
Screenshot_20260620-114532.png
Explain
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed for a comprehensive explanation. Here is the full answer:
PA 30.1 - Breast Pathology: Types, Etiology, Pathogenesis, Hormonal Dependency, and Benign Disease
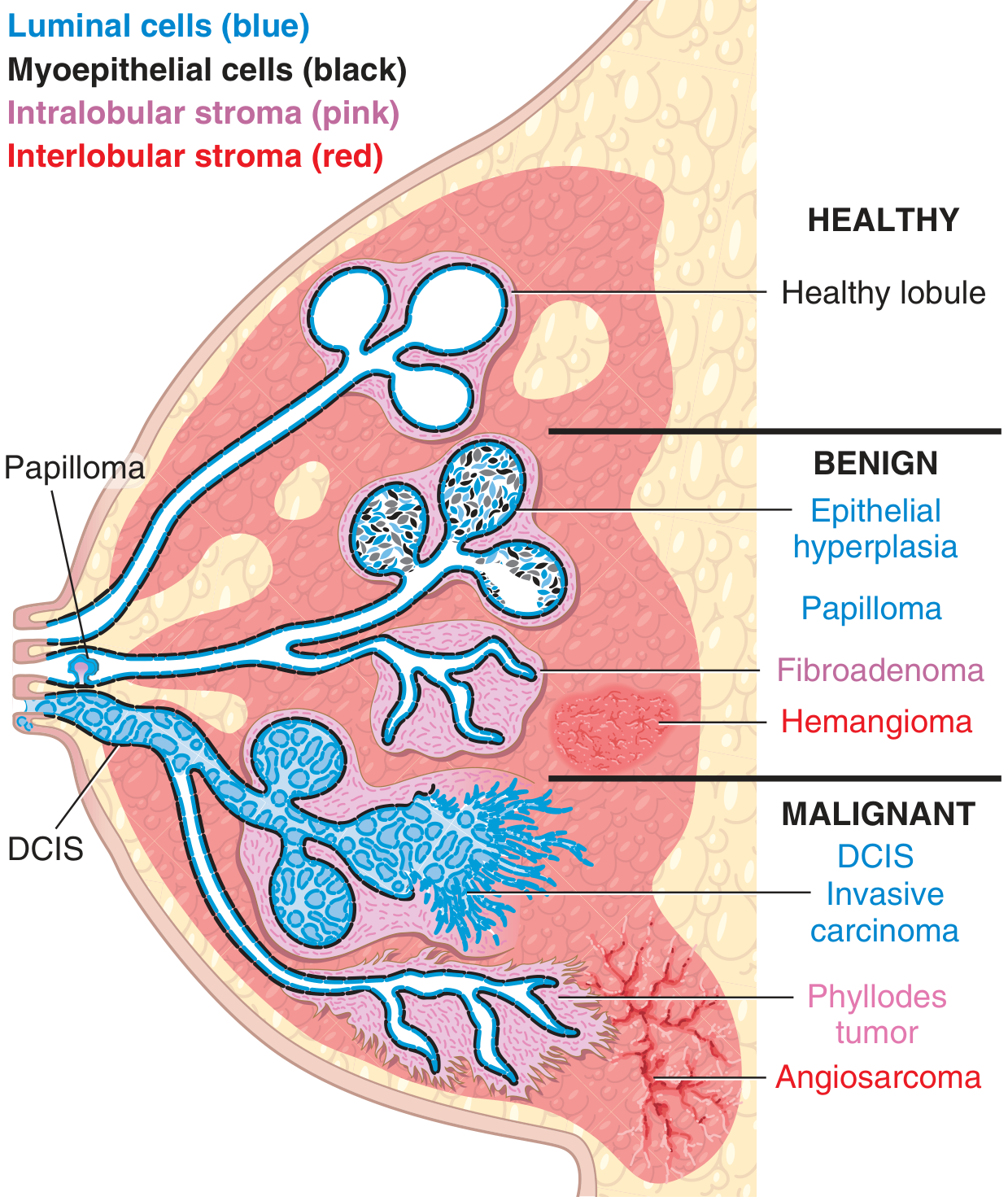
1. Anatomy & Functional Unit
The functional unit of the breast is the terminal duct lobular unit (TDLU). It contains:
- Luminal epithelial cells - produce milk during lactation
- Myoepithelial cells (basal layer) - contractile, aid milk ejection, support basement membrane
- Intralobular stroma (specialized connective tissue around lobules)
- Interlobular stroma (bulk of breast volume; increases at puberty, involutes with age)
Each of these compartments is a source of distinct benign and malignant disorders:
2. Hormonal Dependency of Breast Pathology
The breast is a dynamic, hormonally driven organ. Oestrogen and progesterone act as growth factors on both the epithelial and stromal cells of the TDLU, driving:
- Cyclical changes every menstrual cycle (proliferation in the follicular phase, secretory changes in the luteal phase)
- Development - lobular growth and branching from puberty through reproductive years
- Involution - regression of lobules after menopause (ages 35-55)
Imbalances in these hormones underlie most benign breast disease:
- Excess oestrogen relative to progesterone drives epithelial proliferation
- Progesterone deficiency contributes to cyst formation and mastalgia
- In males, gynecomastia results from an imbalance: too much oestrogen stimulation relative to androgen counteraction
Key hormone-sensitive conditions:
| Condition | Hormonal Link |
|---|---|
| Cyclical mastalgia | Oestrogen/progesterone imbalance |
| Fibrocystic changes | Cyclic oestrogen stimulation |
| Fibroadenoma | Oestrogen-driven intralobular stromal/epithelial growth |
| Breast carcinoma (ER+) | Oestrogen receptor-positive; responds to anti-oestrogens |
| Gynecomastia | Excess oestrogen, reduced androgen |
3. ANDI - The Framework for Benign Breast Disease
The modern concept for understanding benign breast disease is Aberrations of Normal Development and Involution (ANDI), developed by the Cardiff Breast Clinic. It recognizes that most benign disorders are minor aberrations of the normal physiological processes of:
- Lobule development (ages 15-25) → aberration = Fibroadenoma
- Cyclical hormonal changes (ages 15-50) → aberration = Cyclical mastalgia, nodularity, fibrocystic changes
- Involution (ages 35-55) → aberration = Cyst formation, sclerosing adenosis, duct ectasia
4. Classification of Breast Pathology
A. Inflammatory Processes
- Lactational mastitis/abscess - most common; caused by Staphylococcus aureus or streptococci during first month of breastfeeding; treated with antibiotics ± drainage
- Non-lactational abscess - rare; mixed anaerobic organisms
- Autoimmune/foreign body reactions - rare; always exclude inflammatory carcinoma
B. Benign Epithelial Lesions (Fibrocystic-type Changes)
Classified into 3 groups based on cancer risk:
1. Nonproliferative Changes (no increased cancer risk)
- Cysts - most common; lined by luminal cells with apocrine metaplasia; secretions can calcify
- Fibrosis - due to cyst rupture, spilling debris → chronic inflammation → fibrosis → palpable nodularity ("fibrocystic changes")
- Adenosis - increased number of acini per lobule; physiologic in pregnancy
- Characterized by a single layer of epithelial cells
2. Proliferative Lesions Without Atypia (1.5-2x increased cancer risk)
- Epithelial hyperplasia - >2 cell layers in ducts/acini
