physiology, biochem, pathology, micro, clinical presentation, medine and pharma related to abdomen, hepatobiliary for surgery
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
Breast
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive content from all major sources. Let me compile the complete surgical breast review.
Breast - Complete Surgical Review
Physiology | Biochemistry | Pathology | Microbiology | Clinical Presentation | Medicine | Pharmacology
1. ANATOMY & PHYSIOLOGY
Gross Anatomy
The breasts lie in the pectoral region of the anterior thoracic wall. Vascular supply comes from:
- Medial: Perforating branches of the internal thoracic artery (2nd-4th intercostal spaces)
- Lateral: Branches from the axillary artery (lateral thoracic, thoracoacromial)
- Sensory innervation: Lateral and anterior branches of the 4th-6th intercostal nerves
Lymphatic Drainage (surgically critical)
- Lateral breast → axillary nodes (75% of total drainage; Level I > II > III)
- Medial breast → parasternal (internal mammary) nodes
- Axillary levels: Level I (lateral to pectoralis minor), Level II (behind), Level III (medial/infraclavicular)
(Gray's Anatomy for Students, p.168)
Microscopic Structure
The functional unit is the lobule, lined by:
- Inner luminal epithelial cells - produce milk during lactation
- Basal myoepithelial cells - contractile function, milk ejection, support of basement membrane
The ducts conduct milk to the nipple. Breast size is determined primarily by interlobular stroma, which increases at puberty and involutes with age. Each component is a source of distinct lesions:
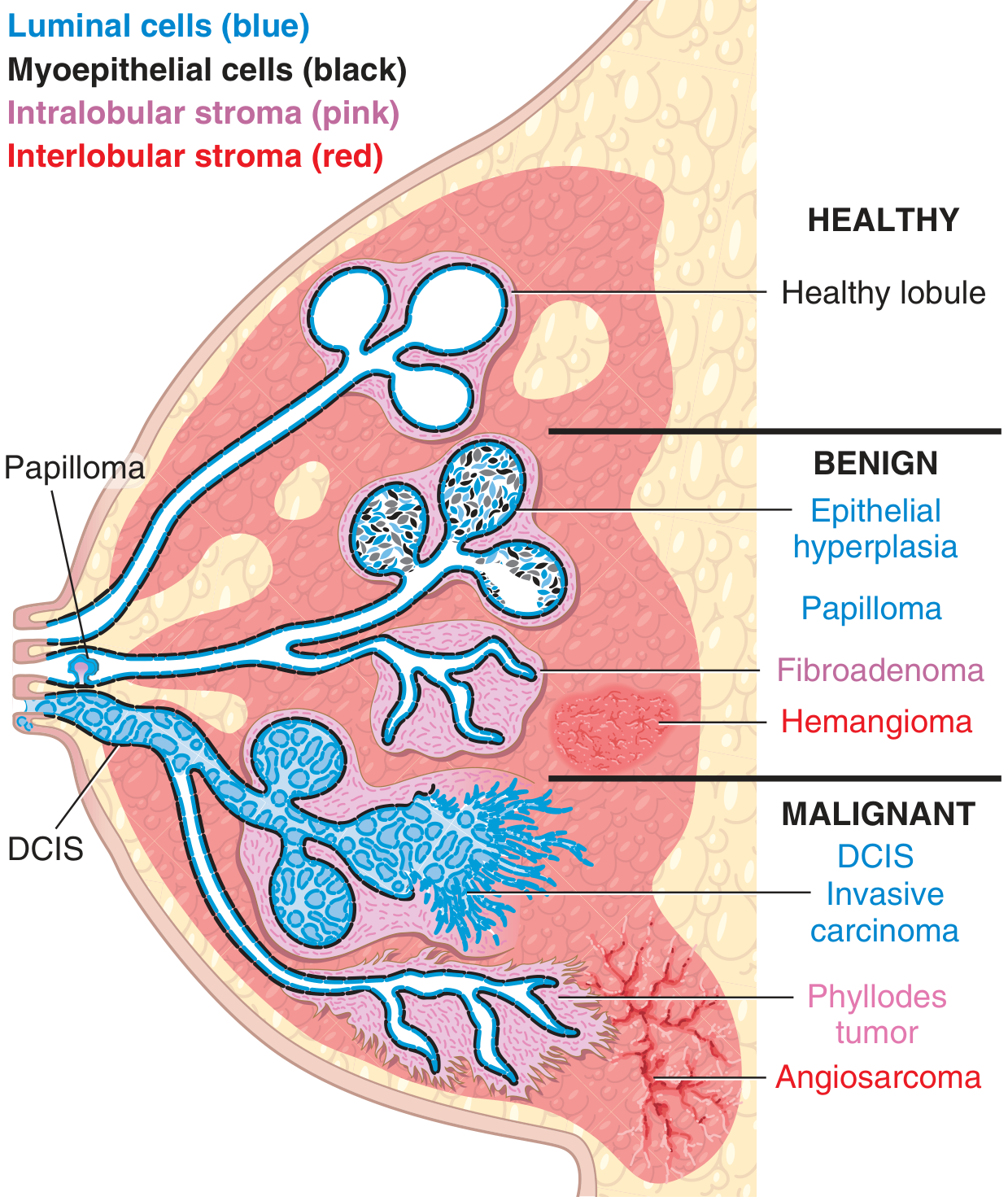
(Robbins & Kumar Basic Pathology, p.705)
Physiological Breast Development
- Puberty: estrogen stimulates ductal growth; progesterone drives lobular development
- Pregnancy: prolactin + human placental lactogen drive alveolar differentiation
- Lactation: prolactin maintains milk production; oxytocin causes myoepithelial contraction, forcing milk from alveolar channels into collecting sinuses (milk ejection reflex - suckling stimulus)
- Menopause: interlobular stroma involutes; glandular tissue regresses
(Goodman & Gilman's, p.956)
2. BIOCHEMISTRY
Estrogen Receptor Signaling
- Estrogen binds ERα/ERβ → receptor dimerizes → binds estrogen response elements (ERE) on DNA → transcription of proliferative genes (cyclin D1, c-Myc, VEGF)
- Progesterone receptor (PR) expression is estrogen-dependent (positive PR indicates functional ER pathway)
BRCA1 and BRCA2 Genes
- BRCA1 - chromosome 17q; encodes a DNA damage sensor/repair protein; involved in homologous recombination repair of double-strand breaks
- BRCA2 - chromosome 13q; encodes a DNA repair protein; interacts with RAD51
