Give me detailed explained notes of hip bone and femur mbbs level notes from netters atlas grays anatomy bd chudasia and klm
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
I now have everything I need to write comprehensive MBBS-level notes. Let me compile the complete, detailed notes:
HIP BONE & FEMUR — MBBS LEVEL ANATOMY NOTES
Sources: Gray's Anatomy for Students | THIEME Atlas of Anatomy | Netter's Atlas | BD Chaurasia | KLM
PART 1: THE HIP BONE (Os Coxae / Innominate Bone)
1.1 Overview
The hip bone (os coxae, innominate bone) is a large, irregular flat bone that forms the lateral wall of the pelvis. It is composed of three parts that fuse in early adulthood:
| Part | Ossification | Contribution to Acetabulum |
|---|---|---|
| Ilium | Flat bone, endochondral | 2/5 (upper) |
| Ischium | Endochondral | 2/5 (posteroinferior) |
| Pubis | Endochondral | 1/5 (anteroinferior) |
Key Point (BD Chaurasia / KLM): All three parts meet at the acetabulum via the triradiate cartilage (Y-shaped growth plate). This fuses between 14-16 years of life (THIEME Atlas).
The two hip bones articulate:
- With each other anteriorly at the pubic symphysis (fibrocartilaginous)
- With the sacrum posteriorly at the sacroiliac joints (synovial + fibrous)
Together they form the pelvic girdle and the bony pelvic ring - a structure critical for weight transfer from trunk to lower limbs.
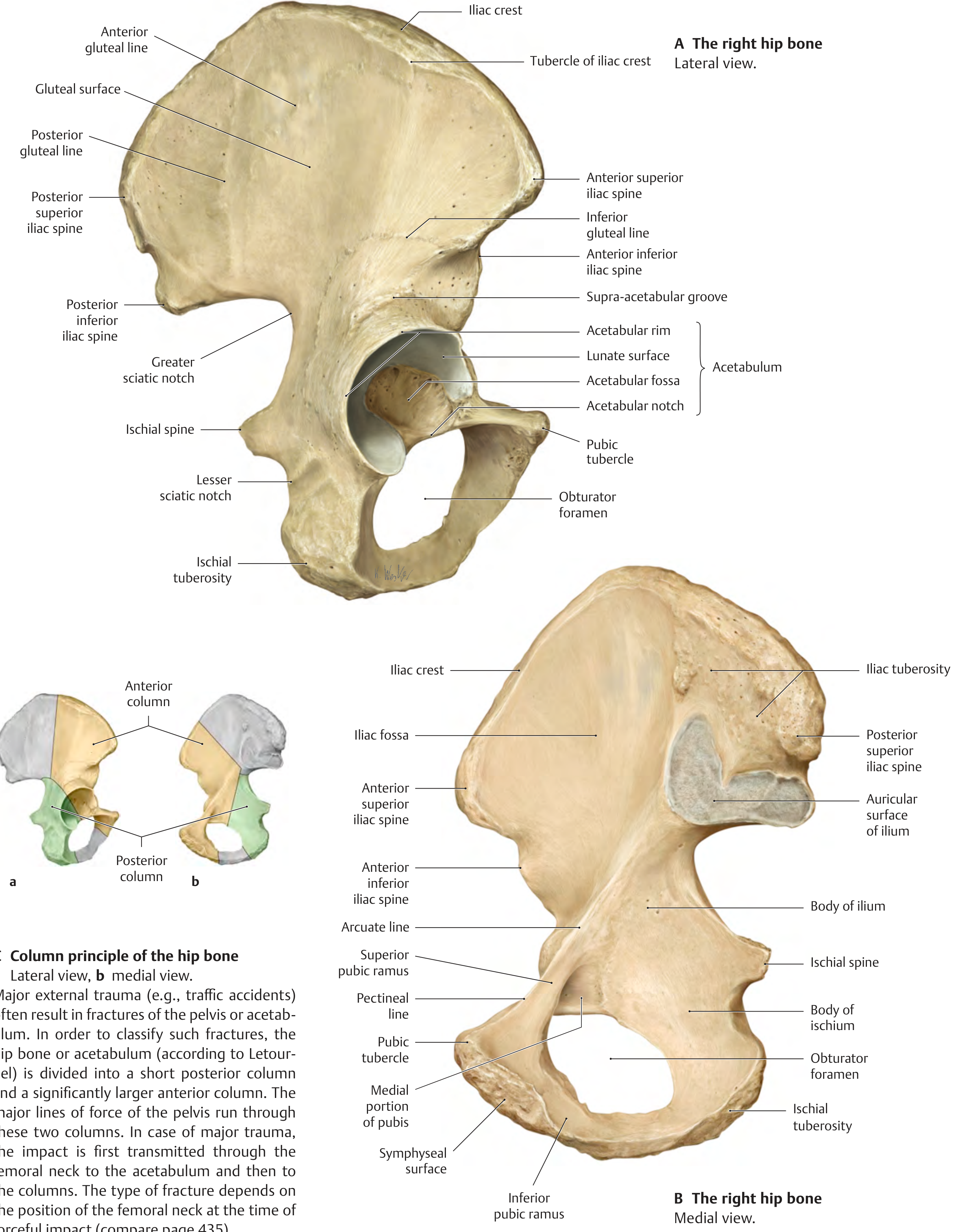
1.2 THE ILIUM
The ilium is the largest of the three parts, forming the superior and largest part of the hip bone.
