERT and the norepinephrine transporter (NET), increasing both serotonin and norepinephrine in the synapse.
Drugs: Venlafaxine, duloxetine, desvenlafaxine, levomilnacipran
Indications:
- Major depressive disorder
- Generalized anxiety disorder
- Neuropathic pain and fibromyalgia (duloxetine)
- Chronic musculoskeletal pain (duloxetine)
- Stress urinary incontinence (duloxetine in some countries)
- PTSD, panic disorder (venlafaxine)
Adverse effects: Similar to SSRIs plus hypertension (especially venlafaxine at higher doses), sweating, and urinary hesitancy (norepinephrine effect).
3. Tricyclic Antidepressants (TCAs)
Mechanism: Block reuptake of both norepinephrine and serotonin. Divided into:
- Tertiary amines (amitriptyline, imipramine, doxepin, clomipramine, trimipramine): Inhibit reuptake of both serotonin AND norepinephrine
- Secondary amines (desipramine, nortriptyline, amoxapine, maprotiline, protriptyline): Preferentially block norepinephrine reuptake
Indications:
- Major depressive disorder (especially anergic depressions with early morning awakening, decreased appetite/libido)
- Neuropathic pain and chronic pain (amitriptyline is the most commonly used)
- OCD (clomipramine - gold standard)
- Enuresis (imipramine)
Adverse Effects - prominent due to anticholinergic activity:
- Orthostatic hypotension
- Urinary retention
- Dry mouth
- Blurred vision
- Constipation
- Sedation and cognitive impairment
- Cardiac arrhythmia risk (QT prolongation) - most dangerous in overdose
- Lowering of seizure threshold
Contraindications: Should NEVER be combined with MAOIs - can cause life-threatening interactions. Also contraindicated in recent MI and bundle branch block.
- Adams and Victor's Principles of Neurology, 12th Edition
4. Monoamine Oxidase Inhibitors (MAOIs)
Mechanism: Inhibit monoamine oxidase (MAO), the enzyme that breaks down monoamines (serotonin, norepinephrine, dopamine, tyramine) in the presynaptic terminal. This results in increased availability of all monoamines.
- MAO-A inhibitors (phenelzine, tranylcypromine, isocarboxazid): Irreversible, non-selective
- MAO-B inhibitors (selegiline transdermal): Relatively selective; also used in Parkinson's disease
Indications:
- Atypical depression (mood reactivity, hypersomnia, leaden paralysis, rejection sensitivity)
- Refractory depression
- Social anxiety disorder
- Panic disorder
Adverse Effects:
- Orthostatic hypotension, urinary retention, skin rashes, tachycardia, sweating
- Significant weight gain
- Impotence, jaundice
- Risk of hypertensive crisis if combined with tyramine-containing foods or sympathomimetics
Critical Drug-Food Interactions (MAOI):
MAOIs require strict dietary restrictions. Tyramine-rich foods that must be avoided include:
- Aged cheeses, red wine, beer
- Pickled herring, sardines, sausages
- Certain preserved meats/fish
- Sympathomimetic cold remedies, nasal sprays, nose drops
Critical Drug-Drug Interactions (MAOI):
Combining MAOIs with any of these is potentially fatal:
- TCAs or SSRIs (risk of serotonin syndrome)
- CNS stimulants
- Phenothiazines
- Meperidine (Demerol) - can cause respiratory depression, hyperpyrexia, profound hypotension
5. Atypical Antidepressants
Bupropion (Wellbutrin)
- Mechanism: Norepinephrine-dopamine reuptake inhibitor (NDRI); no serotonergic activity
- Key advantages: No sexual dysfunction (unlike SSRIs/SNRIs); promotes weight loss; approved for smoking cessation (Zyban)
- Contraindication: Seizure disorders, bulimia/anorexia (lowers seizure threshold); avoid in patients using MAOIs
Mirtazapine (Remeron)
- Mechanism: Alpha-2 adrenergic antagonist ("cuts the brake" on norepinephrine release) - increases NE and 5-HT by a different mechanism than reuptake inhibition
- Key advantages: Highly sedating - useful when insomnia or poor appetite is prominent; weight gain is a feature, not a bug, in malnourished patients
- Adverse effects: Sedation, weight gain, dry mouth
Trazodone (Desyrel)
- Mechanism: Serotonin reuptake inhibition + 5-HT2 antagonism
- Clinical use: Mainly used at low doses for insomnia rather than as primary antidepressant; also used in PTSD
- Adverse effect: Priapism (rare but serious)
Vortioxetine (Trintellix)
- Mechanism: Multimodal - SERT inhibition + 5-HT1A agonism + 5-HT3/5-HT7 antagonism; pro-cognitive actions via 5HT1B heteroreceptors on dopamine, acetylcholine, histamine, and NE terminals
- Advantage: Cognitive benefits especially in depression-related cognitive dysfunction
Nefazodone
- Mechanism: Multimodal - weak serotonin + norepinephrine reuptake inhibition + 5-HT2 postsynaptic antagonism
- Concern: Risk of hepatotoxicity (withdrawn from some markets)
Serotonin Syndrome
A potentially fatal condition caused by excessive serotonergic activity, most commonly from combining an SSRI/SNRI with an MAOI, L-tryptophan, or lithium.
