Anatomy of kidney
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
I now have excellent images and rich content. I have enough material to write a comprehensive, well-illustrated answer. Let me compose it now.
Anatomy of the Kidney
Sources: Brenner and Rector's The Kidney, 2-Volume Set | National Kidney Foundation Primer on Kidney Diseases, 8e | Medical Physiology (Boron & Boulpaep) | Histology: A Text and Atlas (Ross & Pawlina)
1. Position and General Features
The kidneys are paired, bean-shaped, retroperitoneal organs lying on either side of the vertebral column. They extend from T12 to L3 vertebrae. The right kidney sits slightly more caudal than the left (displaced by the liver).
| Parameter | Male | Female |
|---|---|---|
| Weight | 125-170 g | 115-155 g |
| Length (MRI) | ~12.4 cm | ~11.6 cm |
| Width | 5.0-7.5 cm | 5.0-7.5 cm |
| Thickness | 2.5-3.0 cm | 2.5-3.0 cm |
Each kidney is enclosed in a thin fibrous capsule (tough and nearly non-distensible) surrounded by perinephric fat, then the renal (Gerota's) fascia.
The Hilum
On the medial (concave) surface, the hilum is the entry/exit point for:
- Renal artery (enters)
- Renal vein (exits)
- Ureter (exits)
- Lymphatics and nerve plexus
The hilum opens into the renal sinus - a fat-filled space containing the renal pelvis, calyces, and vessels.
2. Gross Internal Structure
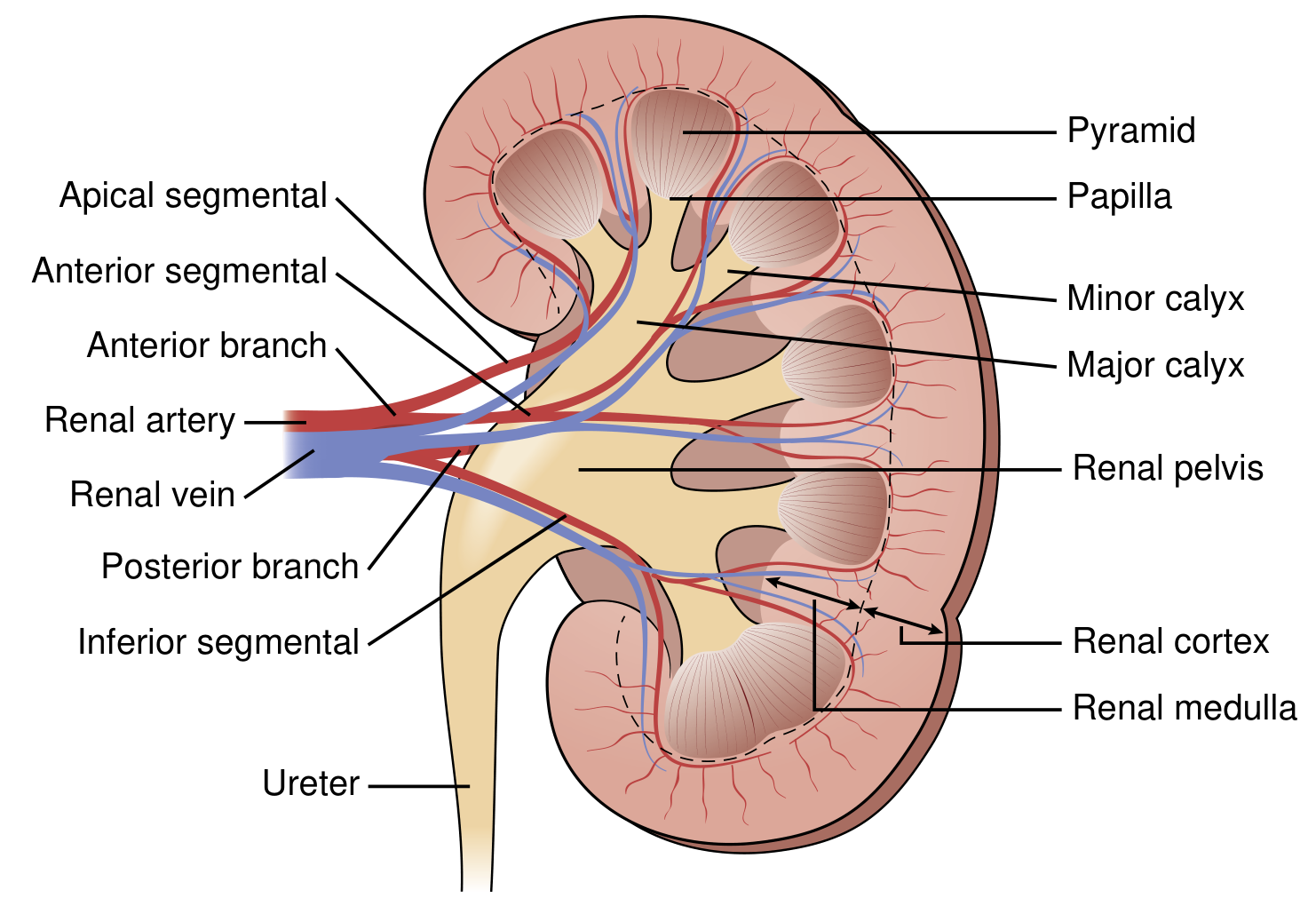
Fig. 1.2 - National Kidney Foundation Primer on Kidney Diseases, 8e
On bisection, two distinct zones are visible:
Cortex
- Outer reddish-brown, granular zone (~1 cm thick)
