Girl 26 years old , has hirsutism since childhood , a couple months ago hair started getting thick below belly button line , she light has hair over breasts and all over body , she noticed a thick single hair strand on her chin and another one on her cheek , suffers from chronic acne , acne disappeared with isotretinoin but appeared again after one face laser session and persisted What could be wrong with her?
Reading File
Finding Sources
Finding Sources
Searching PubMed
hirsutism acne androgen excess women differential diagnosis
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Searching PubMed
PCOS hirsutism acne diagnosis
Reading File
I now have everything needed for a comprehensive answer. Let me synthesize.
Clinical Analysis: 26-year-old with Lifelong Hirsutism + Acne
This presentation is a classic picture of hyperandrogenism — excess androgen action on the pilosebaceous unit. The clues are:
- Hirsutism since childhood (long-standing androgen excess, not acute)
- Terminal hair in androgen-dependent zones: below umbilicus, breasts, chin, cheek
- Chronic, treatment-resistant/recurrent acne
- Generalized body hair
The combination points to a functional androgen excess disorder, with the following differential:
Most Likely Diagnoses
1. 🥇 Polycystic Ovary Syndrome (PCOS) — Most Common
PCOS is the single most common cause of androgen excess in reproductive-age women, accounting for 70–80% of hirsutism cases. Diagnosis requires 2 of 3 Rotterdam criteria:
- Clinical or biochemical hyperandrogenism ✅ (hirsutism, acne)
- Ovulatory dysfunction (menstrual irregularity — not mentioned here, but may be subtle)
- Polycystic ovarian morphology on ultrasound
Key features matching this patient:
- Hirsutism in androgen-dependent areas (chin, cheek, lower abdomen, chest)
- Chronic acne, refractory or recurrent
- Onset around/after puberty
Even with regular periods, PCOS can be present (phenotype D — hyperandrogenism + polycystic ovaries without clear anovulation). — Textbook of Family Medicine 9e; Harrison's 22E
2. 🥈 Nonclassical Congenital Adrenal Hyperplasia (NC-CAH)
This is the second most common cause and is critically important here because:
- Hirsutism since childhood — NC-CAH (most often 21-hydroxylase deficiency) presents at or just after puberty, sometimes even earlier
- The enzyme defect leads to inadequate cortisol synthesis → excess ACTH → adrenal hyperplasia → excess androgens (DHEA-S, androstenedione)
- Clinically identical to PCOS: hirsutism, acne, menstrual irregularity, anovulation
"Nonclassic CAH is most commonly due to 21-hydroxylase deficiency... The adrenal gland cannot secrete glucocorticoids efficiently, resulting in diminished negative feedback inhibition of ACTH, leading to compensatory adrenal hyperplasia and the accumulation of androgen precursors." — Harrison's 22E
Key distinguishing test: Early-morning 17-hydroxyprogesterone (17-OHP) — elevated basal or ACTH-stimulated levels confirm 21-hydroxylase deficiency. This diagnosis is often missed. The childhood onset in this case makes it especially worth pursuing.
3. SAHA Syndrome
The textbooks specifically recognize SAHA — Seborrhea, Acne, Hirsutism, Alopecia — as a distinct clinical entity:
"Some women have acne and androgenetic alopecia as well as hirsutism, in association with slight increases in serum androgen levels (e.g. testosterone and DHEAS)." — Dermatology 5e
This patient has hirsutism + acne, and if seborrhea or androgenetic alopecia is present, SAHA applies. This may overlap with PCOS or idiopathic hyperandrogenism.
4. Idiopathic Hirsutism (IH)
If androgens turn out to be normal or only mildly elevated and menstrual cycles are regular, idiopathic hirsutism is possible — driven by increased 5α-reductase activity and end-organ (hair follicle) sensitivity to androgens, not elevated circulating levels.
However, the presence of acne (sebaceous gland involvement) makes pure idiopathic hirsutism less likely — IH usually presents with hair growth alone without acne.
5. Less Likely, But Must Exclude
| Condition | Red flags present? |
|---|---|
| Androgen-secreting ovarian/adrenal tumor | Rapid progression, virilization (voice deepening, clitoromegaly) — NOT described here. Slow onset makes tumor unlikely. |
| Cushing syndrome | No centripetal obesity, striae, proximal weakness mentioned |
| Hyperprolactinemia | No galactorrhea, amenorrhea, headache mentioned |
| Hyperthecosis | Severe insulin resistance; can mimic PCOS but more extreme |
| HAIR-AN syndrome | Hyperandrogenism + Insulin Resistance + Acanthosis Nigricans |
The Acne Behavior: An Important Clue
The fact that isotretinoin cleared the acne but one laser session triggered a relapse that persisted is notable. Laser (if targeting the face) can cause a temporary inflammatory response, but persistent acne relapse after a single session suggests the underlying hormonal drive was never treated — isotretinoin suppressed sebum production temporarily without addressing the root androgen excess. This is a hallmark pattern of hormonally-driven acne in hyperandrogenic states.