Clinical progression (in order of severity):
- Diarrhea
- Restlessness
- Extreme agitation, hyperreflexia, autonomic instability, rapid vital sign fluctuations
- Myoclonus, seizures, hyperthermia, shivering, rigidity
- Delirium, coma, status epilepticus, cardiovascular collapse, death
Treatment: Remove offending agents + supportive care (cyproheptadine, benzodiazepines, cooling blankets, mechanical ventilation if needed).
- Kaplan & Sadock's Synopsis of Psychiatry
Discontinuation Syndrome
Abrupt withdrawal of antidepressants - especially shorter-half-life agents like paroxetine or fluvoxamine - causes a discontinuation syndrome characterized by:
- "FINISH" symptoms: Flu-like symptoms, Insomnia, Nausea, Imbalance/dizziness, Sensory disturbances (electric-shock sensations/"brain zaps"), Hyperarousal/anxiety
- Onset within 1-3 days of stopping
- Usually self-limiting in 1-2 weeks but can last longer
Fluoxetine has the longest half-life (~1-6 days, active metabolite up to 2 weeks) and rarely causes discontinuation syndrome.
Prevention: Always taper antidepressants gradually rather than stopping abruptly.
Treatment Strategy
- First-line: SSRIs (best tolerability, safety in overdose, broad spectrum)
- Second-line: SNRIs, bupropion, mirtazapine
- Third-line / augmentation: Add aripiprazole, buspirone, lithium, or combine antidepressants
- Refractory: TCAs, MAOIs, or combination strategies
- Special populations: TCAs preferred for neuropathic pain; clomipramine for OCD; bupropion when sexual side effects or weight gain are concerns
For severe or melancholic depression, TCAs may outperform SSRIs.
- Swanson's Family Medicine Review
Special Considerations
Pediatric Use
- Fluoxetine is the only SSRI FDA-approved for pediatric depression
- All antidepressants carry a black-box warning for increased suicidality in patients under 25 years old
- SSRIs approved for pediatric OCD: fluoxetine, fluvoxamine, sertraline
Pregnancy
- SSRIs are most frequently prescribed during pregnancy; information is greatest for SSRIs, venlafaxine, and TCAs
- MAOIs are rarely used in pregnancy
- Risks include: possible miscarriage association (absolute risk small), neonatal adaptation syndrome, persistent pulmonary hypertension (rare)
- Always weigh risk of untreated depression vs. medication exposure
Cardiovascular Disease
- SSRIs (sertraline, paroxetine, fluoxetine) are preferred; generally safe
- Avoid TCAs in recent MI or conduction disease (arrhythmia risk)
- Mirtazapine, bupropion, venlafaxine, duloxetine are alternatives for CVD patients
Elderly
- Use caution with SSRIs due to SIADH/hyponatremia risk
- Avoid TCAs (falls, arrhythmia, urinary retention, confusion)
- Start low, go slow
Sources: Kaplan & Sadock's Synopsis of Psychiatry; Adams and Victor's Principles of Neurology (12th ed.); Lippincott Illustrated Reviews: Pharmacology; Creasy & Resnik's Maternal-Fetal Medicine; Swanson's Family Medicine Review; Bradley and Daroff's Neurology in Clinical Practice
This is a shared conversation. Sign in to Orris to start your own chat.