Tell me in detail about nasal septum and littles area
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Finding Sources
Reading File
Reading File
I now have comprehensive information from multiple authoritative textbooks. Let me compile the full, detailed answer.
Nasal Septum and Little's Area
1. Overview and Functions
The nasal septum is the midline partition that divides the nasal cavity into two distinct chambers. Its key functions include:
- Separating the two nasal airways
- Providing support to the nasal dorsum
- Maintaining the shape of the columella and nasal tip
- Forming part of the nasal valves (internal and external)
- Supporting humidification and filtration of inspired air
Deviation or deformity of the septum can impair nasal airflow, cause olfactory disturbance, predispose to sinusitis, and produce cosmetic deformity. - Scott-Brown's Otorhinolaryngology, p. 1014; Cummings Otolaryngology, p. 565
2. Structural Components
The nasal septum consists of three portions: bony, cartilaginous, and membranous.
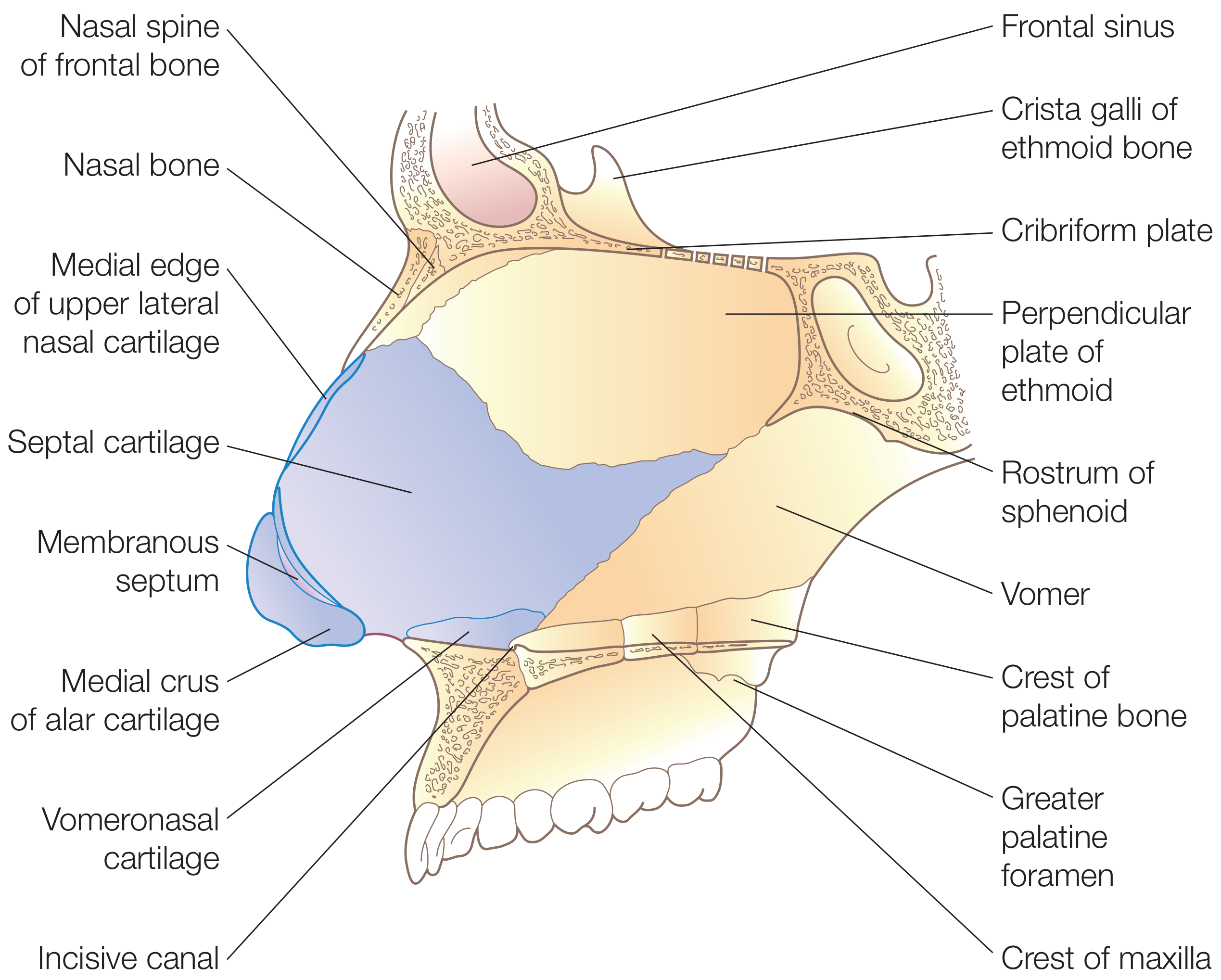
Figure: Cartilaginous and bony components of the nasal septum (Scott-Brown's Otorhinolaryngology)
A. Bony Portion
| Bone | Location/Contribution |
|---|---|
| Perpendicular plate of ethmoid | Upper one-third of the septum; continuous superiorly with the cribriform plate and crista galli |
| Vomer | Posterior and inferior septum; its two alae articulate with the sphenoid rostrum, creating vomerovaginal canals (transmit pharyngeal branches of maxillary artery) |
| Maxillary crest | Inferior border |
| Palatine bone crest | Posterior inferior border |
- The perpendicular plate articulates: superiorly with the cribriform plate, posteriorly with the sphenoid crest, posteroinferiorly with the vomer, and anteroinferiorly with the septal cartilage.