- Contains: renal corpuscles (glomeruli + Bowman's capsule), proximal convoluted tubules, distal convoluted tubules, cortical collecting ducts
- Receives ~90-95% of total renal blood flow
- Columns of Bertin: extensions of cortex dipping between medullary pyramids
- Medullary rays (of Ferrein): striations projecting from medulla into cortex, containing straight tubules and collecting ducts
Medulla
- Inner, lighter-colored, striated zone
- Contains: loops of Henle (thin and thick limbs), medullary collecting ducts, vasa recta
- Lacks glomeruli
- Divided into outer medulla (outer stripe + inner stripe) and inner medulla
Renal Pyramids
- 8-18 conical structures in the medulla
- Base faces corticomedullary junction; apex (papilla) points toward renal sinus
- The papilla is perforated by collecting duct openings at the area cribrosa
- A single pyramid + its overlying cortical cap = renal lobe
Collecting System
- Minor calyces - cup-shaped structures receiving urine from papillae
- Major calyces (2-3) - formed by convergence of minor calyces
- Renal pelvis - expanded upper portion of the ureter, lined by urothelium (transitional epithelium)
- Ureter - 28-34 cm long, exits at the ureteropelvic junction
3. The Nephron - Functional Unit
Each kidney contains approximately 1 million nephrons (range: 600,000 to 2 million). The nephron is the basic structural and functional unit.
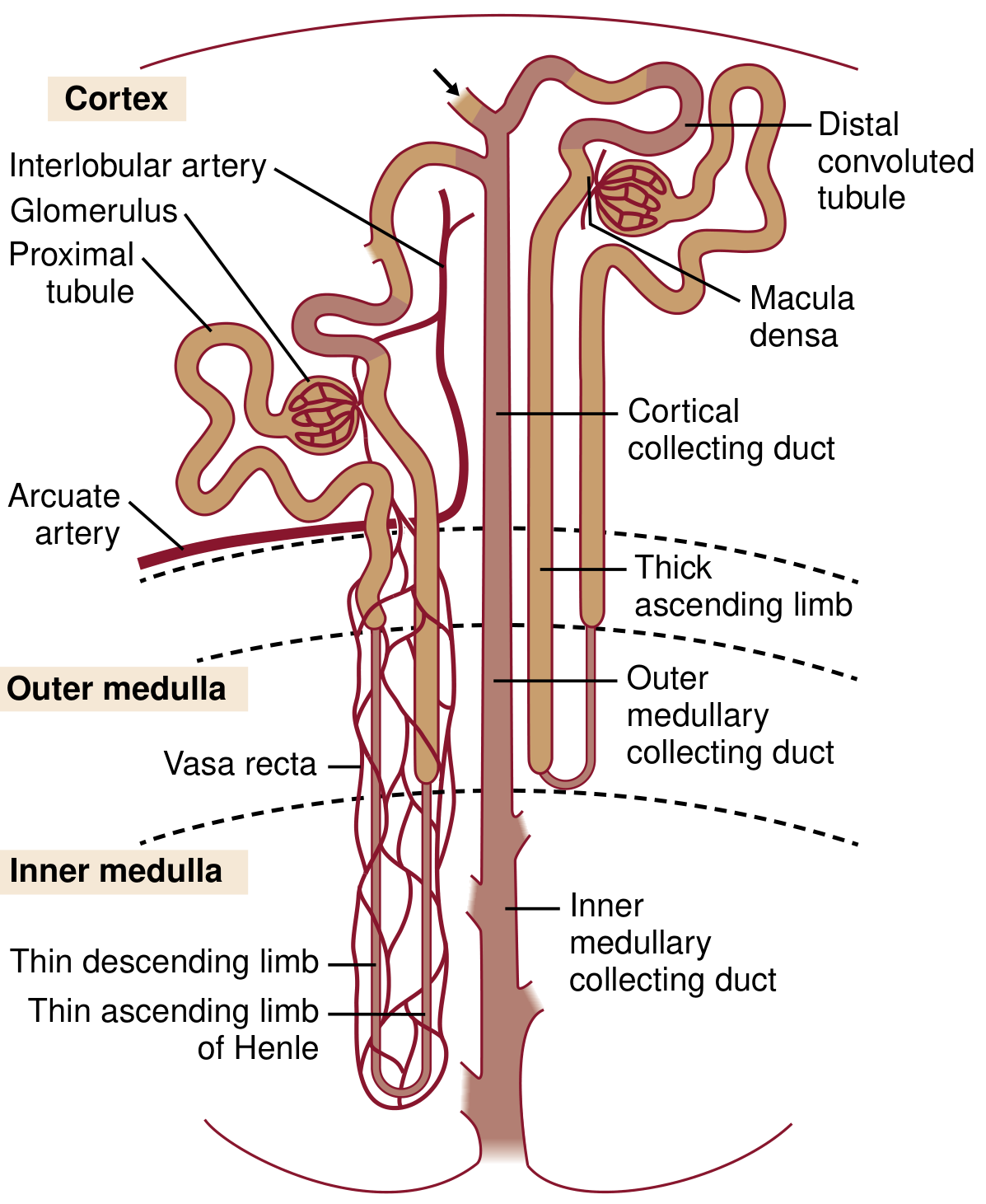
Fig. 1.3 - National Kidney Foundation Primer on Kidney Diseases, 8e
Types of Nephrons
| Type | Location | Loop of Henle |
|---|---|---|
| Superficial (cortical) | Outer cortex | Short loop, stays in outer medulla |
| Juxtamedullary | Deep cortex (near medulla) | Long loop, penetrates deep into inner medulla |
