Taenia solium
Reading File
Finding Sources
Finding Sources
Searching PubMed
"Taenia solium" AND neurocysticercosis
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information from multiple authoritative textbooks. Let me compile the full answer.
Taenia solium (Pork Tapeworm)
Classification and Morphology
Taenia solium is a cestode (flatworm) with a flat, segmented, ribbon-like body (strobila). Its key morphological features:
- Scolex (head): Four muscular cup-shaped suckers plus a rostellum with a double crown of hooklets (this distinguishes it from T. saginata, which has no hooks - hence T. solium = "armed" tapeworm)
- Adult worm length: 10-20 feet (some sources up to 30 feet)
- Proglottids: Terminal proglottids are ~2 cm long, 0.5-1 cm wide, 1-2 mm thick. Gravid proglottids contain fewer than 13 uterine branches (vs ≥14 in T. saginata) - key distinguishing feature
- Ova: 40 µm diameter, surrounded by brown radial striations, embryos with 6 hooks - morphologically identical to T. saginata eggs
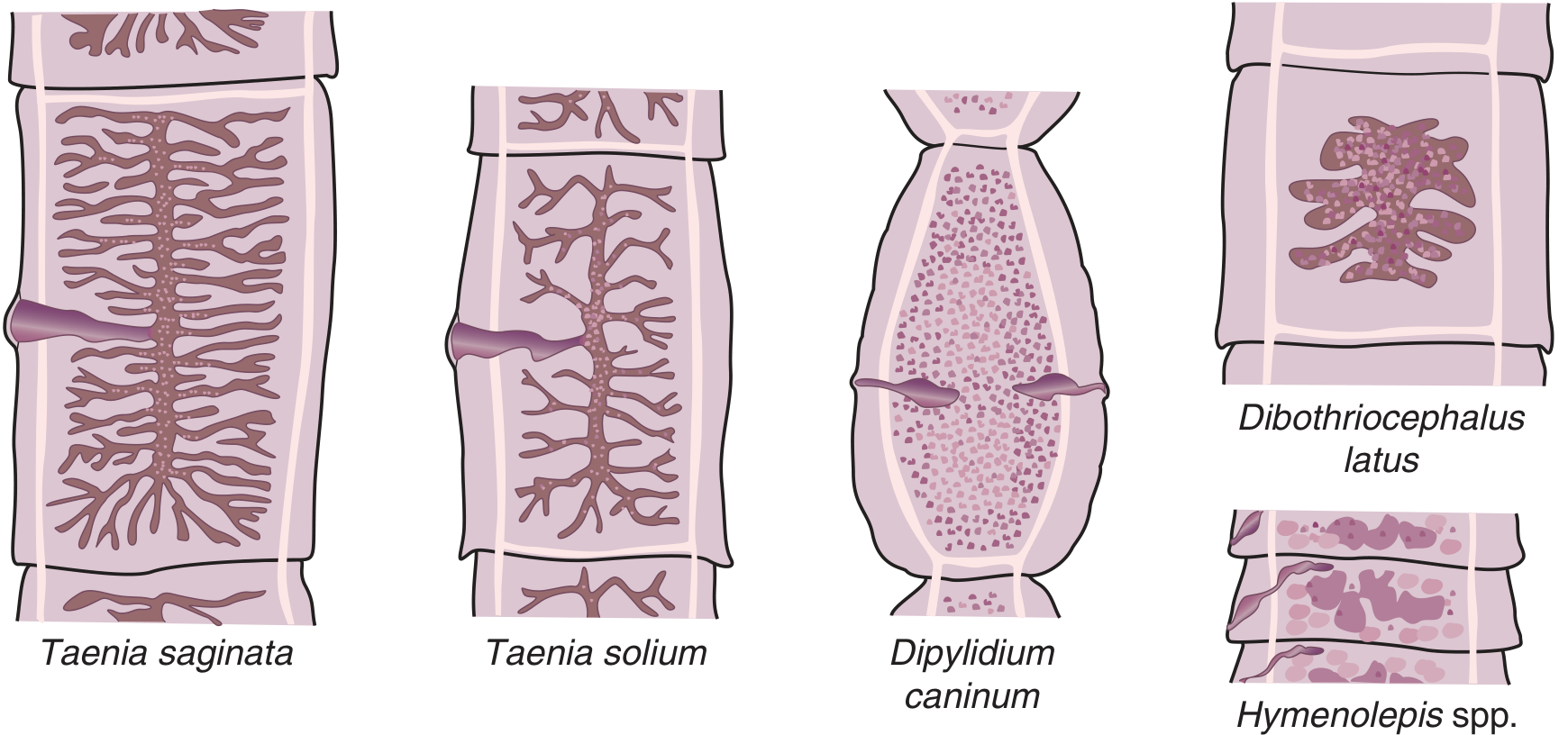
Figure: Gravid proglottid comparison - note T. solium has fewer, less branched uterine laterals compared to T. saginata (Tietz Textbook of Laboratory Medicine, 7th Ed)
