Synthetic mid urethral slings diagrams
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Searching Content
"cdn.orris.care" in /textbooks/9780323546423
Finding Sources
The images for Fig. 125.9 (retropubic) and Fig. 125.11 (single-incision) appear to be embedded in the text as anatomical labels rather than as URL-linked images in that block. The two main diagrams I've already retrieved (the trocars/prosthetics grid and the transobturator approach anatomy) are the key visual assets. Let me now compile everything into a comprehensive answer with the images and clinical detail.
Synthetic Mid-Urethral Slings (MUS) - Diagrams & Overview
Synthetic mid-urethral slings are the most commonly performed surgical procedure for stress urinary incontinence (SUI). Here is a structured overview with the key textbook diagrams.
Device Types and Trocars
Fig. 125.8 - MUS trocars and prosthetics (from Campbell-Walsh-Wein Urology):
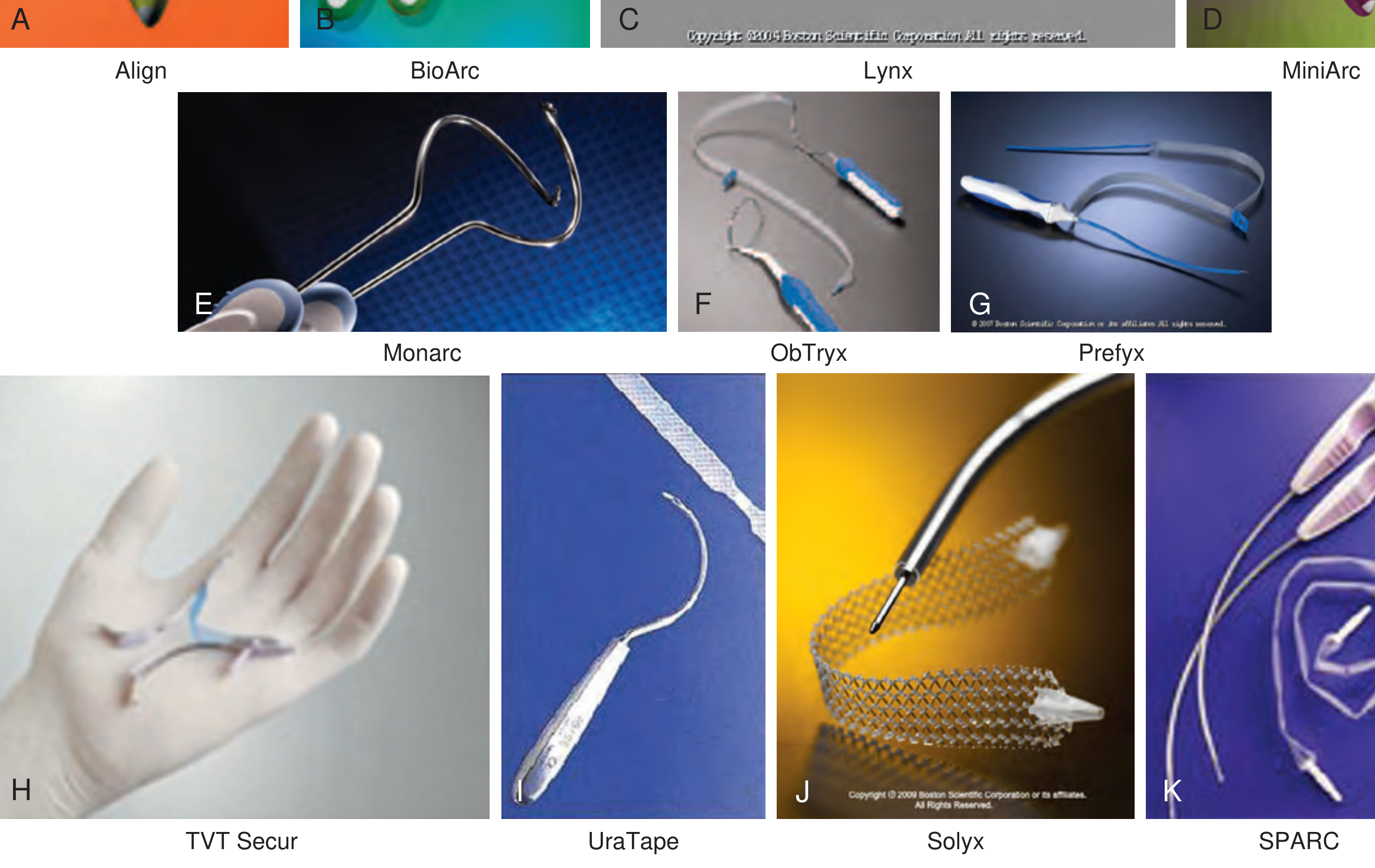
This figure shows the variety of sling systems: A. Align, B. BioArc, C. Lynx, D. MiniArc, E. Monarc (transobturator outside-in), F. ObTryx, G. Prefyx, H. TVT Secur (single-incision), I. UraTape, J. Solyx, K. SPARC. The standard sling consists of two curved 5-mm insertion trocars and a 40-cm long, 1.1-cm wide polypropylene mesh strip.
