10 common ecg changes
Reading File
Finding Sources
Finding Sources
Searching the Web
10 common ECG changes clinical interpretation
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching Images
ECG changes ST elevation STEMI myocardial infarction
Finding Sources
Finding Sources
Searching Images
atrial fibrillation ECG irregularly irregular no P waves
Reading File
Searching Images
heart block first degree second degree third degree ECG PR interval
I now have sufficient material to provide a comprehensive, well-illustrated answer. Here are the 10 most common ECG changes:
10 Common ECG Changes
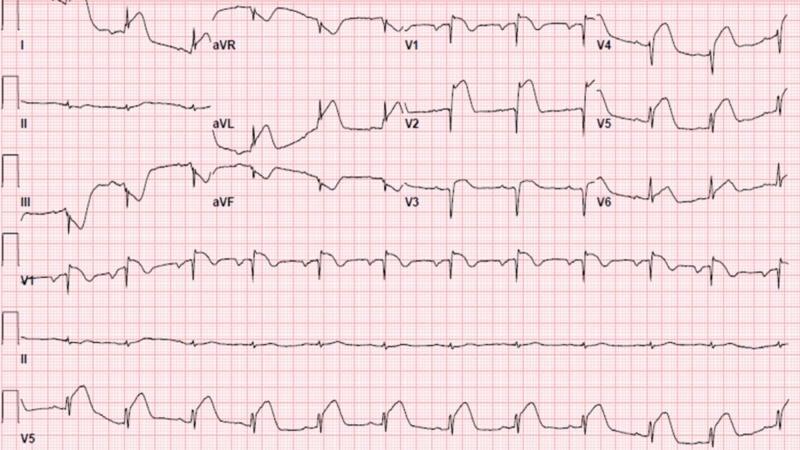
1. ST-Segment Elevation (STEMI)
Definition: ST elevation ≥1 mm in ≥2 contiguous limb leads or ≥2 mm in ≥2 contiguous precordial leads.
Causes: STEMI, Prinzmetal (vasospastic) angina, pericarditis (saddle-shaped, diffuse), left ventricular aneurysm, Brugada pattern.
Key features:
- Convex ("tombstone") morphology in STEMI
- Reciprocal ST depression in opposing leads
- Hyperacute (peaked, broad) T-waves in earliest phase
- Evolves → pathological Q waves over hours
Lead localization:
| Leads | Territory | Artery |
|---|---|---|
| V1–V4 | Anterior | LAD |
| II, III, aVF | Inferior | RCA |
| I, aVL, V5–V6 | Lateral | LCx |
2. ST-Segment Depression
Definition: ST depression >0.5–1 mm below the isoelectric line.
Causes: Subendocardial ischemia/NSTEMI, reciprocal change in STEMI, LVH strain pattern, digoxin effect (reverse "tick" / hockey stick shape), hypokalemia.
Morphologies:
- Horizontal/downsloping → most ominous (ischemia)
- Upsloping → less specific
- Digoxin ("scooped") → concave downsloping with short QT
3. T-Wave Inversion
Definition: Negative T-wave in a lead where it is normally upright (T normally upright in I, II, V3–V6).
Causes:
- Myocardial ischemia / NSTEMI (deep symmetrical inversion)
- Wellens' syndrome — deep symmetric T-wave inversion in V2–V3 = critical proximal LAD stenosis
- RV strain (acute PE) — V1–V4 ± III
- LVH strain — lateral leads
- Hypertrophic cardiomyopathy — deep diffuse inversion
- Normal variant — V1–V2 (and V3 in women)
4. Pathological Q Waves
Definition: Q-wave duration >40 ms (>1 mm wide) or depth >25% of the following R wave, in ≥2 contiguous leads.
Significance: Indicates transmural myocardial necrosis (completed infarction). Develop within 6–24 hours of STEMI and may persist permanently.
Normal Q waves (septal depolarization) are small (<40 ms) in I, aVL, V5–V6 — do not confuse.
5. Atrial Fibrillation (AF)
Definition: Irregularly irregular rhythm with absent P waves replaced by chaotic fibrillatory (f) waves, most visible in V1.