- 5-10% of all breast cancers are due to inherited BRCA1/2 mutations
- BRCA1 mutation: lifetime breast cancer risk ~65-80%; ovarian cancer risk ~39-46%
- BRCA2 mutation: lifetime breast cancer risk ~45-85%; also increased pancreatic, prostate, and male breast cancer risk
- Male breast cancer is most commonly attributed to BRCA2
(Basic Medical Biochemistry 6e, p.3)
HER2/neu (ErbB2)
- Proto-oncogene on chromosome 17q; encodes a receptor tyrosine kinase (transmembrane)
- Amplified/overexpressed in 15-20% of breast cancers
- HER2 has no known ligand - activates by heterodimerization with other HER family members
- Downstream: RAS-MAPK (proliferation) and PI3K-AKT-mTOR (survival) pathways
Key Molecular Pathways
- PI3K/AKT/mTOR: activated by PIK3CA mutations (~40% of ER+ tumors)
- CDK4/6 - Cyclin D1 - Rb axis: drives cell cycle entry (G1→S); targeted therapeutically
- TP53 mutations: common in triple-negative and HER2+ subtypes
- E-cadherin loss: hallmark of lobular carcinoma (loss of cellular cohesion → "single file" invasion)
3. PATHOLOGY
Benign Conditions
Fibrocystic Change (most common benign lesion)
- Non-proliferative: cysts, mild hyperplasia - no increased cancer risk
- Proliferative without atypia (e.g., usual ductal hyperplasia, sclerosing adenosis) - 1.5-2x increased risk
- Proliferative with atypia (atypical ductal hyperplasia [ADH], atypical lobular hyperplasia [ALH]) - 4-5x increased risk; if positive family history, risk up to 10x
Fibroadenoma
- Most common solid benign tumor; young women (20s-30s)
- Intralobular stroma derived - neoplastic stromal cells + reactive epithelial proliferation
- Histology: circumscribed, low cellularity; fibroblasts push/distort epithelium into elongated slitlike structures
- Management: observation if typical on imaging; excision if enlarging or atypical
Phyllodes Tumor
- Also intralobular stroma derived (spectrum with fibroadenoma)
- Stromal cells outgrow epithelium → "leaf-like" (phyllodes) growth pattern with bulbous nodules of stroma covered by epithelium
- Low/borderline/high grade; high grade may be sarcomatous
- Treatment: wide local excision (WLE) with clear margins - no effective chemotherapy
Intraductal Papilloma
- Most common cause of unilateral, spontaneous, bloody/serous nipple discharge in premenopausal women
- Grows in large ducts below nipple
- Benign but associated with slightly increased cancer risk
Lactational (Puerperal) Abscess
- Peak: first month of breastfeeding
- Organism: Staphylococcus aureus (most common), rarely streptococci
- Treatment: antibiotics (dicloxacillin/flucloxacillin; MRSA → vancomycin or TMP-SMX) + continued milk expression; I&D if fluctuant
Non-lactational (Periductal) Mastitis/Abscess