Components of the Nephron
A. Renal Corpuscle (Glomerulus + Bowman's Capsule)
- Spherical structure, ~200 µm diameter
- Located in the cortex
- Glomerulus: tuft of fenestrated capillaries fed by afferent arteriole, drained by efferent arteriole
- Bowman's capsule: double-walled epithelial cup surrounding the glomerulus
- Parietal layer: simple squamous epithelium
- Visceral layer: specialized podocytes with foot processes (pedicels) that interdigitate around capillaries
- Urinary (Bowman's) space between layers collects filtrate
Glomerular Filtration Barrier (3 layers):
- Fenestrated capillary endothelium (covered by glycocalyx - negatively charged)
- Glomerular basement membrane (GBM) - type IV collagen, laminin, heparan sulfate
- Podocyte foot processes with filtration slits bridged by the slit diaphragm (nephrin, podocin)
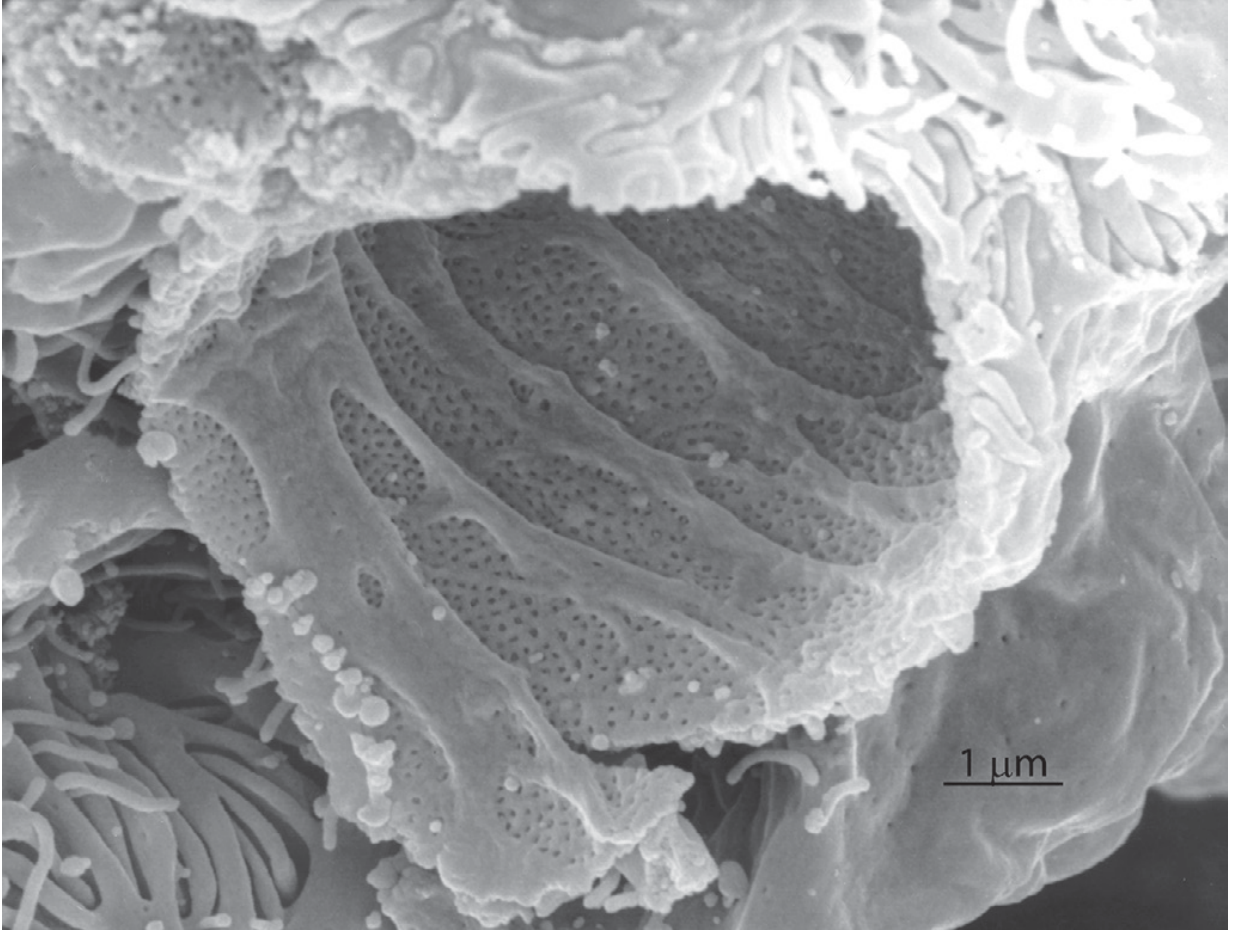
Fig. 2.12 - Brenner and Rector's The Kidney: SEM of glomerular capillary showing fenestrae and podocyte foot processes
B. Proximal Tubule
- Longest segment; begins at urinary pole of Bowman's capsule
- Proximal Convoluted Tubule (PCT): coils in the cortex; tall cells with abundant microvilli (brush border) maximizing reabsorptive surface
- Proximal Straight Tubule (PST): descends into medullary ray/outer stripe
- Reabsorbs ~2/3 of glomerular filtrate (Na+, glucose, amino acids, HCO₃⁻, water)
C. Loop of Henle
- Creates the medullary osmotic gradient essential for urine concentration
- Thin descending limb: permeable to water, impermeable to solutes; descends into medulla