Parts:
- Body of ilium - forms the upper 2/5 of the acetabulum
- Ala (wing) of ilium - the large fan-shaped plate above the body
Surfaces:
A. Gluteal (External/Lateral) Surface:
Contains three curved ridges - the gluteal lines - which divide the surface into areas for gluteal muscle attachments:
| Gluteal Line | Position | Muscle between it and acetabulum |
|---|---|---|
| Anterior gluteal line | Runs from iliac crest to greater sciatic notch | Gluteus medius (between anterior and posterior lines) |
| Posterior gluteal line | Short, near posterior end | Gluteus maximus (behind posterior line) |
| Inferior gluteal line | Just above acetabulum | Gluteus minimus (between anterior and inferior lines) |
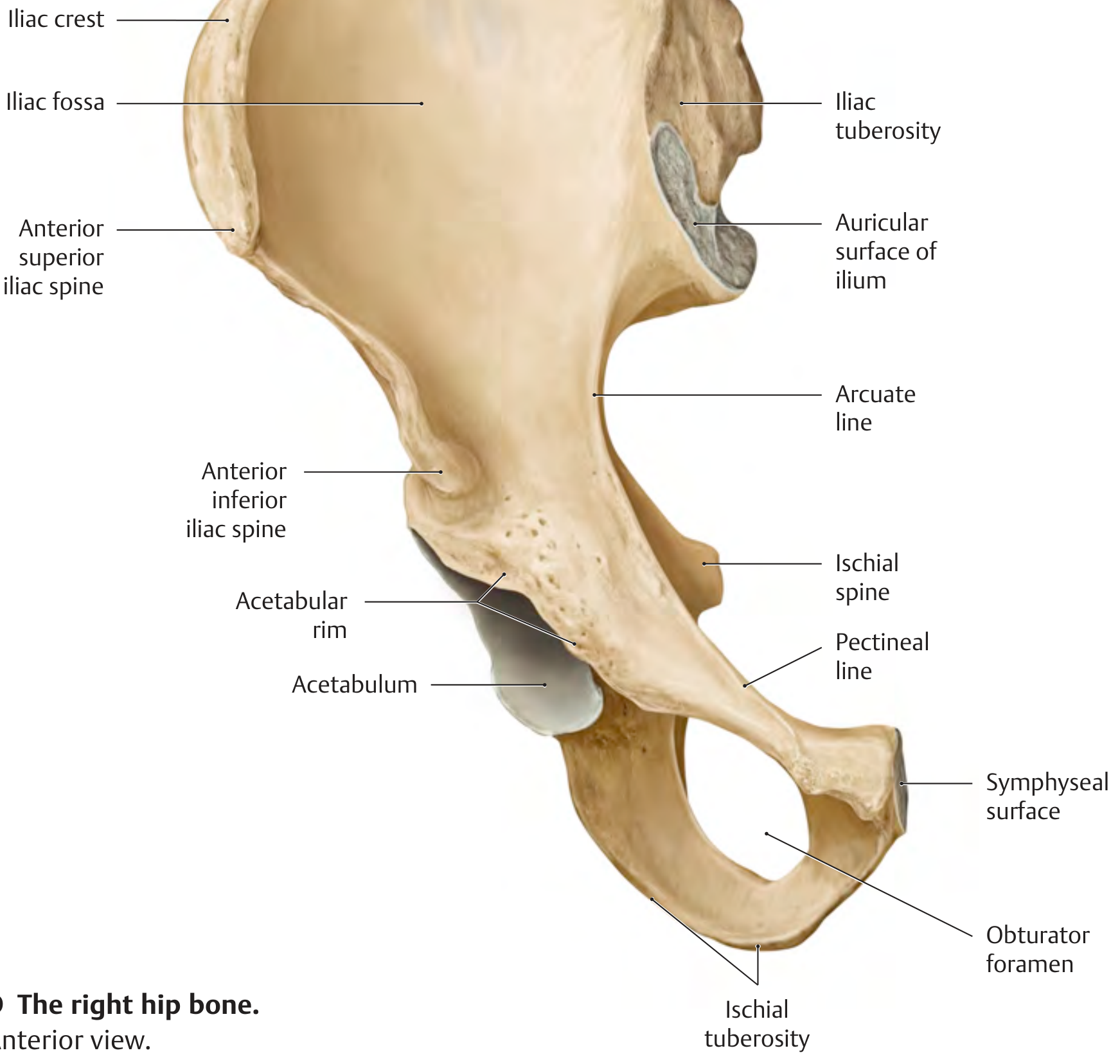
B. Iliac Fossa (Internal/Medial Surface):
- Large concave smooth area on the inner surface
- Gives origin to the iliacus muscle
- Separated from the true pelvis by the arcuate line
C. Auricular Surface + Iliac Tuberosity (Posterior Surface):
- Auricular surface - ear-shaped articular surface for articulation with the sacrum (sacroiliac joint)
- Iliac tuberosity - roughened area above auricular surface; attachment for the interosseous sacroiliac ligament
Iliac Crest:
- The thick curved superior border of the ala
- Extends from ASIS (Anterior Superior Iliac Spine) to PSIS (Posterior Superior Iliac Spine)
- Has an outer lip, inner lip, and intermediate zone
- Tubercle of the iliac crest - palpable bony projection approximately 5 cm posterior to the ASIS (on the outer lip)
- Important as a surface landmark - the highest point of the iliac crest is at the level of L4 vertebra (used for lumbar puncture)
Iliac Spines (4 in total):
| Spine | Location | Attachments / Clinical Significance |
|---|---|---|
| ASIS | Anterosuperior | Sartorius (origin), inguinal ligament (lateral end) - easily palpable |
| AIIS | Anteroinferior, below ASIS | Rectus femoris (straight head), iliofemoral ligament |
| PSIS | Posterosuperior | Sacrotuberous and posterior sacroiliac ligaments; corresponds to skin dimple of the back |
| PIIS | Posteroinferior | Posterior sacroiliac ligament |
1.3 THE ISCHIUM
The ischium forms the posteroinferior part of the hip bone.