- Mixed anaerobic organisms
- Associated with smoking, duct ectasia, periareolar location
- Treatment: antibiotics (co-amoxiclav covers anaerobes); may need I&D and fistula excision
Premalignant and In Situ Lesions
DCIS (Ductal Carcinoma In Situ)
- Malignant cells confined to ducts/lobules, basement membrane intact
- Most detected by mammography (calcifications - often linear/branching in comedo type)
- Subtypes: comedo (high grade, central necrosis/calcifications), cribriform, micropapillary, solid
- Paget disease of the nipple = DCIS extending up lactiferous ducts into nipple skin → unilateral crusting/oozing exudate over nipple/areola
- Treatment: surgical excision ± radiation → >95% survival at 20 years
- High-grade or extensive DCIS: higher risk of progression to invasive carcinoma
LCIS (Lobular Carcinoma In Situ)
- Bland, monomorphic cells expanding lobules; rarely produces calcifications
- Not truly a precursor lesion but a bilateral risk marker (~1% per year progression to invasive carcinoma in either breast)
- Treatment: surveillance vs. risk reduction with tamoxifen/raloxifene
- E-cadherin negative (unlike DCIS which is E-cadherin positive)
(Robbins & Kumar Basic Pathology, p.712-713)
Invasive Carcinoma - Types
Most common location: upper outer quadrant (50%), then central (20%)
| Type | Frequency | Key Features |
|---|---|---|
| Invasive ductal carcinoma (IDC), No Special Type (NST) | 70-80% | Variable histology; desmoplastic stroma → hard palpable mass; spiculated on mammography |
| Invasive lobular carcinoma (ILC) | 10-15% | Single-file invasion; E-cadherin negative; often bilateral; subtle on mammography |
| Medullary carcinoma | ~5% | Sheets of anaplastic cells + prominent lymphocytic infiltrate; usually triple-negative; >50% are BRCA1-associated; circumscribed on imaging (can mimic benign) |
| Mucinous (colloid) carcinoma | <5% | Tumor cells floating in mucin; soft, well-circumscribed; better prognosis |
| Tubular carcinoma | <2% | Well-differentiated tubules; excellent prognosis |
| Inflammatory breast carcinoma | 1-3% | Tumor emboli in dermal lymphatics → peau d'orange, erythema, warmth; no discrete mass; clinical diagnosis |
(Robbins & Kumar Basic Pathology, p.713-714)
Molecular Subtypes (Intrinsic Subtypes)
| Subtype | Receptor Status | Frequency | Characteristics |
|---|---|---|---|
| Luminal A | ER+/PR+, HER2-, low Ki67 | ~40% | Best prognosis; endocrine therapy usually sufficient |
| Luminal B | ER+/PR+/-, HER2-, high Ki67 OR HER2+ | ~20% | Intermediate prognosis; may need chemotherapy |
| HER2-enriched | ER-, PR-, HER2+ | ~15% | Aggressive; targeted anti-HER2 therapy |