- The posterior free edge of the vomer forms the posterior free edge of the septum.
B. Cartilaginous Portion
- Formed by the quadrilateral (septal) cartilage, a large four-sided hyaline cartilage
- Bound to the nasal bones, perpendicular plate of ethmoid, and vomer by collagenous fibers
- Continuous with the upper lateral cartilages at the bridge of the nose (forming the internal nasal valve at this junction)
- Posterior projection = the septal tail (sphenoidal process), which extends between the vomer and perpendicular plate - useful as a cartilage harvest site in revision rhinoplasty
- Inferior attachment to the maxillary nasal crest is via loose connective tissue, forming a pseudarthrosis that allows mobility and reduces fracture risk from trauma
C. Membranous Septum
- A small segment of connective tissue between the caudal edge of septal cartilage and the columella
- No skeletal component
3. Nasal Septal Swell Body
A widened region of the anterior nasal septum located anterior to the middle turbinate at the level of the internal nasal valve. Histologically it contains abundant venous sinusoids (fewer glands than adjacent mucosa), giving it the capacity to modulate nasal airflow in a manner similar to the inferior turbinate. - Scott-Brown's, p. 1014
4. Blood Supply of the Nasal Septum
Both the internal and external carotid arteries contribute. This dual supply is clinically important.
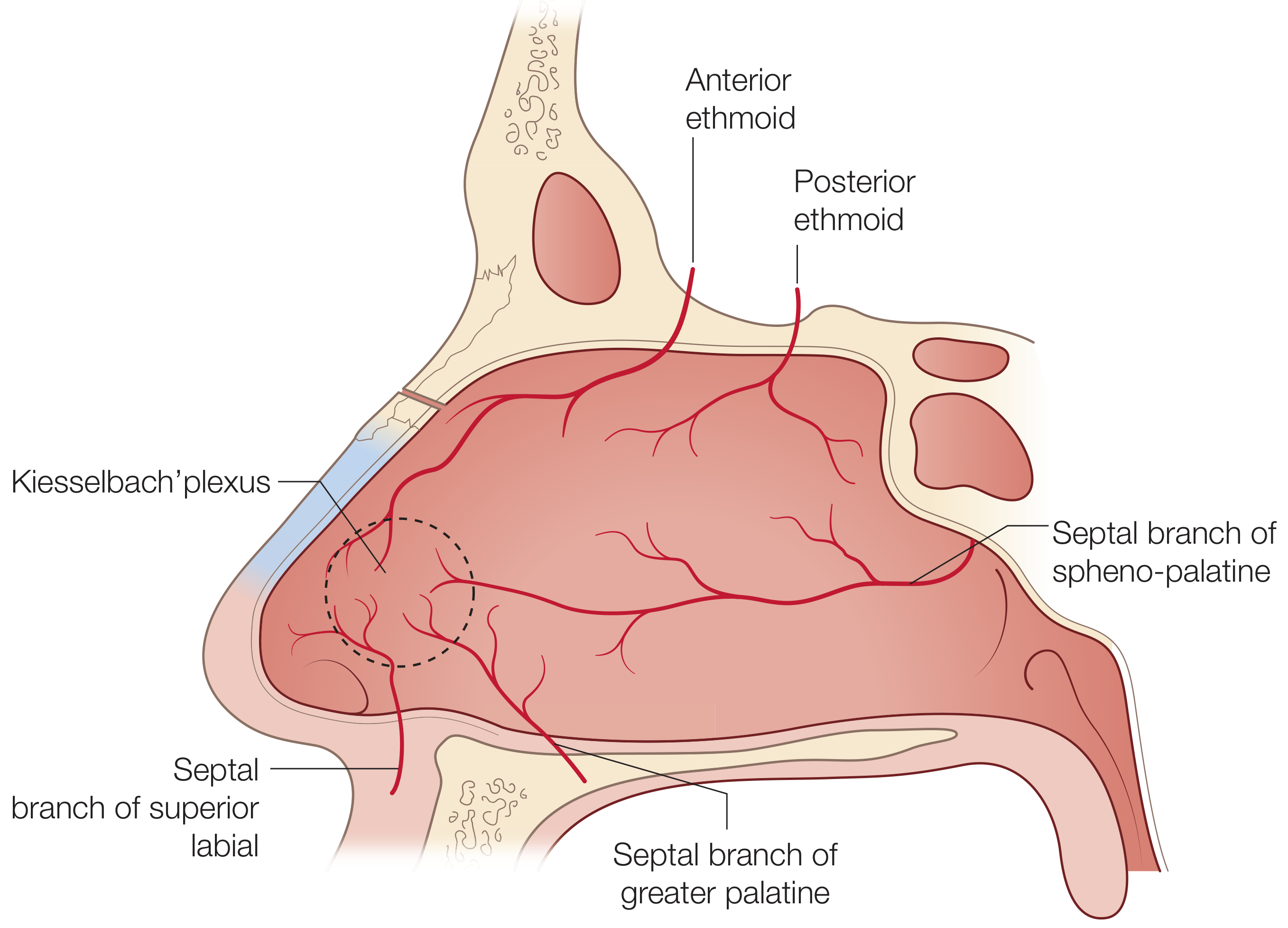
Figure: Vascular supply of the nasal septum with Kiesselbach's plexus (Scott-Brown's, p. 1015)
From the External Carotid Artery (via Internal Maxillary Artery):
| Artery | Region Supplied |
|---|---|
| Posterior septal artery (branch of sphenopalatine artery) | Posteroinferior septum; basis of the nasoseptal mucosal flap used in endoscopic skull base reconstruction |
| Greater palatine artery | Enters through the incisive canal; supplies anteroinferior septum |
| Septal branch of superior labial artery (branch of facial artery) | Caudal septum and columella |
From the Internal Carotid Artery (via Ophthalmic Artery):
| Artery | Region Supplied |
|---|---|
| Anterior ethmoid artery | Anterosuperior septum |
| Posterior ethmoid artery | Posterosuperior septum |
Venous Drainage:
- Posteriorly via sphenopalatine vein into the pterygoid plexus
- Anteriorly into the facial veins
- Superiorly via ethmoidal veins into the superior ophthalmic system - with possible direct intracranial connections through the foramen caecum into the superior sagittal sinus (this creates a pathway for intracranial spread of infection)
- This is a valveless venous system, making retrograde spread of infection to the cavernous sinus possible. - KJ Lee's Essential Otolaryngology, p. 518
5. Nerve Supply
Sensory (Trigeminal Nerve):
| Division | Nerve | Region |
|---|---|---|