Parts:
- Body of ischium - forms the posteroinferior 2/5 of the acetabulum
- Ramus of ischium (inferior ramus) - projects anteriorly to join the inferior pubic ramus, forming the ischiopubic ramus
Key Features:
Ischial Spine:
- Sharp bony projection from the posterior border of the body
- Separates the greater sciatic notch (above) from the lesser sciatic notch (below)
- Attachment: sacrospinous ligament; pudendal nerve passes around it
- Can be palpated per rectum / per vaginum - landmark for pudendal nerve block
Ischial Tuberosity:
- Large, rough, oval prominence on the posteroinferior aspect
- Bears the body's weight in sitting
- Attachments: hamstring muscles (semitendinosus, semimembranosus, long head of biceps femoris), adductor magnus (hamstring part), sacrotuberous ligament
- Palpable through buttock when hip is flexed
Greater Sciatic Notch:
- Between PIIS and ischial spine
- Converted to greater sciatic foramen by the sacrospinous ligament
- Transmits: piriformis muscle, sciatic nerve, superior and inferior gluteal vessels/nerves, pudendal vessels/nerve (enter and re-enter)
Lesser Sciatic Notch:
- Between ischial spine and ischial tuberosity
- Converted to lesser sciatic foramen by sacrospinous + sacrotuberous ligaments
- Transmits: obturator internus tendon, pudendal nerve and vessels (re-enter pelvis)
Obturator Foramen:
- Large oval opening in the lower part of the hip bone, bounded by ischium and pubis
- Mostly closed by the obturator membrane, except superiorly where the obturator canal transmits the obturator nerve and vessels
1.4 THE PUBIS
The pubis is the anteroinferior part of the hip bone.
Parts:
- Body of pubis - forms the anteromedial part; medial surface = symphyseal surface; contributes 1/5 of acetabulum
- Superior pubic ramus - projects laterally from the body toward the acetabulum
- Inferior pubic ramus - projects downward and backward to join the ischial ramus
Key Features:
Pubic Tubercle:
- Small rounded projection on the superior aspect of the body
- Attachment for medial end of the inguinal ligament
- Key landmark for identifying the inguinal ligament and femoral canal
Pectineal Line (Pecten Pubis):
- Sharp ridge on the superior pubic ramus
- Part of the linea terminalis (pelvic brim)
- Attachment: pectineus muscle, pectineal ligament (Cooper's ligament)
Pubic Crest:
- Medial thickening of the superior body surface, between the two pubic tubercles (across the midline)
Symphyseal Surface:
- Oval, rough, vertical medial face of pubic body
- Articulates with the opposite side at the pubic symphysis (secondary cartilaginous joint / amphiarthrosis)
1.5 THE ACETABULUM
The acetabulum is a cup-shaped socket on the lateral surface of the hip bone. It is formed by all three bones meeting (ilium 2/5 + ischium 2/5 + pubis 1/5).
Parts:
| Part | Description |
|---|---|
| Lunate surface | Horseshoe-shaped articular cartilage-covered surface; articulates with head of femur |
| Acetabular fossa | Central non-articular area; has fatty tissue (Haversian gland/fat pad) and attachment of ligament of head of femur |
| Acetabular rim | Peripheral bony edge of acetabulum |
| Acetabular notch | Inferior gap in the rim; bridged by the transverse acetabular ligament |
The acetabulum faces laterally, inferiorly, and anteriorly (approximately 17° anterior inclination per THIEME Atlas).
The acetabular labrum (fibrocartilaginous rim) deepens the socket, increasing its depth from ~40% to ~70% coverage of the femoral head.
