Acromegaly and gigantism features
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have excellent content and images from multiple textbooks. Let me compile the full answer.
Acromegaly and Gigantism: Clinical Features
Key Distinction
Both conditions result from excess Growth Hormone (GH) secretion, almost always due to a somatotroph (GH-secreting) pituitary adenoma. The timing relative to epiphyseal plate closure determines the syndrome:
| Gigantism | Acromegaly | |
|---|---|---|
| Onset | Before puberty (open epiphyses) | After puberty (closed epiphyses) |
| Linear growth | Extraordinary height (proportionate) | No increase in height |
| Soft-tissue/bony changes | Present + height | Present without height |
Etiology
Cause of GH excess (Harrison's 22e):
| Source | Prevalence |
|---|---|
| Pituitary adenoma (all types) | ~98% |
| - Densely/sparsely granulated GH cell adenoma | 60% |
| - Mixed GH + PRL cell adenoma | 25% |
| - Mammosomatotrope cell adenoma | 10% |
| Extrapituitary tumor (pancreatic islet, lymphoma) | <1% |
| Excess GHRH (central: hypothalamic; peripheral: carcinoid, small-cell lung) | <1% |
Associated syndromes include MEN-1 and McCune-Albright syndrome. GH co-secretes PRL in ~20-40% of cases (may cause hypogonadism and galactorrhea).
Gigantism - Features
- Occurs when GH excess arises before epiphyseal fusion (childhood/adolescence)
- The individual grows to extraordinary height - proportionate overall, but later develops acromegalic changes
- If untreated, features of acromegaly superimpose as the patient ages
- Increased length of long bones, enlarged head and feet (as shown below)
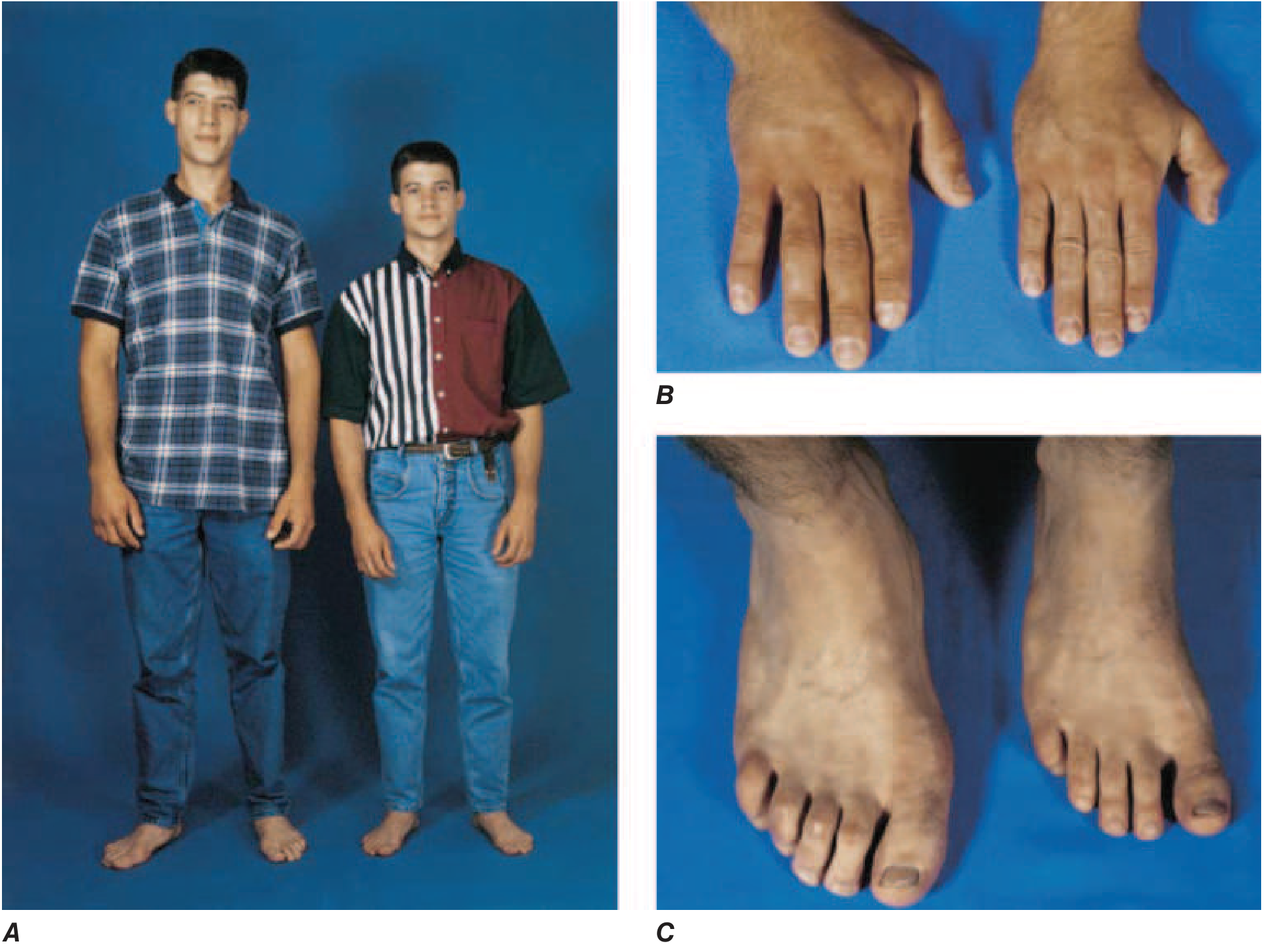
FIGURE: A 22-year-old man with gigantism (left) beside his identical twin (right). Note the increased height, prognathism, enlarged head, and enlarged feet. Clinical divergence began at age ~13. (Harrison's 22e, Fig. 392-7)
Acromegaly - Clinical Features
Onset is insidious (average delay of 7-10 years between onset and diagnosis). Features arise from GH/IGF-1 excess and local tumor mass effects.