- Thin ascending limb (juxtamedullary nephrons): impermeable to water, permeable to NaCl
- Thick ascending limb (TAL): actively transports NaCl (NKCC2 cotransporter); impermeable to water - the diluting segment
D. Distal Tubule
- Distal Convoluted Tubule (DCT): located in cortex; contains cells with basolateral Na/K-ATPase and apical Na-Cl cotransporter (NCC)
- Fluid is maximally dilute here (~100 mOsm/kg)
- The DCT contacts its own glomerulus at the juxtaglomerular apparatus (JGA)
E. Collecting Duct System
- Connecting tubule → cortical collecting duct → outer medullary collecting duct → inner medullary collecting duct (duct of Bellini)
- Principal cells: regulated by aldosterone (Na+ reabsorption) and ADH/vasopressin (water reabsorption via aquaporin-2)
- Intercalated cells: regulate acid-base balance (H+ and K+ secretion/reabsorption)
- Urine drains from collecting duct openings at area cribrosa into minor calyces
4. Juxtaglomerular Apparatus (JGA)
Located where the distal tubule returns to contact its own glomerulus. Three components:
| Component | Cell Type | Function |
|---|---|---|
| Macula densa | Specialized DCT cells (tall, crowded nuclei) | Sense tubular NaCl; regulate GFR and renin release |
| Juxtaglomerular (granular) cells | Modified smooth muscle of afferent arteriole | Synthesize and secrete renin |
| Extraglomerular mesangial (Lacis) cells | Between macula densa and glomerulus | Signal transduction |
The JGA is the structural basis for tubuloglomerular feedback and the renin-angiotensin-aldosterone system (RAAS).
5. Blood Supply
The kidneys receive ~20% of cardiac output despite comprising <0.5% of body weight.