1.6 SEX DIFFERENCES IN THE HIP BONE (Important for MBBS/Forensics)
| Feature | Male | Female |
|---|---|---|
| Subpubic angle | Narrow (<70°) | Wide (>80°, "V vs. U") |
| Obturator foramen | Large, oval | Smaller, triangular |
| Acetabulum | Large, faces laterally | Smaller, faces more anterolaterally |
| Iliac crest | Higher, more inclined | Broader, more flared |
| Greater sciatic notch | Narrow | Wide |
| Sacrum | Narrow, long | Wide, short |
| Pelvic inlet | Heart-shaped | Oval/round |
PART 2: THE FEMUR
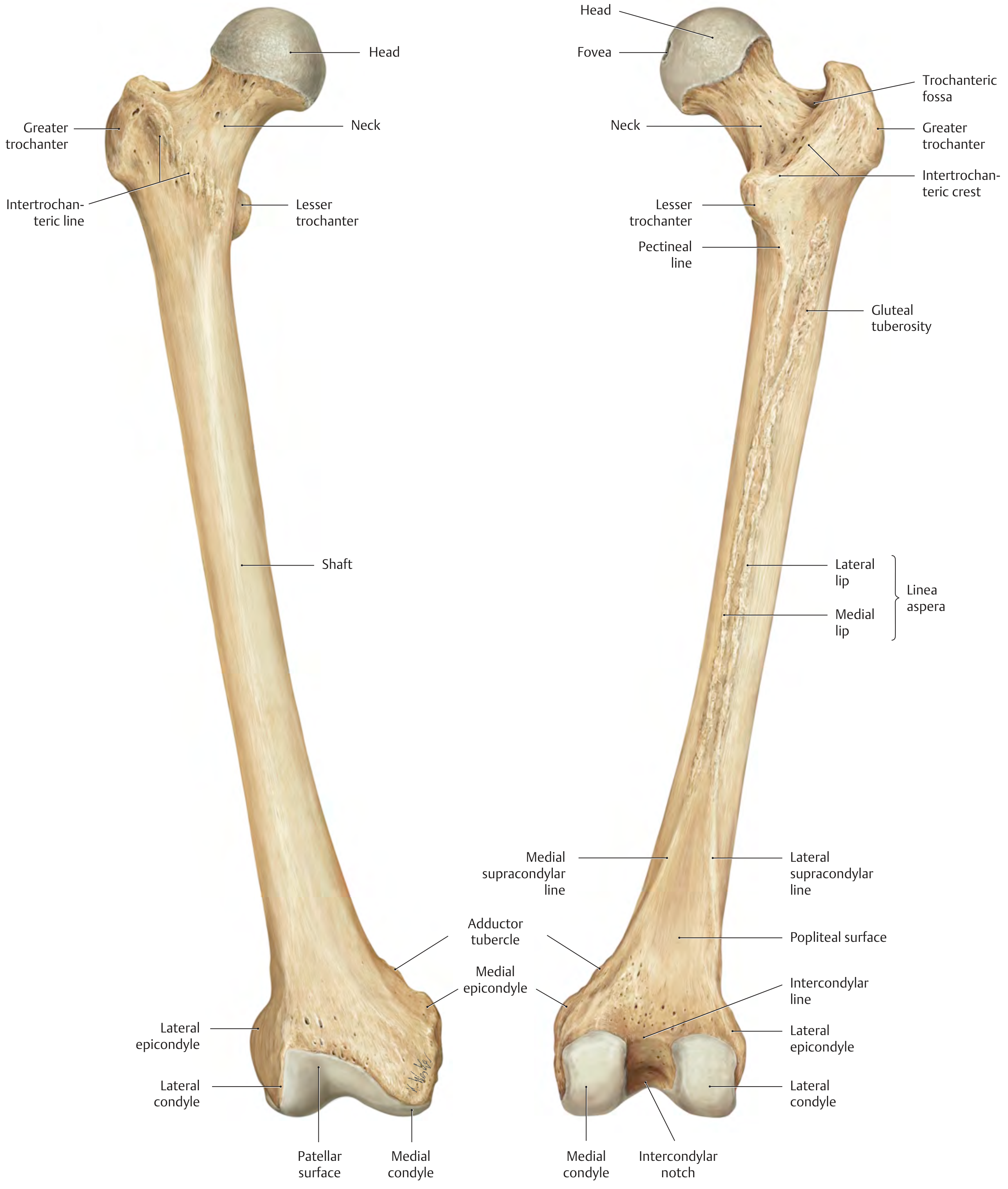
2.1 Overview
The femur is the longest, strongest, and heaviest bone in the body. It is the bone of the thigh and articulates:
- Proximally with the acetabulum of the hip bone (hip joint)
- Distally with the tibia and patella (knee joint)
The shaft of the femur is obliquely oriented, descending from lateral to medial at 7 degrees from the vertical (Gray's Anatomy for Students). This oblique course brings the knee close to the midline beneath the body's center of gravity.