- Sclerosing adenosis - distorted, enlarged lobules with proliferating acini
- Radial scar / complex sclerosing lesion - stellate lesion that mimics carcinoma on imaging
- Intraductal papilloma - fibrovascular core + papillary epithelial projections; most common cause of bloody nipple discharge; 3 types:
- Solitary papilloma (RR for cancer: 1.5-2)
- Papillomatosis - 5+ papillomas (RR: 3)
- Juvenile papillomatosis ("Swiss cheese disease") - affects young women
3. Proliferative Disease With Atypia (4-5x increased cancer risk)
- Atypical Ductal Hyperplasia (ADH) - closely resembles DCIS but more limited; uniform cells with sharply marginated spaces
- Atypical Lobular Hyperplasia (ALH) - resembles LCIS but limited; monomorphic cells with bland, round nuclei
- These are precursor lesions and are important to identify on biopsy
C. Stromal Neoplasms (from Intralobular Stroma)
| Tumor | Features |
|---|---|
| Fibroadenoma | Benign; most common solid breast lump in young women; both neoplastic stroma + reactive epithelium; circumscribed; driven by oestrogen (enlarges in pregnancy) |
| Phyllodes tumor | Stromal cells outgrow epithelium; "leaflike" growth; most benign but can recur; rarely malignant |
From interlobular stroma: lipomas, angiosarcomas (same tumors as elsewhere in connective tissue)
5. Clinical Presentations of Breast Disease
| Symptom | Most Likely Cause |
|---|---|
| Mastalgia (cyclical) | Hormonal (oestrogen/progesterone imbalance); most common breast complaint (50-70% of clinic attendees) |
| Mastalgia (non-cyclical) | Cyst rupture, fat necrosis, musculoskeletal |
| Diffuse nodularity | Physiologic or fibrocystic changes; bilateral, upper outer quadrant |
| Palpable discrete lump | Fibroadenoma (young), cyst (middle-aged), carcinoma (older) |
| Nipple discharge | Papilloma (most common benign cause); bloody + unilateral = suspicious for malignancy |
| Inflammatory signs | Lactational abscess (most common); always exclude inflammatory carcinoma |
| Gynecomastia (males) | Oestrogen/androgen imbalance |
-
90% of breast lesions are benign
- Likelihood of malignancy increases with age
6. Mastalgia - Detail
- Cyclical mastalgia: Starts ~day 14, worsens until day 27-28, relieved with onset of menses; usually bilateral; related to oestrogen excess/progesterone deficiency
- Non-cyclical mastalgia: No relation to menstrual cycle; usually unilateral; causes include cyst, fat necrosis, costochondritis
Treatment ladder (Bailey & Love's):
- Reassure (exclude cancer first); adequate bra support
- Flaxseed / evening primrose oil (omega-3/GLA)
- Topical NSAIDs (diclofenac, piroxicam)
- Tamoxifen 10 mg/day, Danazol, or Ormeloxifene for 3-6 months
- LHRH agonist for refractory cases
Summary Table: ANDI Classification
| Phase | Normal | Aberration | Disease |
|---|---|---|---|
| Development (15-25 yr) | Lobule formation; fibroadenoma stroma | Fibroadenoma | Giant fibroadenoma |
| Cyclical change (15-50 yr) | Cyclical breast changes | Cyclical mastalgia, nodularity | Incapacitating mastalgia |
| Involution (35-55 yr) | Lobular involution; duct widening | Cysts, sclerosing adenosis, duct ectasia | Symptomatic cysts, periductal mastitis |
Sources: Robbins & Kumar Basic Pathology, Bailey and Love's Short Practice of Surgery 28th ed.

Screenshot_20260621-105240.png
Explain
Your credits are exhausted. You can purchase a top-up or subscribe to a plan to continue using Orris. If you're already subscribed, your daily credits will reset tomorrow.
This is a shared conversation. Sign in to Orris to start your own chat.