| Triple-Negative (TNBC) | ER-, PR-, HER2- | ~15% | Most aggressive; BRCA1-associated; basal-like phenotype; chemotherapy backbone |
Grading (Nottingham/Elston-Ellis Grade)
Three components, each scored 1-3:
- Tubule formation
- Nuclear pleomorphism
- Mitotic count
Total 3-9: Grade 1 (3-5) = well differentiated; Grade 2 (6-7) = moderately differentiated; Grade 3 (8-9) = poorly differentiated
Staging (TNM - AJCC 8th Edition, now includes biomarkers)
- T: T1 ≤2cm; T2 2-5cm; T3 >5cm; T4 chest wall/skin involvement (T4d = inflammatory)
- N: N0 no nodes; N1 1-3 axillary nodes; N2 4-9 nodes; N3 ≥10 nodes or internal mammary
- M: M0 no metastasis; M1 distant metastasis (bone most common, then lung, liver, brain)
4. MICROBIOLOGY
Breast Infections
| Condition | Organism | Setting | Treatment |
|---|---|---|---|
| Lactational mastitis/abscess | S. aureus (MSSA >> MRSA), Group A/B Strep | Breastfeeding, 1st month | Dicloxacillin/clindamycin; MRSA: TMP-SMX/vancomycin; continue breastfeeding; I&D if abscess |
| Periductal mastitis | Mixed anaerobes (Bacteroides, Peptostreptococcus), coliforms | Non-lactating, smokers | Co-amoxiclav (covers anaerobes); smoking cessation; excision of fistula |
| Tuberculosis mastitis | Mycobacterium tuberculosis | Rare; endemic areas | Anti-TB therapy; excision not required |
| Hidradenitis suppurativa | Polymicrobial | Apocrine glands, axilla/breast fold | Antibiotics + surgical excision of affected skin |
Microbiology note on inflammatory breast carcinoma: This is NOT infectious - it mimics cellulitis but is caused by tumor emboli in dermal lymphatics. Must be distinguished from true mastitis. Biopsy confirms diagnosis.
5. CLINICAL PRESENTATION & EXAMINATION
Symptoms and Their Significance
| Symptom | Most Common Cause | Red Flags for Malignancy |
|---|---|---|
| Pain (mastalgia) | Cyclic (hormonal), fibrocystic | Localized fixed pain, in ~5% underlies cancer |
| Nipple discharge | Fibrocystic, lactation | Unilateral, spontaneous, bloody = malignancy until proven otherwise |
| Palpable mass | Fibroadenoma (young), cyst (middle-aged) | Hard, irregular, fixed, non-tender; in UOQ |
| Skin changes | Infection | Peau d'orange, skin tethering, nipple retraction, ulceration |
| Nipple changes | Eczema | Paget disease: unilateral, crusting, not responding to topical steroids |
Key exam features of malignant mass: hard, irregular, fixed (tethered) to skin or chest wall, non-tender, associated lymphadenopathy
The Triple Assessment
- Clinical examination
- Imaging - Mammography (>35y) or Ultrasound (<35y or dense breasts)
- Tissue biopsy - Core needle biopsy (preferred over FNAC for hormone receptor/HER2 testing)
All three must agree for benign diagnosis (concordance). Any suspicious finding mandates biopsy.