Key ECG features:
- No identifiable P waves
- Irregular baseline (f-waves, 350–600/min)
- Irregularly irregular R-R intervals
- Narrow QRS (unless aberrant conduction/pre-excitation)
- Ventricular rate depends on AV nodal conduction

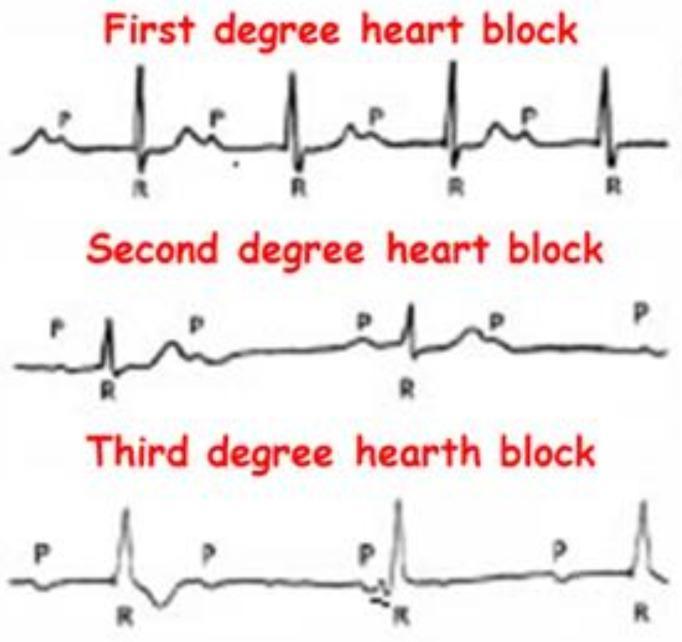
6. AV Blocks (Heart Block)
Three degrees:
| Degree | PR Interval | Dropped beats | Notes |
|---|---|---|---|
| 1st degree | >200 ms (>5 small sq) | None | All P waves conducted; benign |
| 2nd degree — Mobitz I (Wenckebach) | Progressive lengthening | Periodic | Group beating; AV node level |
| 2nd degree — Mobitz II | Fixed | Sudden | Below AV node; risk of complete block |
| 3rd degree (Complete) | AV dissociation | All | P & QRS completely independent; escape rhythm |
7. Bundle Branch Blocks (BBB)
Rule: BBB = QRS duration ≥120 ms (≥3 small squares).
Right Bundle Branch Block (RBBB):
- RSR' ("M-shape") in V1
- Wide slurred S wave in I, V6
- Causes: PE, RV overload, congenital heart disease, normal variant
Left Bundle Branch Block (LBBB):
- Broad notched R wave in I, aVL, V5–V6
- Deep QS in V1
- Causes: IHD, dilated cardiomyopathy, hypertension
- ⚠️ New LBBB with chest pain = STEMI equivalent (Sgarbossa criteria apply)
8. Left Ventricular Hypertrophy (LVH)
Common voltage criteria (Sokolow–Lyon):
- S in V1 + R in V5 or V6 ≥35 mm
- R in aVL ≥11 mm
Associated changes (strain pattern):
- ST depression + asymmetric T-wave inversion in I, aVL, V5–V6
- Left axis deviation
- Broad, notched P wave (left atrial enlargement) — P-mitrale
Note: Voltage criteria alone have ~50% sensitivity; strain pattern increases specificity. — Harrison's Principles of Internal Medicine 22E

9. Prolonged QT Interval
Definition: QTc >440 ms (men), >460 ms (women). QTc = QT ÷ √RR (Bazett formula).
Danger: QTc >500 ms significantly increases risk of Torsades de Pointes (polymorphic VT → VF → sudden death).
Causes — "ACUTE":
- Antiarrhythmics (amiodarone, sotalol, quinidine)
- Cardiac (ischemia, myocarditis)
- Underelectrolytes (↓K⁺, ↓Mg²⁺, ↓Ca²⁺)
- Toxins/drugs (antipsychotics, macrolides, TCAs)
- Endocrine (hypothyroidism)
- Congenital long QT syndromes (LQTS1, 2, 3)
10. Sinus Tachycardia / Sinus Bradycardia
Sinus Tachycardia (HR >100 bpm):
- Regular rhythm, normal P-waves (upright in II), PR <200 ms
- Causes: fever, pain, hypovolemia, anemia, PE, thyrotoxicosis, sympathomimetics
- Never a primary diagnosis — always find and treat the cause
Sinus Bradycardia (HR <60 bpm):
- Regular rhythm, normal P-waves
- Causes: athlete's heart (normal), inferior MI (RCA → SA node), hypothyroidism, hypothermia, beta-blockers, raised ICP (Cushing reflex)
- Treat only if symptomatic or hemodynamically compromised
Quick Reference Table
| # | ECG Change | Key Feature | Classic Cause |
|---|---|---|---|
| 1 | ST elevation | Convex ↑, reciprocal depression | STEMI, pericarditis |
| 2 | ST depression | Horizontal/downsloping | NSTEMI, LVH strain, digoxin |
| 3 | T-wave inversion | Deep symmetrical | Ischemia, Wellens', PE |
| 4 | Pathological Q waves | >40 ms, >25% R wave | Old MI / transmural necrosis |
| 5 | Atrial fibrillation | Irregularly irregular, no P waves | HTN, valvular disease, thyrotoxicosis |
| 6 | AV block | PR prolonged / dropped beats / dissociation | Inferior MI, drugs, degenerative |
| 7 | Bundle branch block | QRS ≥120 ms, RSR' or broad R | IHD, PE, cardiomyopathy |
| 8 | LVH | High voltage + strain pattern | Hypertension, AS, HCM |
| 9 | Long QT | QTc >440–460 ms | Drugs, electrolytes, congenital |
| 10 | Sinus brady/tachy | Rate <60 or >100, normal morphology | Systemic illness, athlete, MI |
Sources: Harrison's Principles of Internal Medicine 22E; Tintinalli's Emergency Medicine; Fuster & Hurst's The Heart 15E; Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.