Life Cycle
T. solium is unique in that humans can act as either definitive host OR intermediate host.
Route 1 - Taeniasis (Definitive Host)
- Human ingests undercooked pork containing cysticerci (larval cysts)
- Cysticercus evaginates in the small intestine, scolex attaches to intestinal wall
- Proglottids form at base of scolex, mature into an adult tapeworm
- Gravid proglottids and eggs are shed in stool
- Pigs (intermediate host) ingest eggs from fecally contaminated environment
- Eggs hatch → oncospheres penetrate pig gut wall → disseminate hematogenously → encyst in muscle as cysticerci
Route 2 - Cysticercosis (Accidental Intermediate Host)
- Human ingests eggs (not larvae) from fecally contaminated food, water, or via autoinfection
- Eggs hatch → oncospheres penetrate intestinal wall → hematogenous spread
- Lodge in tissues (brain, muscle, subcutaneous tissue, eye) → develop into cysticerci
- Critical: The egg-ingestion route does NOT require pork consumption - vegetarians and people who never eat pork can get cysticercosis from contact with a tapeworm carrier (e.g., infected household worker)
Epidemiology
- Endemic regions: Latin America, sub-Saharan Africa, South/Southeast Asia, Eastern Europe, China, India, Pakistan
- Correlates with poor sanitation, free-ranging pigs, and unregulated slaughter practices
- An estimated 370,000 symptomatic new cases of taeniasis/cysticercosis occurred in 2010, with >28,000 attributed deaths
- Leading cause of acquired epilepsy worldwide - WHO estimates 30% of epilepsy cases in endemic areas are attributable to cysticercosis
- Both conditions are WHO Neglected Tropical Diseases (NTDs)
- In the US, cases are mainly seen in immigrants from endemic countries, with rare autochthonous transmission
Disease Manifestations
1. Taeniasis (intestinal infection with adult worm)
- Usually asymptomatic or mild: nausea, abdominal discomfort, anorexia, pruritus ani
- Motile proglottids may be noted in stool or exiting the anus
- Far less clinically significant than cysticercosis
2. Cysticercosis / Neurocysticercosis (larval tissue infection)
Cysticerci can form in any organ; clinical presentation depends on location:
| Location | Manifestation |
|---|---|
| Brain parenchyma | Seizures (most common), headache, focal deficits |
| Cerebral ventricles | Obstructive hydrocephalus, raised ICP |
| Subarachnoid space | Racemose cysticercosis, meningitis, arachnoiditis, vasculitis |
| Spine | Myelopathy |
| Eye | Visual disturbances, blindness |
| Subcutaneous/muscle | Palpable nodules, calcifications |
Neurocysticercosis (NCC) is the most serious form. Viable cysts evade immunity by producing taeniaestatin and paramyosin, which inhibit complement activation. When cysts degenerate, the host mounts an inflammatory response, causing edema, seizures, and scarring.