Screening
- Mammography: standard of care; annual from age 40 (ACS); biennial 50-74 (USPSTF)
- MRI: indicated for BRCA carriers, high-risk women (>20% lifetime risk), implants
- BRCA1/2 carriers: MRI + mammogram annually from age 25-30
6. SURGICAL MANAGEMENT
Surgical Options for Breast Cancer
| Procedure | Definition | Indications |
|---|---|---|
| Lumpectomy (BCS - Breast-Conserving Surgery) | Excision of tumor with clear margins (>2mm) | Stage I-II; must be followed by whole-breast radiation; equivalent OS to mastectomy (landmark NSABP B-06, Milan trials) |
| Simple (total) mastectomy | Removal of entire breast (skin, nipple, areola) without axillary dissection | DCIS; prophylactic; followed by SLNB if invasive cancer possible |
| Modified radical mastectomy (MRM) | Mastectomy + Level I/II axillary clearance; pectoralis major preserved | Historically standard for invasive cancer; now less common with BCS availability |
| Skin-sparing mastectomy | Mastectomy preserving breast skin envelope | For immediate reconstruction |
| Nipple-sparing mastectomy (NSM) | Preserves skin, nipple, and areola | Prophylactic; selected invasive cancers; facilitates direct-to-implant reconstruction |
| Radical mastectomy (Halsted) | En bloc removal of breast + pectoralis muscles + axillary nodes | Now rarely indicated; reserved for T4 disease with chest wall invasion |
Axillary Management
Sentinel Lymph Node Biopsy (SLNB) - Standard of care for clinically node-negative breast cancer
- Developed in 1994; radiotracer (Tc-99m sulfur colloid) ± blue dye injected peritumorally
- First draining node(s) removed and examined (intraoperative frozen section or permanent)
- If sentinel node negative → no further axillary dissection required (NSABP B-32 trial)
- ACOSOG Z0011 trial: even with 1-2 positive sentinel nodes in patients undergoing BCS + whole-breast radiation, completion axillary dissection may be omitted without compromising OS
Axillary Lymph Node Dissection (ALND) - Level I-III clearance
- Indicated for: clinically positive nodes (confirmed by biopsy), >2 positive sentinel nodes in certain settings, inflammatory breast cancer
- Complications: lymphedema (most feared; 15-25%), shoulder stiffness, nerve injury (long thoracic nerve → winged scapula; thoracodorsal nerve → latissimus weakness)
(Sabiston Textbook of Surgery, p.1425; Current Surgical Therapy 14e)
Breast Reconstruction
Timing:
- Immediate: at time of mastectomy; psychologically beneficial; better aesthetics; contraindicated if inflammatory breast cancer or when post-mastectomy radiation is planned (risk of implant loss/fibrosis)
- Delayed: after mastectomy on separate date; mandated when radiation or chemotherapy needed first; also for high BMI, poorly controlled diabetes, active smokers
Types:
-
Implant-based (most common today):
- Two-stage: tissue expander placed at mastectomy → gradual expansion → permanent implant exchange (6-12 weeks after expansion complete; delayed further if radiation needed)
- Direct-to-implant (one-stage): NSM candidates with well-perfused skin flap
- Implants can be submuscular, subpectoral, or prepectoral (with ADM - acellular dermal matrix)
- Complication: Breast Implant-Associated Anaplastic Large Cell Lymphoma (BIA-ALCL) - rare T-cell lymphoma linked to textured implants
-
Autologous flap reconstruction:
- TRAM flap (transverse rectus abdominis myocutaneous): pedicled or free; uses lower abdominal skin/fat; associated with abdominal wall weakness
- DIEP flap (deep inferior epigastric perforator): free flap; spares rectus muscle; gold standard for autologous reconstruction
- Latissimus dorsi flap: pedicled; often combined with implant; suitable after chest wall radiation
- SGAP/IGAP flap: gluteal perforator flaps for patients without suitable abdominal tissue
Women's Health and Cancer Rights Act (1998): mandates insurance coverage for breast reconstruction including contralateral symmetry procedures.