1. Facial / Head Features
- Coarsening of facial features (most characteristic)
- Prognathism - jaw protrusion, leading to interdental separation and underbite
- Frontal bossing - prominent supraorbital ridges / brow protrusion
- Macroglossia - enlarged tongue
- Enlarged nose, lips, and ears
- Deepening of the voice (enlargement of larynx and sinuses)

Lateral profile of a patient with acromegaly showing coarse facial features (Scott-Brown's ENT, Fig. 82.3c)
2. Extremities
- Enlarged hands and feet - "spade-like" or "shovel-like" hands; patients note increasing ring/glove/shoe size
- Soft-tissue swelling of the hands and feet

Enlarged, broadened hands ("spade hands") in acromegaly (Scott-Brown's ENT, Fig. 82.3d)
3. Musculoskeletal
- Degenerative osteoarthritis (vertebral changes, joint pain - arthralgia)
- Myopathy - proximal muscle weakness
- Kyphosis / vertebral changes
- Carpal tunnel syndrome (median nerve compression from soft-tissue swelling)
- Hearing loss (from bony changes)
4. Skin and Soft Tissue
- Excess sweating (hyperhidrosis) - one of the most common symptoms
- Hirsutism
- Oily skin, acne-like lesions
- Acanthosis nigricans
- Skin tags (acrochordons)
5. Metabolic
- Insulin resistance / Diabetes mellitus - GH is diabetogenic (anti-insulin effect); ~25% have abnormal glucose tolerance
- Hypercalciuria (GH stimulates renal 1α-hydroxylase → increased vitamin D activation → increased calcium absorption)
- Hyperprolactinemia in ~30% (co-secretion) - may cause galactorrhea in ~4% and hypogonadism
6. Cardiovascular (most common cause of death)
- Hypertension
- Cardiomegaly / cardiomyopathy
- Arrhythmias
- Congestive cardiac failure
- Ischaemic heart disease and cerebrovascular disease
- Premature cardiovascular disease is the leading cause of death
7. Respiratory
- Obstructive sleep apnoea (OSA) - common; from macroglossia, soft-tissue hypertrophy, and jaw changes
8. Gastrointestinal
- Colonic polyps (increased risk of colorectal neoplasia) - screening colonoscopy required at diagnosis
- Multinodular thyroid enlargement
9. Neurological / Local Tumor Effects
- Headaches (pituitary expansion)
- Visual field defects - bitemporal hemianopia from optic chiasm compression by macroadenoma
- Polyneuropathy (rare; described by Adams & Victor)
Summary Table (Scott-Brown's ENT, Table 84.5)
| Domain | Symptoms | Signs | Complications |
|---|---|---|---|
| Musculoskeletal | Arthralgia, increased shoe/hand size | Enlarged hands/feet, myopathy, osteoarthritis, prognathism, macroglossia | Carpal tunnel syndrome, hearing loss |
| Cardiovascular | - | Hypertension, cardiomyopathy | Ischaemic heart disease, CCF, cerebrovascular disease |
| Respiratory | - | OSA signs | Obstructive sleep apnoea |
| Metabolic | Sweating, headaches | Coarse features, hirsutism | Diabetes mellitus, metabolic syndrome |
| GI | - | - | Colonic polyps |
| Visual | - | Visual field defects | Blindness (if untreated) |
Diagnosis
- IGF-1 level (age/sex matched) - elevated; best screening test
- Oral glucose tolerance test (OGTT): GH fails to suppress to <1 μg/L after glucose load - confirmatory test
- MRI pituitary: demonstrates adenoma in 98% of cases
- Screen for associated conditions: diabetes, hypertension, OSA, colonic polyps, thyroid enlargement, cardiovascular disease
Treatment Overview
- Surgery: Transsphenoidal resection (first-line for most patients); remission ~70% for microadenomas, <50% for macroadenomas
- Somatostatin receptor ligands (SRLs): Octreotide, lanreotide - normalize GH/IGF-1 in ~50%
- GH receptor antagonist: Pegvisomant - for refractory cases
- Radiotherapy: Reserved for aggressive tumors not responding to surgery/medical therapy (slow response, 5-15 years; risk of hypopituitarism)
Sources: Harrison's Principles of Internal Medicine 22e; Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 1; Ganong's Review of Medical Physiology 26e; Tietz Textbook of Laboratory Medicine 7e
Gigantism features
Your credits are exhausted. You can purchase a top-up or subscribe to a plan to continue using Orris. If you're already subscribed, your daily credits will reset tomorrow.
Create a comparison chart: gigantism vs acromegaly
Your credits are exhausted. You can purchase a top-up or subscribe to a plan to continue using Orris. If you're already subscribed, your daily credits will reset tomorrow.
This is a shared conversation. Sign in to Orris to start your own chat.