1. Retropubic Approach (TVT - Tension-Free Vaginal Tape)
Fig. 125.9 - Retropubic MUS placement:
The retropubic sling passes through the space of Retzius (retropubic space), exiting via two small suprapubic stab incisions ~2 cm lateral to the midline.
Key anatomical landmarks:
- The trocar passes from the vaginal incision (1.5 cm from the external meatus) upward through the endopelvic fascia
- Traverses the space of Retzius, stays in close contact with the inferior pubic bone surface
- Exits suprapubically just above the symphysis pubis
- Sling anchors to the endopelvic fascia
Technique steps:
- Two suprapubic stab incisions, 2 cm lateral to midline just above the symphysis
- Midline vaginal incision 1.5 cm, 1.5 cm proximal to the urethral meatus
- Dissection laterally to the pubocervical (endopelvic) fascia bilaterally (not perforated)
- Trocar passed bottom-up (vagina to abdomen) or top-down with a catheter guide deflecting the bladder
- Cystoscopy mandatory with 70-degree lens to exclude bladder/urethral perforation
- Sling placed loosely; tension adjusted with a clamp between sling and urethra
2. Transobturator Approach (TOT / TVT-O)
Fig. 125.10 - Transobturator MUS placement:
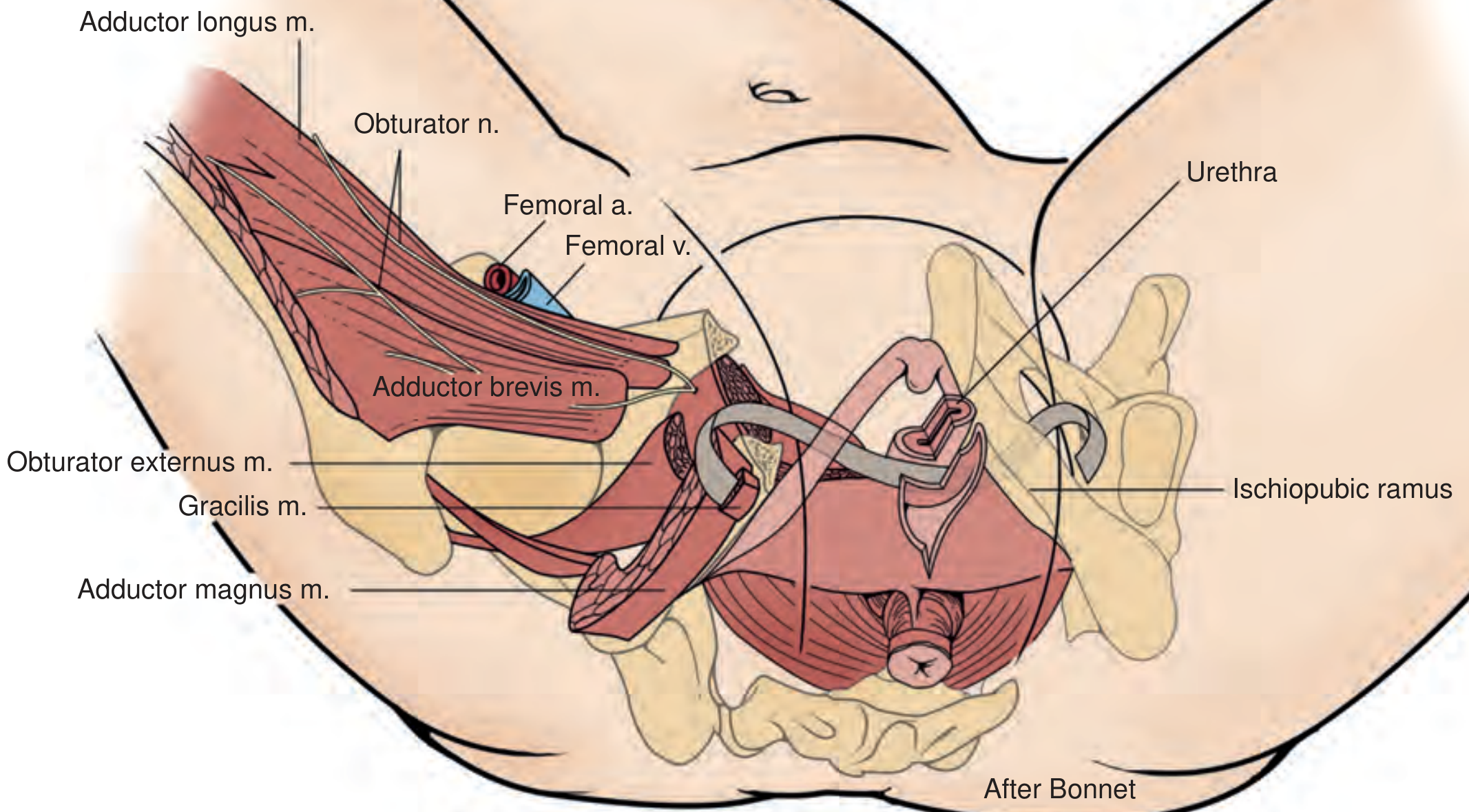
The sling passes through the obturator foramen, anchoring in the obturator internus and externus muscle/fascia, and exits via stab incisions in the groin crease at the level of the clitoris.
Key structures transited (visible in diagram):
- Adductor longus muscle (medial thigh)
- Obturator nerve (at risk)
- Obturator externus muscle
- Adductor brevis and gracilis muscles
- Ischiopubic ramus (bony landmark)
Two sub-techniques:
- Outside-in (TOT): Puncture incision in the groin crease at the inferior pubic ramus / adductor longus junction, trocar perforates obturator membrane and exits the vaginal incision - guided by the surgeon's index finger
- Inside-out (TVT-O): Vaginal incision first, introducer passed at 45 degrees through the obturator membrane, helical passer rotated to exit the interthigh stab incision