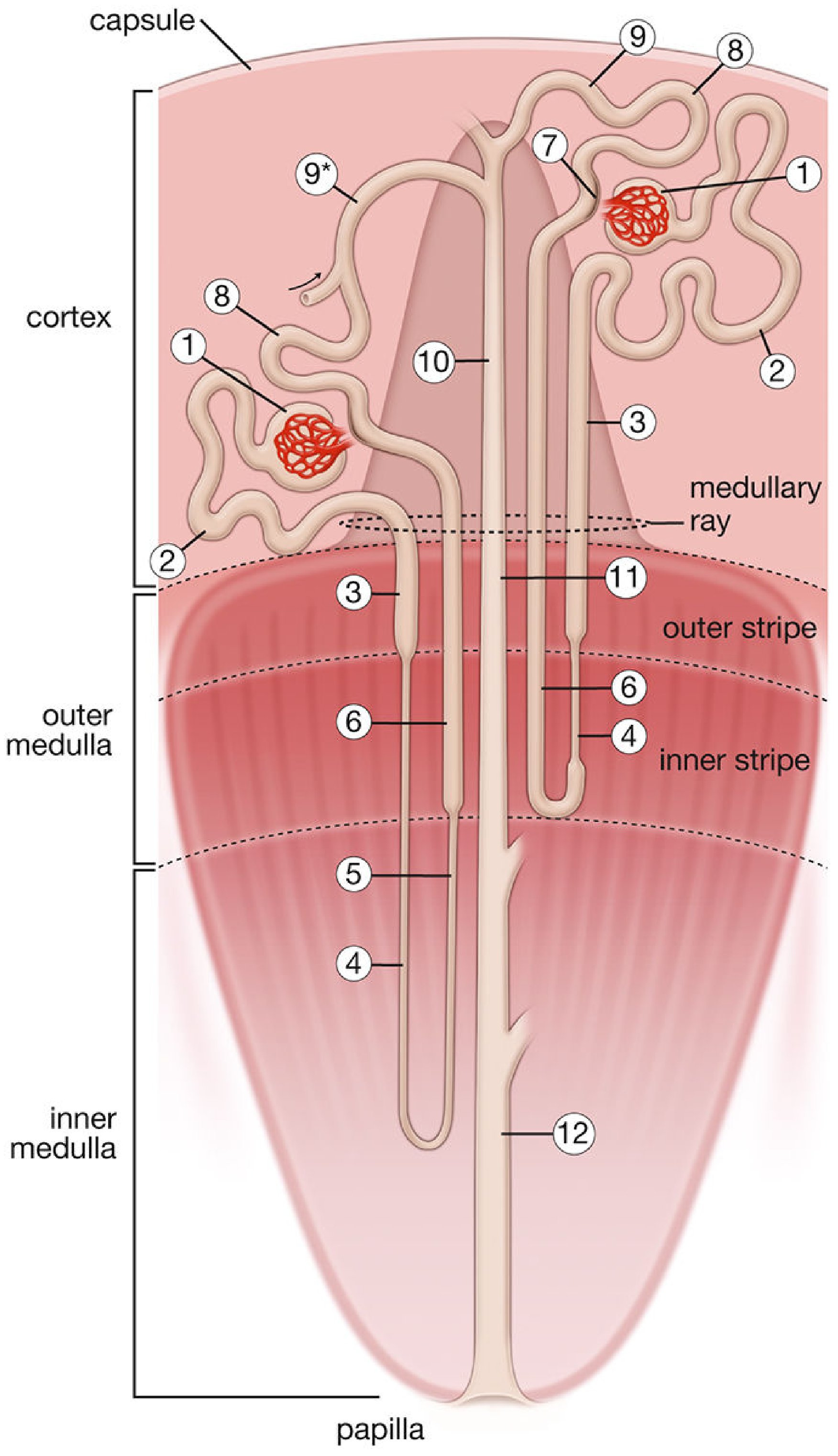
Histology: A Text and Atlas - nephron and vascular supply
Arterial Supply (Hierarchical)
Renal artery → anterior + posterior divisions → segmental (lobar) arteries (5 segments, end arteries - no collaterals) → interlobar arteries (travel in columns of Bertin) → arcuate arteries (run along corticomedullary junction) → interlobular (cortical radiate) arteries → afferent arterioles → glomerular capillaries → efferent arterioles
After the efferent arteriole:
- Superficial nephrons: peritubular capillaries surround cortical tubules
- Juxtamedullary nephrons: vasa recta - long hairpin capillaries that descend into medulla parallel to loops of Henle, form the countercurrent exchange system for urine concentration
Venous Drainage
Peritubular capillaries → interlobular veins → arcuate veins → interlobar veins → renal vein → inferior vena cava (IVC)
- The venous system has extensive collaterals (unlike arteries)
Clinical Note
The 5 segmental arteries are end arteries - occlusion causes segmental infarction with no collateral rescue.
6. Lymphatics and Innervation
- Lymphatics: drain into paraaortic (lumbar) lymph nodes; run with the blood vessels in the renal sinus
- Innervation: sympathetic fibers from T8-L1 via the renal plexus (derived from celiac and aorticorenal ganglia); control vascular tone, renin secretion, and tubular transport. The kidney has no parasympathetic innervation.