Pathological stages of cysticerci:
- Viable (vesicular): thin translucent bladder with invaginated scolex, little inflammation
- Degenerating (colloidal): turbid fluid, surrounding edema and enhancement on MRI
- Granular: cyst collapses, granuloma forms
- Calcified: end-stage, may continue to cause perilesional edema and seizures
Diagnosis
Taeniasis
- Stool microscopy: identify ova (identical to T. saginata) or proglottids
- Proglottid morphology: count uterine branches to distinguish species (<13 = T. solium, ≥14 = T. saginata)
Cysticercosis / Neurocysticercosis
- Neuroimaging (CT/MRI): key modality - detects cystic lesions, scolex ("hole-with-dot" sign), calcifications, hydrocephalus, enhancement
- Serology: Enzyme-Linked Immunoelectrotransfer Blot (EITB) using lentil lectin-purified glycoproteins is >99% specific and sensitive for multiple cysts (less sensitive for single or calcified lesions). Crude antigen ELISAs have high false-positive/negative rates and should be avoided
- Biopsy: histologic demonstration of parasite (absolute criterion)
- Subcutaneous nodules: surgical removal and examination
Del Brutto Revised Diagnostic Criteria (2017) - Harrison's 22e
Absolute criteria (any one confirms diagnosis):
- Histologic demonstration from brain/spinal cord biopsy
- Visualization of subretinal cysticercus
- Scolex within cystic lesion on neuroimaging
Major neuroimaging criteria: cystic lesions ± scolex, small enhancing lesions, multilobulated subarachnoid cysts, parenchymal calcifications
Major clinical/exposure criteria: positive EITB, cysticercosis outside CNS, household contact with T. solium
Treatment
Taeniasis
- Praziquantel 10 mg/kg single dose (drug of choice) - use with caution if comorbid cysticercosis suspected, as it can trigger CNS inflammation/seizures
- Niclosamide 2 g single dose - equally effective, safer in patients with occult cysticercosis
Neurocysticercosis - Principles
Treatment is never an emergency and must be staged:
- Stabilize first: antiseizure medications, manage raised ICP
- Antiparasitic drugs are contraindicated in patients with elevated ICP or purely calcified lesions
Anti-seizure therapy:
- Single enhancing lesions: may taper ASMs after 6 months if imaging normalizes
- Multiple parenchymal lesions: taper after 2 years if lesions resolve, no calcification, no breakthrough seizures
- Calcified lesions: higher risk of recurrent seizures, especially with perilesional edema
Hydrocephalus management:
- Ventricular cysts in lateral/3rd ventricle → neuroendoscopic removal (preferred)
- 4th ventricle → microdissection posterior approach or neuroendoscopy
- If complete removal impossible → ventriculoperitoneal (VP) shunting
Antiparasitic drugs:
- Albendazole 15 mg/kg/day for 8-28 days (preferred for parenchymal disease)
- Combination albendazole + praziquantel 50 mg/kg/day - more effective for >2 cystic lesions or subarachnoid disease
- Always co-administer glucocorticoids (dexamethasone 0.1-0.4 mg/kg/day or prednisone 60 mg/day) to limit inflammation from dying parasites
Special situations:
- Ocular cysticercosis: surgical management only (drugs risk irreversible inflammation)
- Subarachnoid/racemose NCC: prolonged antiparasitic + prolonged glucocorticoids + shunting for hydrocephalus; methotrexate or TNF inhibitors as steroid-sparing agents in refractory cases
Prevention and Control
- Taeniasis prevention: cook pork until interior is gray (56°C for 5 min) or freeze at -20°C for ≥7-10 days; meat inspection
- Cysticercosis prevention: handwashing, treated water, proper disposal of human feces; treat tapeworm carriers
- Programmatic control: mass chemotherapy in human and pig populations; porcine vaccine licensed in India (and a few other countries)
Key Distinguishing Points: T. solium vs T. saginata
| Feature | T. solium | T. saginata |
|---|---|---|
| Common name | Pork tapeworm | Beef tapeworm |
| Scolex | 4 suckers + rostellum with hooklets ("armed") | 4 suckers only ("unarmed") |
| Proglottid uterine branches | <13 | ≥14 |
| Intermediate host | Pig (and humans) | Cattle |
| Human can be intermediate host? | Yes → cysticercosis | No |
| Infection route (taeniasis) | Undercooked pork | Undercooked beef |
| Infection route (larval) | Ingestion of eggs (fecal-oral) | N/A |
| Clinical significance | High (NCC, epilepsy) | Lower (intestinal only) |
Sources: Medical Microbiology 9e; Harrison's Principles of Internal Medicine 22e (2025); Goldman-Cecil Medicine; Tietz Textbook of Laboratory Medicine 7e; Robbins & Cotran Pathologic Basis of Disease
Recent evidence: Recent systematic reviews (2025) focus on neurosurgical management of NCC (PMID 39982074) and neuroendoscopic management of intraventricular NCC (PMID 40381508), consistent with current textbook guidance favoring neuroendoscopy for ventricular cysts.
This is a shared conversation. Sign in to Orris to start your own chat.