(Sabiston Textbook of Surgery, p.1425)
7. MEDICINE (SYSTEMIC THERAPY & ONCOLOGY)
Adjuvant Chemotherapy
- Used for higher-risk tumors: node-positive, large tumors, triple-negative, HER2+
- Standard regimens: AC-T (doxorubicin/cyclophosphamide → paclitaxel/docetaxel)
- TNBC: AC-T ± carboplatin; consider capecitabine adjuvant after neoadjuvant if residual disease
- Neoadjuvant (pre-operative): to downstage tumors for BCS; pathological complete response (pCR) is a surrogate for improved survival
Prognostic Genomic Tests
- Oncotype DX (21-gene recurrence score): most validated; ER+/HER2-/node-negative (or limited node-positive); score 0-100; guides chemotherapy decisions (TAILORx trial: RS 11-25 → endocrine therapy alone adequate)
- MammaPrint (70-gene signature): FDA-approved for predicting distant recurrence
- Prosigna (PAM50): intrinsic subtype classification + risk of recurrence score
8. PHARMACOLOGY
A. Endocrine Therapy (for ER+ tumors)
Selective Estrogen Receptor Modulators (SERMs)
Tamoxifen
- Mechanism: competitive partial antagonist at ER in breast; agonist at uterus and bone
- Reduces breast cancer risk by 38% in high-risk women (chemoprevention - multiple trials including NSABP P-1)
- Adjuvant use: 5-10 years (extended therapy with 10 years shows additional benefit in premenopausal)
- Used in pre- and postmenopausal women
- Side effects: hot flashes, VTE (2-3x risk), endometrial cancer (2-3x risk - agonist effect on uterus), cataracts
- Metabolized by CYP2D6 to endoxifen (active metabolite); CYP2D6 inhibitors (fluoxetine, paroxetine) reduce efficacy
Raloxifene - Breast agonist antagonist; used for postmenopausal women; no endometrial stimulation; less VTE than tamoxifen; approved for chemoprevention (STAR trial: non-inferior to tamoxifen for invasive breast cancer risk reduction)
Selective Estrogen Receptor Degraders (SERDs)
Fulvestrant - Pure ER antagonist + downregulates/degrades ER; no agonist activity; IM injection monthly; used in metastatic ER+ disease
Elacestrant - Oral SERD; approved for ER+/HER2- tumors with ESR1 mutation (mechanism of AI resistance)
Aromatase Inhibitors (AIs) - Postmenopausal women only (or premenopausal + ovarian function suppression)
| Drug | Type | Key Facts |
|---|---|---|
| Anastrozole (Arimidex) | Type 2 non-steroidal, reversible | 1 mg/day oral; superior to tamoxifen in postmenopausal ER+ (ATAC trial) |
| Letrozole (Femara) | Type 2 non-steroidal, reversible | 2.5 mg/day oral; extended adjuvant use post-tamoxifen (MA.17 trial) |
| Exemestane (Aromasin) | Type 1 steroidal, irreversible | 25 mg/day oral; active metabolite of androstenedione |
- Mechanism: inhibit peripheral aromatase (CYP19A1) → block conversion of androgens (androstenedione) to estrogens (estrone) - the main source of estrogen in postmenopausal women
- Side effects: hot flashes, arthralgias/myalgias, vaginal dryness, osteoporosis/fractures (use bisphosphonate co-prescription)
- No increased endometrial cancer or VTE risk (unlike tamoxifen)
- SOFT/TEXT trials: OFS + exemestane superior to tamoxifen in high-risk premenopausal patients
(Current Surgical Therapy 14e, p.771; Goodman & Gilman's; Katzung 16e)