7. Summary Table
| Region | Key Contents | Primary Function |
|---|---|---|
| Renal cortex | Glomeruli, PCT, DCT, cortical collecting duct | Filtration, bulk reabsorption |
| Outer medulla (outer stripe) | PST, thick ascending limb | Active NaCl transport |
| Outer medulla (inner stripe) | Thin descending limb, thin ascending limb, vasa recta | Countercurrent multiplication |
| Inner medulla | Inner collecting duct, thin limbs of long loops | Urine concentration |
| Renal sinus | Pelvis, calyces, major vessels, fat | Urine collection and drainage |
Coverings of kidney
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Reading File
Loading Image
I now have all the content and images needed for a thorough, well-illustrated answer.
Coverings of the Kidney
The kidney has four concentric coverings, arranged from innermost to outermost. Each layer has distinct structural, functional, and clinical significance.
Sources: Gray's Anatomy for Students | Fischer's Mastery of Surgery, 8e | Campbell-Walsh-Wein Urology | Brenner and Rector's The Kidney
Overview - Layers from Inside Out
| Layer | Name | Also Called |
|---|---|---|
| 1st (innermost) | Fibrous capsule | Renal capsule |
| 2nd | Perirenal (perinephric) fat | Perirenal fat capsule |
| 3rd | Renal fascia | Gerota's fascia, fascia of Gerota |
| 4th (outermost) | Pararenal (paranephric) fat | Pararenal fat body |
Schematic Cross-Section
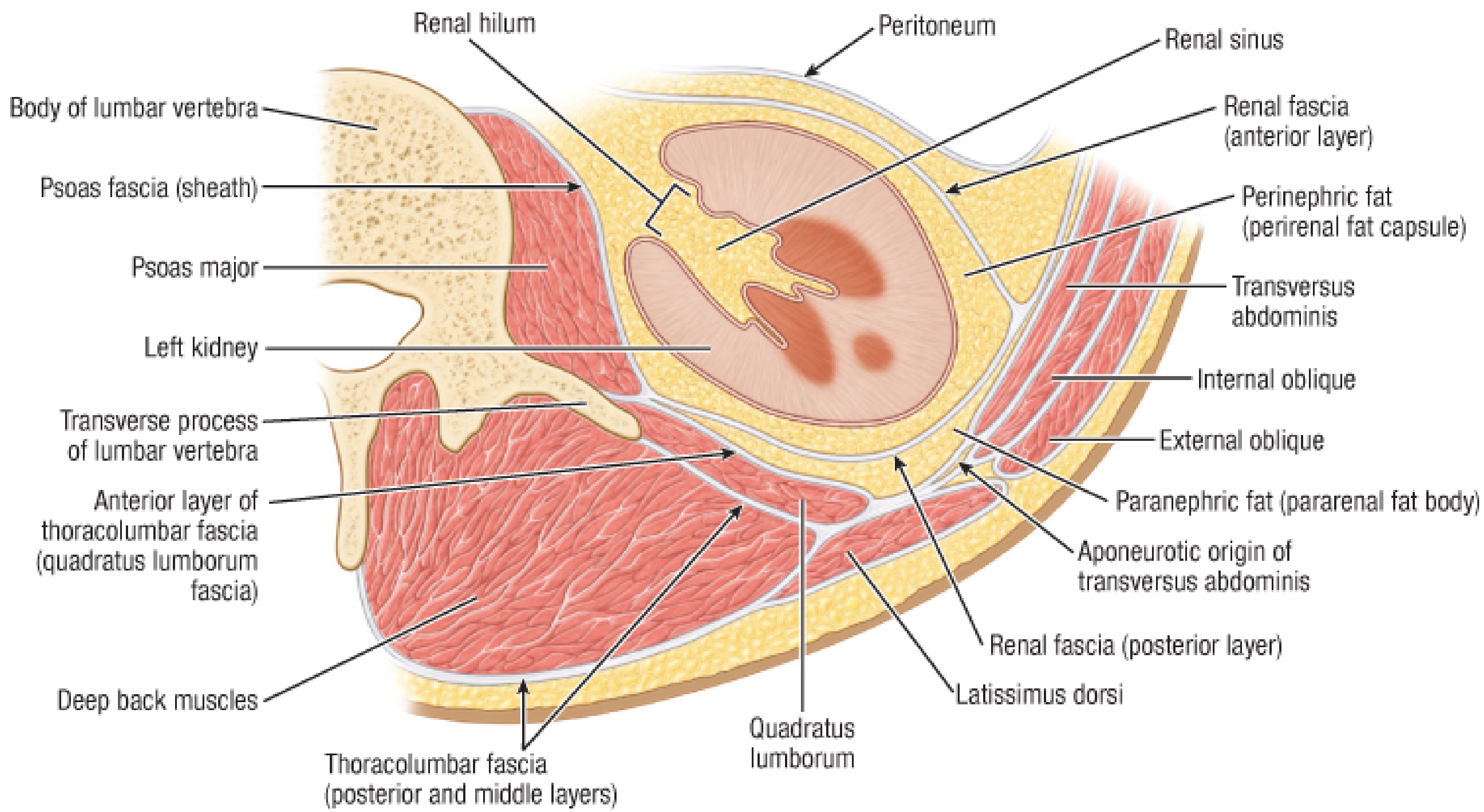
Fig. 281.2 - Fischer's Mastery of Surgery, 8e: Renal fascia and retroperitoneal fat, schematic transverse section
1. Fibrous Capsule (Renal Capsule) - Innermost
- A tough, thin fibrous layer directly investing the renal parenchyma
- Composed of collagen and smooth muscle fibers