The femur consists of:
- Proximal end - head, neck, greater and lesser trochanters
- Shaft (diaphysis)
- Distal end - medial and lateral condyles, epicondyles, patellar surface
2.2 PROXIMAL FEMUR
Head of the Femur:
- Spherical, covered with articular cartilage (except at the fovea)
- Articulates with the acetabulum
- Fovea capitis (fovea of the head): Non-articular pit on the medial surface of the head; attachment for the ligamentum teres (ligament of the head) - contains the artery of the ligamentum teres (branch of obturator artery; small and variable in adults)
Neck of the Femur:
-
Cylindrical strut connecting head to shaft
-
Projects superomedially from the shaft
-
Angle of inclination (CCD angle / Femoral Neck Angle):
- Newborn: ~150°
- Adult: ~126° (THIEME Atlas) / ~125° (Gray's)
- If >126° = Coxa valga (neck more vertical, relative leg lengthening)
- If <126° = Coxa vara (neck more horizontal, relative leg shortening)
-
Angle of anteversion (torsion angle):
- The neck is twisted forward relative to the condylar axis
- Newborn: 30-40°; Adult: ~12°
- If increased = coxa anteverta → toeing-in gait
- If decreased/reversed = coxa retroverta → toeing-out gait
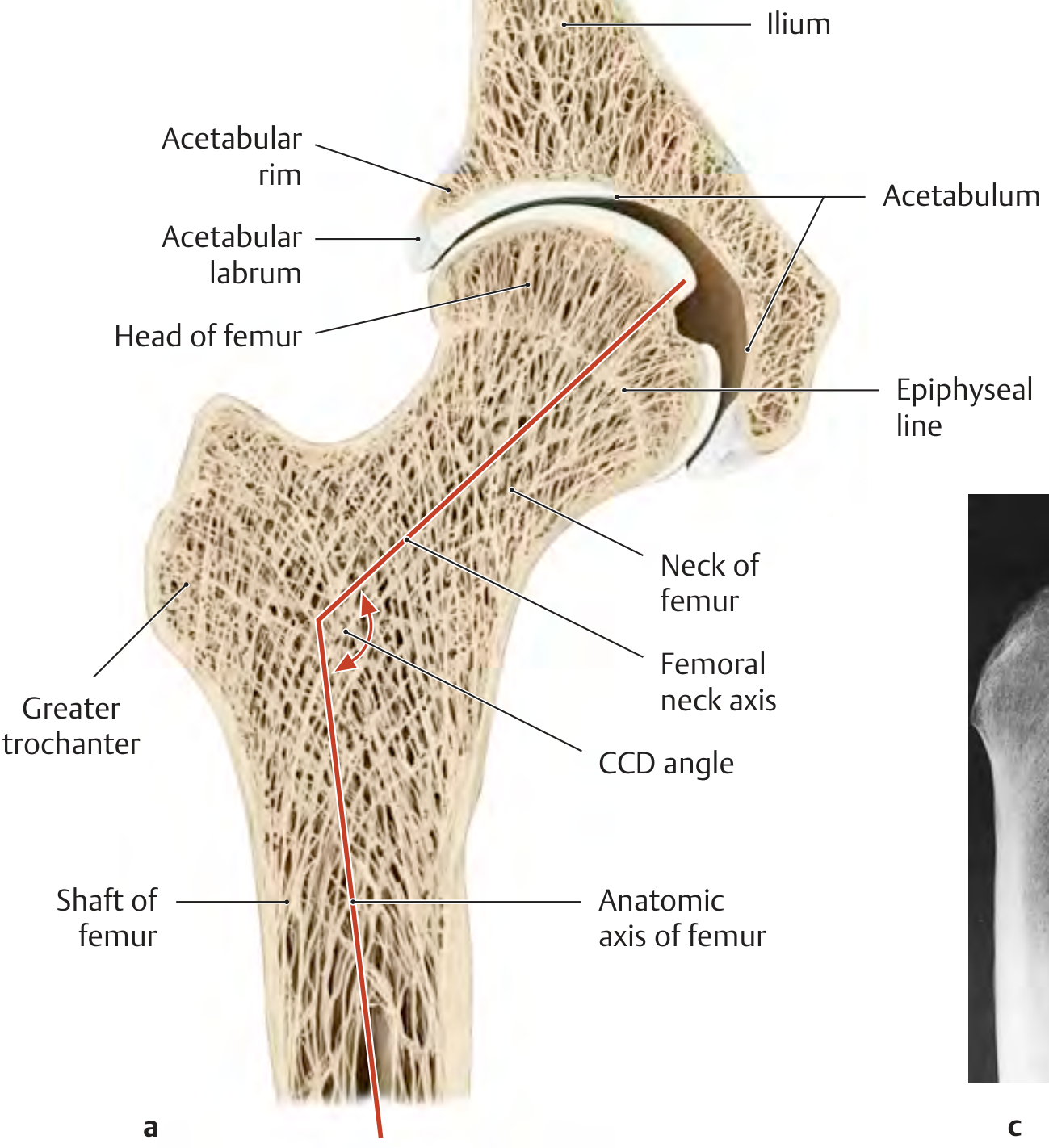
2.3 TROCHANTERS
Greater Trochanter:
- Large quadrilateral bony projection extending superiorly from the junction of the neck and shaft, laterally
- Trochanteric fossa: Deep depression on the medial surface of the greater trochanter; where obturator externus inserts
- Muscle attachments (lateral surface):
- Anterior ridge: Gluteus minimus
- Posterior ridge: Gluteus medius
- Superior margin (medial to fossa): Obturator internus + gemelli
- Superior-posterior margin: Piriformis
- The greater trochanter is palpable in the lateral thigh (important surface landmark)
Lesser Trochanter:
- Smaller, cone-shaped projection from the posteromedial aspect at the junction of neck and shaft
- Attachment: combined tendon of psoas major + iliacus (iliopsoas)
Connecting Ridges:
- Intertrochanteric line (anterior surface): Runs between the two trochanters on the anterior aspect; marks the anterior limit of the femoral neck and capsular attachment line; attachment for the iliofemoral ligament (superior band)
- Intertrochanteric crest (posterior surface): Thick rounded ridge on the posterior aspect; bears the quadrate tubercle at its midpoint (attachment for quadratus femoris)
2.4 SHAFT OF THE FEMUR
The shaft has an oblique course and is bowed slightly anteriorly.