B. CDK4/6 Inhibitors (ER+/HER2- metastatic disease; expanding to adjuvant)
- Palbociclib, Ribociclib, Abemaciclib - inhibit CDK4 and CDK6 → arrest cell cycle at G1
- Combined with letrozole or fulvestrant; significantly improve PFS (PALOMA, MONALEESA, MONARCH trials)
- Abemaciclib: also approved adjuvant for high-risk ER+/HER2- early breast cancer (monarchE trial)
- Key side effects: neutropenia (palbociclib, ribociclib), diarrhea (abemaciclib), QTc prolongation (ribociclib)
C. Anti-HER2 Therapies
| Drug | Class | Mechanism | Key Use |
|---|---|---|---|
| Trastuzumab (Herceptin) | mAb (HER2 domain IV) | Binds HER2 → ADCC + inhibits downstream signaling | HER2+ early and metastatic; adjuvant (1 year post-surgery + chemo) |
| Pertuzumab (Perjeta) | mAb (HER2 domain II) | Blocks HER2-HER3 heterodimerization | Combined with trastuzumab + docetaxel for neoadjuvant/metastatic HER2+ (CLEOPATRA trial) |
| Lapatinib | TKI (HER1+HER2) | Dual tyrosine kinase inhibitor; small molecule, crosses BBB | HER2+ metastatic; CNS metastases |
| Neratinib | Irreversible pan-HER TKI | Covalently binds HER1/2/4 | Extended adjuvant after trastuzumab |
| Tucatinib | Selective HER2 TKI | Crosses BBB | Metastatic HER2+, brain metastases (HER2CLIMB trial) |
| T-DM1 (ado-trastuzumab emtansine) | ADC (trastuzumab + DM1) | HER2-targeted delivery of cytotoxic | Residual disease after neoadjuvant (KATHERINE trial) |
| T-DXd (trastuzumab deruxtecan) | ADC (trastuzumab + topoisomerase I inhibitor) | HER2-targeted + bystander effect | HER2+ metastatic (post T-DM1); also HER2-low (DESTINY-Breast04) |
Preferred 1st-line metastatic HER2+: taxane + pertuzumab + trastuzumab
- Trastuzumab binds domain IV of HER2 extracellular domain; mediates ADCC via NK cells (Current Surgical Therapy 14e, p.1413; Goldman-Cecil Medicine)
D. PARP Inhibitors (for germline BRCA1/2-mutated tumors)
- Olaparib, Talazoparib - inhibit PARP enzyme → prevent single-strand break repair → replication fork collapse → synthetic lethality in BRCA-deficient cells (defective homologous recombination)
- Olaparib: approved for gBRCA1/2+ early breast cancer (adjuvant, OlympiA trial) and metastatic HER2-
- Used in HER2- (TNBC and ER+) with gBRCA1/2 mutations
E. Immunotherapy (TNBC)
- Pembrolizumab (anti-PD-1): approved with chemotherapy for high-risk early TNBC (KEYNOTE-522) and PD-L1+ metastatic TNBC (KEYNOTE-355)
- Atezolizumab (anti-PD-L1): previously approved for PD-L1+ metastatic TNBC; now primarily replaced by pembrolizumab
F. Antibody-Drug Conjugates (ADC)
- Sacituzumab govitecan (anti-Trop2 ADC): for metastatic TNBC (ASCENT trial) and ER+/HER2-; delivers SN-38 (irinotecan metabolite) intracellularly
- T-DXd: HER2-low (IHC 1+ or 2+/ISH-) tumors - a new actionable category (DESTINY-Breast04)
G. PI3K/mTOR Pathway Inhibitors
- Alpelisib (PI3Kα inhibitor): for PIK3CA-mutated ER+/HER2- metastatic breast cancer (SOLAR-1 trial); combined with fulvestrant; side effects: hyperglycemia, rash, diarrhea
- Everolimus (mTOR inhibitor): combined with exemestane in metastatic ER+/HER2- disease; side effects: stomatitis, pneumonitis, hyperglycemia