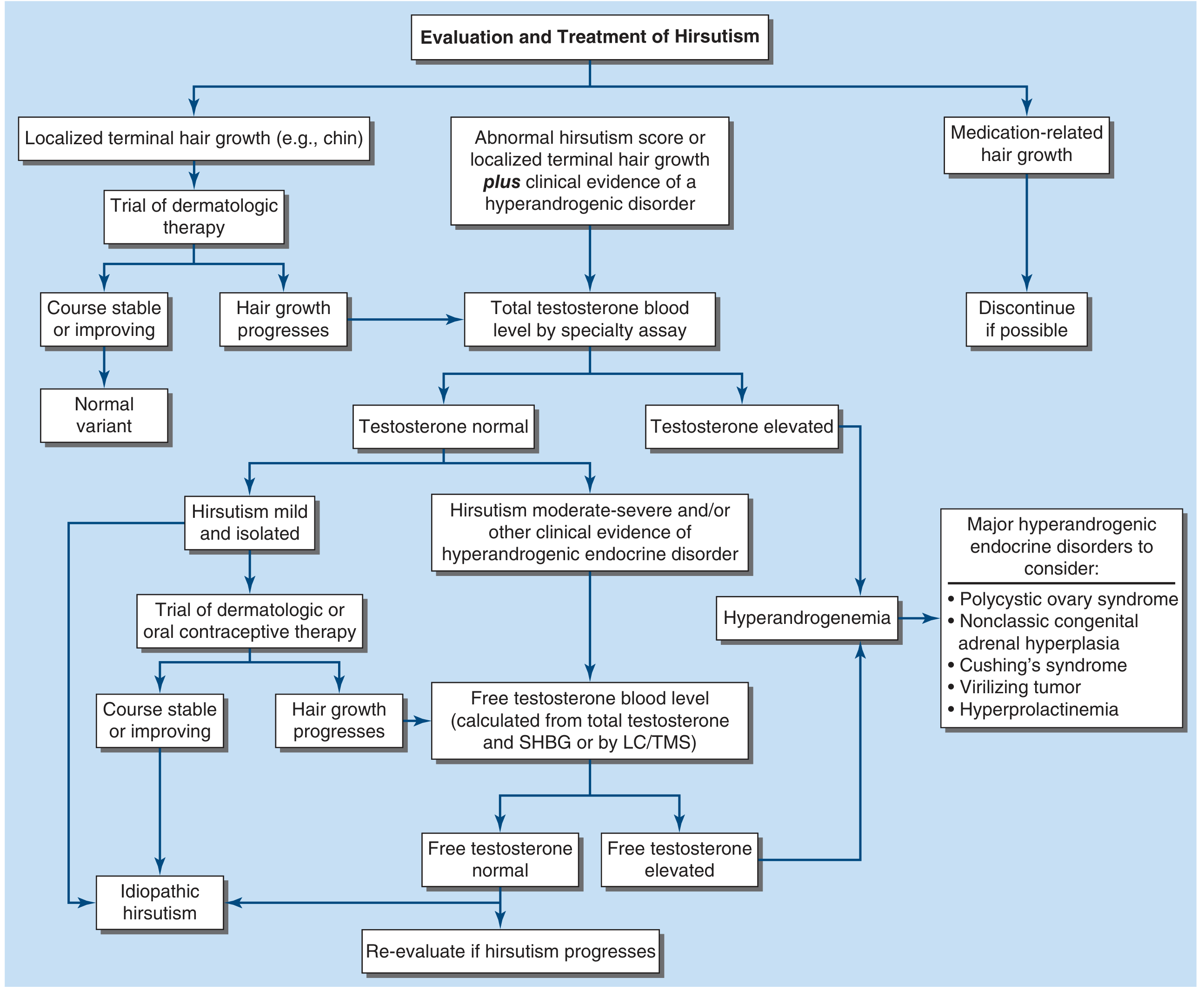
Recommended Workup
Based on Harrison's 22E and Fitzpatrick's Dermatology diagnostic algorithm:
First line:
- Total testosterone (free/bioavailable preferred): >7 nmol/L suggestive of tumor, >12 nmol/L highly suggestive
- DHEAS: elevated → adrenal source; markedly elevated (>18.5 μmol/L) → adrenal tumor
- Early morning 17-OHP (ideally follicular phase): to screen for NC-CAH
- LH, FSH (LH:FSH ratio >2 suggests PCOS, though not diagnostic alone)
- Fasting insulin, glucose, HOMA-IR: insulin resistance is common in PCOS
- Prolactin, TSH: to exclude hyperprolactinemia/thyroid disease
- Pelvic ultrasound: assess for ovarian morphology
Summary
| Priority | Diagnosis | Key Feature Supporting It |
|---|---|---|
| 1st | PCOS | Most common cause, hyperandrogenism + acne + female of reproductive age |
| 2nd | Nonclassical CAH | Childhood onset, adrenal androgen excess, confirmed by 17-OHP |
| 3rd | SAHA syndrome | Seborrhea + Acne + Hirsutism |
| 4th | Idiopathic hirsutism | If labs normal, but acne makes this less likely |
The hormonal basis explains why acne keeps returning despite isotretinoin — the androgen stimulus is never removed. Treatment must target the underlying cause (OCP with anti-androgenic progestin, spironolactone, or low-dose glucocorticoid in CAH) rather than just the skin manifestation.
Sources: Harrison's Principles of Internal Medicine 22E; Fitzpatrick's Dermatology Vol. 1–2; Textbook of Family Medicine 9e; Dermatology 2-Volume Set 5e; Berek & Novak's Gynecology
This is a shared conversation. Sign in to Orris to start your own chat.