Cross-Section (middle third):
The shaft is triangular in cross section with:
- Anterior surface
- Medial (posteromedial) surface
- Lateral (posterolateral) surface
- Medial border (rounded)
- Lateral border (rounded)
- Posterior border = Linea aspera (rough crest)
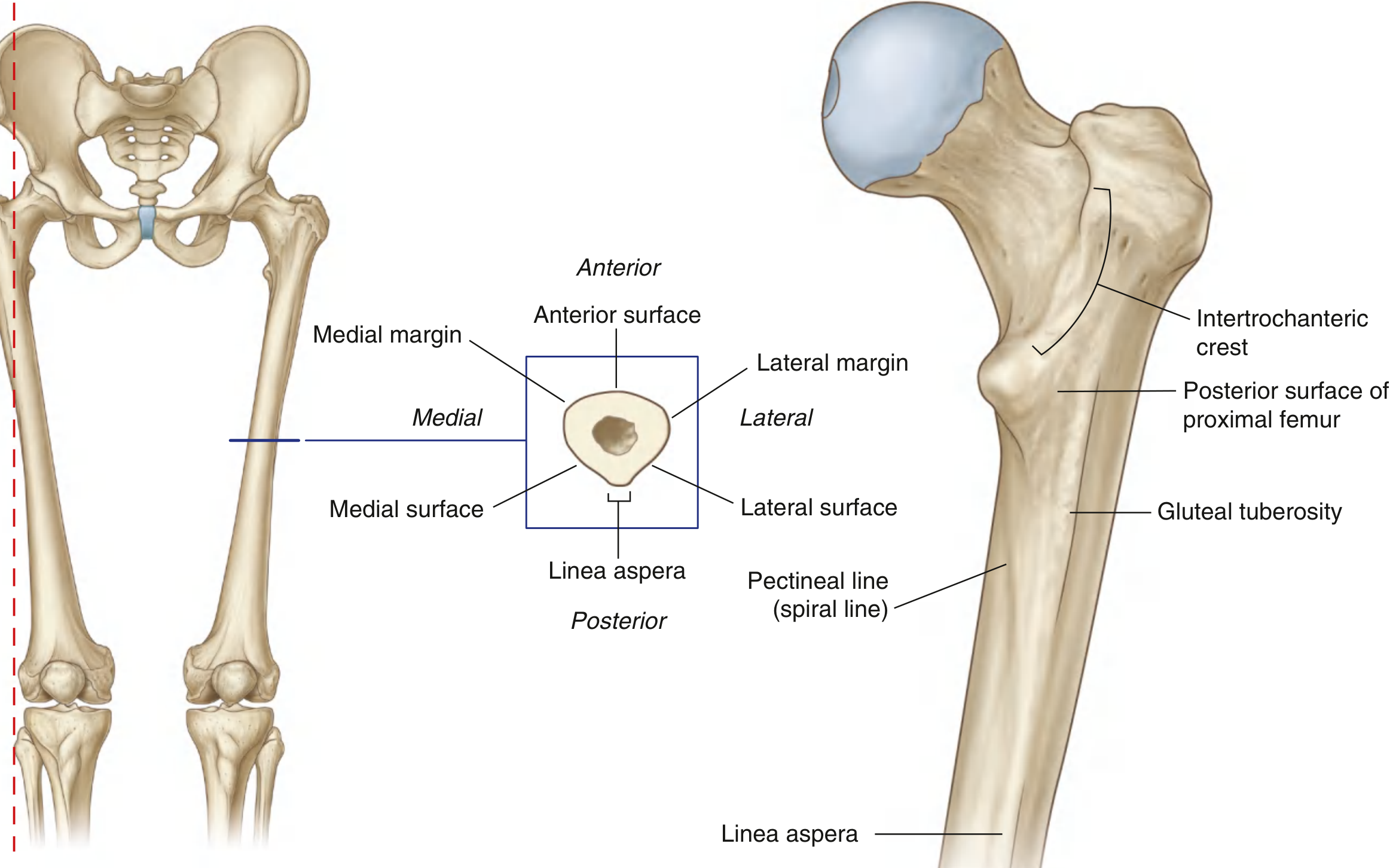
Linea Aspera:
- Major muscular ridge on the posterior surface of the middle third
- Has a medial lip and lateral lip
- Muscle attachments on linea aspera (a favorite MBBS exam question):
| Muscle | Attachment Site |
|---|---|
| Vastus medialis | Medial lip |
| Vastus lateralis | Lateral lip |
| Adductor longus | Middle (medial lip) |
| Adductor brevis | Upper medial lip |
| Adductor magnus | Both lips |
| Short head of biceps femoris | Lateral lip |
| Pectineus | Pectineal line (proximal continuation) |
| Gluteus maximus | Gluteal tuberosity (lateral proximal continuation) |
Proximal continuations of linea aspera:
- Pectineal line (spiral line): Medial lip curves anteriorly, passing under the lesser trochanter, joining the intertrochanteric line
- Gluteal tuberosity: Lateral lip curves to the base of the greater trochanter; gluteus maximus attaches here (sometimes a 3rd trochanter is present)
Distal continuations of linea aspera:
- Linea aspera splits into medial supracondylar line and lateral supracondylar line, enclosing the popliteal surface (floor of popliteal fossa)
- Medial supracondylar line terminates at the adductor tubercle on the medial condyle
- Adductor tubercle = attachment for adductor magnus (adductor part)
2.5 DISTAL FEMUR
The distal end consists of two large condyles that articulate with the tibia and patella.