- Continuous at the hilum with the connective tissue of the renal sinus, where it surrounds the blood vessels and pelvis
- In health, it is smooth and easily stripped from the kidney surface
- In disease (e.g., chronic pyelonephritis, renal carcinoma), the capsule becomes adherent and cannot be cleanly removed
- Connected to the overlying renal fascia by fine connective tissue fiber bundles
- Clinical note: The non-distensible nature of the capsule means that acute renal swelling (e.g., pyelonephritis, obstruction) causes significant pain - the capsule has a rich pain nerve supply (sympathetic afferents T10-L1)
2. Perirenal (Perinephric) Fat - Perirenal Fat Capsule
- A layer of adipose tissue sitting between the fibrous capsule and the renal fascia
- Completely surrounds the kidney and fills the perinephric space
- Extends into the renal sinus through the hilum, surrounding the renal pelvis, calyces, and intrarenal vessels
- Fine, lighter yellow in texture - distinct from the coarser, yellow-orange pararenal fat (a useful surgical distinction during retroperitoneal dissection)
- Acts as a mechanical cushion protecting the kidney from trauma
- Also provides thermal insulation
- The perinephric space (bounded by renal fascia) also contains: the adrenal gland, ureter, renal vascular pedicle, and gonadal vessels
3. Renal Fascia (Gerota's Fascia) - The Key Investing Layer
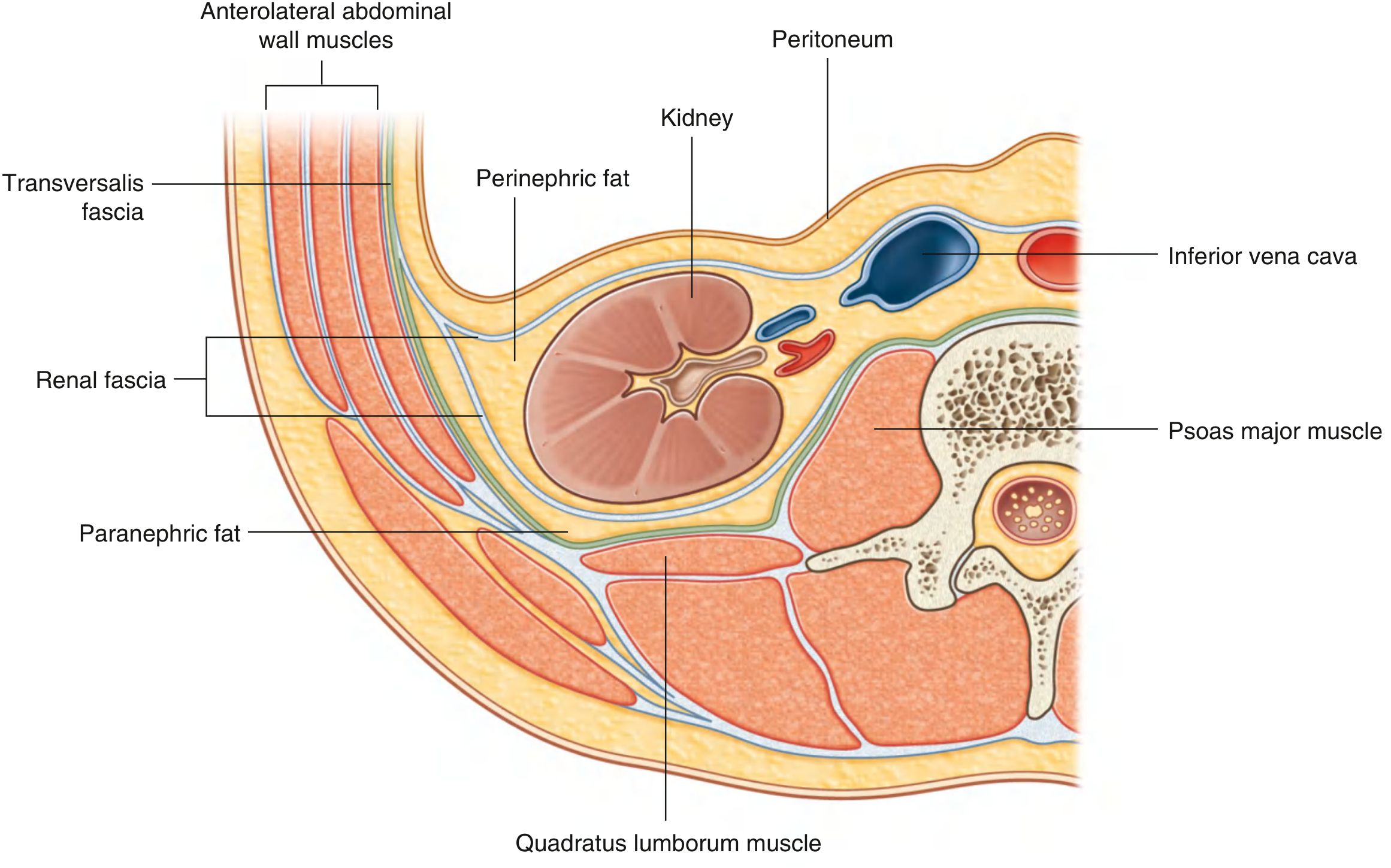
Fig. 4.155 - Gray's Anatomy for Students: Organization of Fat and Fascia Surrounding the Kidney
Named after the Romanian anatomist Dimitrie D. Gerota (1867-1939), the renal fascia is a membranous condensation of extraperitoneal fascia. It is the most surgically important covering.