3. Single-Incision Sling (SIS / Mini-sling)
Fig. 125.11 - Single-incision MUS, two configurations:
- (A) Hammock position - anchors into the obturator internus muscle bilaterally
- (B) U-shaped position - anchors into connective tissue of the urogenital diaphragm (endopelvic fascia) behind the pubic bone
Short polypropylene mesh segment with pointed self-anchoring ends, placed through a single vaginal incision only - no abdominal or thigh exit incisions. Tension set when a hemostat tip passes easily between sling and urethra.
Material
All synthetic MUS are made of type 1 macroporous polypropylene mesh (pore size >75 microns), which allows tissue ingrowth, resists infection, and avoids the problems of microporous mesh.
Mechanism of Action
The MUS works by:
- Impeding posterior urethral wall movement during stress maneuvers (Valsalva), directing it anteriorly
- Compressing the urethral lumen by inward movement of the posterior wall under the sling
- Dynamic urethral kinking during stress events (Lo et al., 2001)
- The sling is anchored broadly - not just at the midline - which explains why continence is maintained even after sling incision for obstruction in many patients
Outcomes at a Glance
| Type | ~10-year objective cure | Key complication |
|---|---|---|
| Retropubic (TVT) | 84-91% | Bladder perforation (trocar passage), voiding dysfunction |
| Transobturator (TOT/TVT-O) | Similar efficacy | Groin/thigh pain, obturator nerve injury |
| Single-incision | Lower (variable) | Less data; early versions had higher failure rates |
Overall ~90% cure rate reported at 17-year follow-up (Bailey & Love's Surgery, p. 6105). Cystoscopy is mandatory after all approaches to exclude bladder and urethral injury.
- Campbell-Walsh-Wein Urology, 3-Volume Set, Chapter 125 (Mid-Urethral Slings)
- Bailey and Love's Short Practice of Surgery 28th Edition, Chapter 83
This is a shared conversation. Sign in to Orris to start your own chat.