Medial and Lateral Condyles:
- Large, rounded condyles, broader posteriorly and becoming flatter inferiorly
- Articulate with the tibial plateau inferiorly
- Articulate with the patella anteriorly via the patellar surface (femoral trochlea) - a V-shaped groove; lateral wall is larger and steeper
Intercondylar Fossa (Notch):
- Deep notch separating the condyles posteriorly
- Contains the cruciate ligaments:
- Anterior cruciate ligament (ACL): Attaches to the medial surface of the lateral condyle (posterosuperior oval facet)
- Posterior cruciate ligament (PCL): Attaches to the lateral surface of the medial condyle (large oval facet, inferior half)
Epicondyles:
- Non-articular bony elevations on the outer surfaces of condyles
- Medial epicondyle: Attachment for medial collateral ligament of knee; the adductor tubercle lies just above it
- Lateral epicondyle: Attachment for lateral collateral ligament of knee; has two facets posterior to it for the popliteus and lateral head of gastrocnemius
2.6 IMPORTANT ANGLES (MUST KNOW FOR EXAMS)
| Angle | Normal Value | Clinical Significance |
|---|---|---|
| Femoral neck angle (CCD/angle of inclination) | ~126° adult | Coxa valga >135°; Coxa vara <120° |
| Angle of anteversion (torsion) | ~12° adult | Coxa anteverta (toeing-in); coxa retroverta (toeing-out) |
| Shaft obliquity | 7° from vertical | Medial angulation of shaft; knee at midline |
2.7 BLOOD SUPPLY TO THE HEAD OF FEMUR (Extremely Important Clinically)
Three sources (from Gray's Anatomy for Students):
- Retinacular vessels (primary supply in adults): Branches of the medial and lateral circumflex femoral arteries form an arterial ring at the base of the neck; from here, vessels run along the neck deep to the capsular periosteum (retinacula) and supply the head
- Medial circumflex femoral artery supplies most of the head
- Artery of the ligamentum teres (branch of obturator artery): Small and variable; significant in children, attenuated in adults
- Medullary artery via nutrient artery: Contributes in youth; in older age, medullary cavity undergoes fatty replacement (reduced supply)
Clinical Pearl: In subcapital fractures of the neck of femur, the retinacular vessels are disrupted, leading to avascular necrosis (AVN) of the femoral head. This is why hemiarthroplasty (not internal fixation) is preferred for displaced subcapital fractures in the elderly.
Subcapital > Transcervical > Basicervical - risk of AVN decreases as fracture moves distally.
PART 3: CLINICAL APPLIED ANATOMY (MBBS Must-Know)
3.1 Fracture of the Neck of Femur
Classic presentation (Gray's Anatomy case):
- Elderly woman, fall at home
- Right leg shorter and externally rotated
- Displaced fracture on X-ray
Why external rotation?
- Psoas major attaches to the lesser trochanter; normally its fulcrum is the femoral head in the acetabulum
- When the neck fractures, psoas overriding action pulls the femur proximally and into external rotation
- Spasm of adductors exacerbates external rotation
Fracture types by location:
- Subcapital: Across head-neck junction - highest AVN risk
- Transcervical: Through midportion of neck
- Basicervical: Across base of neck - lowest AVN risk
Management:
- Elderly with displaced subcapital fracture → Hemiarthroplasty (femoral head removed, prosthesis inserted)
- Young patients or undisplaced fractures → Internal fixation (cannulated screws / dynamic hip screw)
- Intertrochanteric fractures → DHS (dynamic hip screw), retinacular vessels not at risk
3.2 Coxa Valga vs. Coxa Vara
| Coxa Valga | Coxa Vara | |
|---|---|---|
| CCD angle | >135° | <120° |
| Neck position | More vertical | More horizontal |
| Greater trochanter | Lower than head | Elevated (above head level) |
| Relative leg length | Longer | Shorter |
| Risk | Hip instability | Limping gait (Trendelenburg) |
| Cause | Rickets, Paget's (vara); paralysis (valga) | Rickets, Paget's, congenital |
3.3 Pelvic Brim (Linea Terminalis)
From posterior to anterior:
- Sacral promontory → sacral ala → sacroiliac joint → arcuate line of ilium → pectineal line → pubic crest → pubic symphysis
This line separates the greater (false) pelvis from the lesser (true) pelvis.