Two Laminae
The renal fascia has two layers that enclose the perinephric space:
| Lamina | Name | Relations |
|---|---|---|
| Anterior | Fascia of Toldt (prerenal fascia) | Lies anterior to the kidney; continuous with peritoneum anteriorly |
| Posterior | Fascia of Zuckerkandl (retrorenal fascia) | Lies posterior; thicker and more visible radiographically |
Attachments and Extents
- Superiorly: Anterior and posterior layers fuse above the suprarenal gland and blend with the fascia of the diaphragm - the compartment is closed superiorly
- Laterally: Anterior and posterior layers fuse to form the lateroconal fascia, which continues to the transversalis fascia
- Medially:
- Anterior layer passes over the hilar vessels and fuses with connective tissue around the aorta and IVC; may cross the midline to the opposite side
- Posterior layer passes medially between kidney and quadratus lumborum to fuse with psoas fascia
- Inferiorly: The compartment is open inferiorly - the two layers do not fuse; they taper into a cone-like shape and continue around the ureter as periureteric fascia descending into the pelvis
Contents of the Perirenal Space (inside Gerota's fascia)
- Kidney + fibrous capsule
- Perinephric fat
- Suprarenal (adrenal) gland (usually separated by a thin septum)
- Proximal ureter and gonadal vessels
- Renal vascular pedicle
Clinical Significance of Gerota's Fascia
- Perinephric collections - the fascia limits spread of perinephric hematoma, urinoma, or abscess; they tend to spread inferiorly (the only open end)
- Renal cell carcinoma (RCC) staging - invasion through Gerota's fascia = pT3b/T4 disease (upstages the tumor)
- Radical nephrectomy - performed outside Gerota's fascia, removing kidney + fat + adrenal en bloc
- Simple nephrectomy - performed inside Gerota's fascia
- Renal transplantation - Gerota's fascia is opened to expose the kidney
4. Pararenal (Paranephric) Fat - Outermost
- Located outside the renal fascia
- Positioned between:
- Posteriorly: renal fascia and quadratus lumborum fascia (anterior layer of thoracolumbar fascia)
- Anteriorly: renal fascia and parietal peritoneum
- Most prominent posterolateral to the kidney
- Coarser, yellow-orange in colour
- The renal fascia sends collagen fiber bundles through the paranephric fat, anchoring the kidney in position
- Variable in thickness; can be substantial in obese individuals
Summary Diagram Relationships
Retroperitoneal Space Compartments
The renal fascia divides the retroperitoneal space into three compartments:
| Compartment | Boundaries | Contents |
|---|---|---|
| Anterior pararenal space | Posterior parietal peritoneum (ant.) / Anterior renal fascia (post.) | Ascending & descending colon, duodenum, pancreas |
| Perirenal space | Within Gerota's fascia | Kidney, adrenal, ureter, perinephric fat |
| Posterior pararenal space | Posterior renal fascia (ant.) / Transversalis fascia (post.) | Paranephric fat only |
Structures That Must Be Incised to Reach the Kidney
Any surgical approach to the kidney requires sequential incision of:
- Skin and subcutaneous fat
- Muscles (flank approach: external oblique, internal oblique, transversus abdominis)
- Transversalis fascia
- Pararenal (paranephric) fat - posterior pararenal space
- Renal fascia (Gerota's fascia) - mandatory for all renal surgery
- Perirenal (perinephric) fat
- Fibrous capsule - only if operating directly on the parenchyma
This is a shared conversation. Sign in to Orris to start your own chat.