H. Chemoprevention Summary
| Drug | Risk Reduction | Use | Key SE |
|---|---|---|---|
| Tamoxifen | 38% ↓ ER+ invasive cancer | Pre/postmenopausal high-risk | VTE, endometrial cancer |
| Raloxifene | Similar to tamoxifen for invasive | Postmenopausal only | VTE, no endometrial stimulation |
| Aromatase inhibitors | ~50-65% risk reduction | Postmenopausal high-risk | Arthralgias, osteoporosis |
9. MALE BREAST CANCER
- Rare (~1% of all breast cancers); peak age 60-70 years
- Risk factors: BRCA2 mutation (most important hereditary cause), Klinefelter syndrome (XXY), liver disease, estrogen exposure, obesity
- Almost all are ER+/PR+; treated with tamoxifen (not AIs unless orchiectomy performed, as testes are primary androgen source for aromatization)
- Stage for stage, prognosis similar to female breast cancer
10. QUICK-REFERENCE KEY FACTS FOR SURGERY EXAMS
| High-Yield Fact | Answer |
|---|---|
| Most common cause of bloody nipple discharge | Intraductal papilloma |
| Most common breast tumor in young women | Fibroadenoma |
| Most common type of breast cancer | Invasive ductal carcinoma (NST), ~70-80% |
| Organism in lactational abscess | S. aureus |
| Paget disease of nipple = | Extension of DCIS into nipple epidermis |
| Sentinel node technique developed | 1994 |
| ACOSOG Z0011 trial message | 1-2 positive SLNs in BCS + WBR → omit ALND |
| Tamoxifen mechanism | SERM - ER antagonist in breast, agonist in uterus/bone |
| Aromatase inhibitors side effect NOT seen | Endometrial cancer, VTE |
| Most commonly mutated gene in ER+ breast cancer | PIK3CA (~40%) |
| BRCA1-associated tumor type | Medullary, triple-negative |
| Best prognosis subtype | Mucinous/tubular carcinoma; Luminal A |
| CDK4/6 inhibitor + adjuvant approved | Abemaciclib (monarchE) |
| Most feared ALND complication | Lymphedema |
| Inflammatory breast cancer diagnosis | Clinical (peau d'orange + skin biopsy showing dermal lymphatic emboli) |
| WHCRA (1998) | Mandates insurance coverage for breast reconstruction |
Sources: Robbins & Kumar Basic Pathology; Sabiston Textbook of Surgery; Current Surgical Therapy 14e; Schwartz's Principles of Surgery 11e; Goodman & Gilman's Pharmacological Basis of Therapeutics; Katzung's Basic and Clinical Pharmacology 16e; Gray's Anatomy for Students; Goldman-Cecil Medicine; Harrison's Principles of Internal Medicine 22e; Basic Medical Biochemistry 6e
Abdomen 101- preclinicals, clinically, diseases, investigations, management from cpg, nice
Finding Sources
Finding Sources
Searching the Web
NICE guidelines abdominal conditions appendicitis bowel obstruction pancreatitis 2024 2025
Finding Sources
Finding Sources
Searching the Web
NICE guidelines acute appendicitis pancreatitis bowel obstruction hernia management site:nice.org.uk
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Searching the Web
NICE CKS acute abdomen appendicitis pancreatitis cholecystitis bowel obstruction management guidelines 2024
Finding Sources
Finding Sources
Searching the Web
IAP APA ACG acute pancreatitis guidelines 2024 management severity assessment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.