3.4 Osseofascial Compartments & Nerve Injuries
- ASIS avulsion fracture: Young athletes - sartorius pulls off the ASIS
- AIIS avulsion fracture: Rectus femoris pulls off AIIS in kicking sports
- Ischial tuberosity avulsion: Hamstrings pull off in sprinters (gymnasts doing splits)
- Meralgia paresthetica: Lateral femoral cutaneous nerve compressed at ASIS/inguinal ligament - burning pain/numbness on anterolateral thigh
3.5 Trabecular Pattern of Femoral Head (THIEME Atlas)
The femoral neck contains two main trabecular systems:
- Compression trabeculae: Run from the head downward to the medial cortex - bear compressive loads
- Tension trabeculae: Run from the head to the lateral cortex - bear tensile loads
- The Ward's triangle = area of relative weakness between the two trabecular systems in the neck; first site of fracture in osteoporosis
PART 4: PELVIC GIRDLE - ARTICULATIONS SUMMARY
| Joint | Type | Movements |
|---|---|---|
| Pubic symphysis | Secondary cartilaginous (fibrocartilaginous disc) | Minimal; slight widening in pregnancy |
| Sacroiliac joint | Synovial (anterior); fibrous (posterior) | Nutation/counternutation; minimal movement |
| Hip joint | Ball and socket synovial | Flexion, extension, abduction, adduction, medial/lateral rotation, circumduction |
QUICK REVISION TABLE: KEY Attachments at a Glance
Hip Bone - Key Muscle Origins
| Structure | Muscle(s) Attached |
|---|---|
| Outer lip of iliac crest | Tensor fascia lata, gluteus maximus |
| Intermediate zone, iliac crest | External oblique |
| Inner lip, iliac crest | Internal oblique, transversus abdominis |
| Iliac fossa | Iliacus |
| Gluteal surface (between lines) | Gluteus maximus (behind post. line), medius (between ant. & post.), minimus (between ant. & inf.) |
| ASIS | Sartorius (origin), tensor fascia lata |
| AIIS | Rectus femoris (straight head), iliofemoral lig. |
| Ischial tuberosity | Semitendinosus, semimembranosus, long head biceps, adductor magnus |
| Ischial spine | Gemellus superior |
| Body of ischium | Gemellus inferior |
| Pubic tubercle | Inguinal ligament (medial end) |
| Pectineal line | Pectineus |
| Superior pubic ramus | Obturator externus (external surface) |
| Obturator membrane | Obturator internus (internal surface), obturator externus (external surface) |
Femur - Key Muscle Insertions/Origins
| Structure | Muscle |
|---|---|
| Greater trochanter (lateral ant.) | Gluteus minimus (insertion) |
| Greater trochanter (lateral post.) | Gluteus medius (insertion) |
| Trochanteric fossa | Obturator externus (insertion) |
| Superior greater trochanter | Obturator internus + gemelli (insertion), piriformis |
| Lesser trochanter | Iliopsoas (insertion) |
| Intertrochanteric line | Iliofemoral ligament |
| Gluteal tuberosity | Gluteus maximus (insertion) |
| Linea aspera (medial lip) | Vastus medialis, adductor longus, adductor brevis, adductor magnus |
| Linea aspera (lateral lip) | Vastus lateralis, short head of biceps femoris |
| Adductor tubercle | Adductor magnus (adductor part) |
| Medial epicondyle | Medial collateral ligament |
| Lateral epicondyle | Lateral collateral ligament |
PART 5: OSSIFICATION (Important for MBBS Exams - BD Chaurasia/KLM)
Hip Bone Ossification:
- Ilium: Primary center appears at 8th week of fetal life
- Ischium: Primary center appears at 4th month of fetal life
- Pubis: Primary center appears at 4-5th month of fetal life
- The three centers fuse at the acetabulum (triradiate cartilage) between 14-16 years
- Secondary centers appear at iliac crest, ASIS, ischial tuberosity, pubic tubercle, etc. - fuse by 25 years
Femur Ossification:
| Center | Appearance | Fusion |
|---|---|---|
| Shaft (primary) | 7th week of fetal life | - |
| Lower end | 9th month of fetal life (just before birth) - always present at birth | 18-20 years |
| Upper end (head) | 6-12 months postnatal | 18 years |
| Greater trochanter | 4th year | 18 years |
| Lesser trochanter | 13-14 years | 18 years |
Medicolegal Note (BD Chaurasia): The distal femoral epiphysis is visible on X-ray at birth (36 weeks+ gestation). Its presence confirms that the fetus was viable (full-term). This is used in medicolegal examination of newborns.
SUMMARY MNEMONICS
Muscles inserted on greater trochanter (lateral-to-medial, superior-to-inferior):
"P-OI-Gem-Min-Med" = Piriformis, Obturator Internus + Gemelli, Gluteus Minimus, Gluteus Medius
Linea aspera attachments (medial lip, lateral to medial, from above down):
Pectineus → Adductor brevis → Adductor longus → Adductor magnus (medial lip); Vastus lateralis → Biceps short head → Vastus medialis (lateral then medial lips)
Contents of greater sciatic foramen:
"P-Sup G-Sciatic-Inf G-P-PN-I" = Piriformis, Superior gluteal, Sciatic nerve, Inferior gluteal, Posterior cutaneous of thigh, Pudendal nerve (enters), Internal pudendal vessels
Sources: Gray's Anatomy for Students (4th Ed.), THIEME Atlas of Anatomy - General Anatomy & Musculoskeletal System (3rd Ed.), Netter's Atlas of Human Anatomy (7th Ed.), BD Chaurasia's Human Anatomy Vol.2 (Lower Limb), KLM (Kulkarni) Anatomy
This is a shared conversation. Sign in to Orris to start your own chat.