| V1 (Ophthalmic) | Internal nasal branch of anterior ethmoidal nerve | Anterior and superior nasal cavity septum |
| V1 | Posterior ethmoidal nerve | Posterior superior nasal cavity |
| V2 (Maxillary) | Nasopalatine nerve (through sphenopalatine foramen) | Posterior nasal cavity and septum; the largest septal nerve, passes anteriorly and inferiorly to the incisive canal |
Autonomic:
- Parasympathetic: Preganglionic fibers travel with the facial nerve → greater superficial petrosal nerve → joins deep petrosal nerve → forms the vidian nerve → synapse in the sphenopalatine ganglion → postganglionic fibers innervate nasal mucosa (controls secretion and vascular tone)
- Sympathetic: Postsynaptic fibers pass through the sphenopalatine ganglion and terminate in nasal mucosa (vasoconstriction, reduces secretion)
- The trigeminal fibers transmit pain, temperature, and touch from the nasal mucosa. - Cummings Otolaryngology, p. 566
6. Little's Area (Kiesselbach's Plexus)
Definition and Location
Little's area (also called Kiesselbach's plexus or the Kiesselbach-Little area) is a small zone of mucosa on the anterior nasal septum, approximately 1.5 mm wide, located at the junction between the nasal vestibule and the actual nasal cavity. It contains a rich anastomotic capillary network just beneath a thin mucosal layer. - Color Atlas of Human Anatomy, p. 175
Arterial Contributions (5 vessels converge here):
| Artery | Origin |
|---|---|
| Anterior ethmoid artery | Internal carotid (via ophthalmic artery) |
| Posterior ethmoid artery | Internal carotid (via ophthalmic artery) |
| Posterior septal branch of sphenopalatine artery | External carotid (via internal maxillary artery) |
| Greater palatine artery | External carotid (via internal maxillary artery) |
| Septal branch of superior labial artery | External carotid (via facial artery) |
This makes Little's area an anastomotic highway between the internal and external carotid systems. - KJ Lee's Essential Otolaryngology, p. 584
Why Is It So Prone to Bleeding?
- The vessels form a rich vascular bed of long capillary loops right beneath a thin, exposed mucosa
- Located at the anterior septum where it is easily traumatized by digital trauma (nose picking) - the single most common cause
- Exposed to turbulent, drying airflow at the nasal entrance, which can desiccate and crack the mucosa
- Receives convergent blood supply from both carotid systems with no redundancy in pressure equalization
Little's area is the most common site of epistaxis overall, and in children it accounts for more than 90% of all nosebleeds. - Scott-Brown's Vol 2, p. 285

Figure: Endoscopic view showing septal crusting over Little's area - a precursor to epistaxis in children (Scott-Brown's Vol 2, p. 285)
7. Nasal Lateral Wall and Nasal Cavity Reference
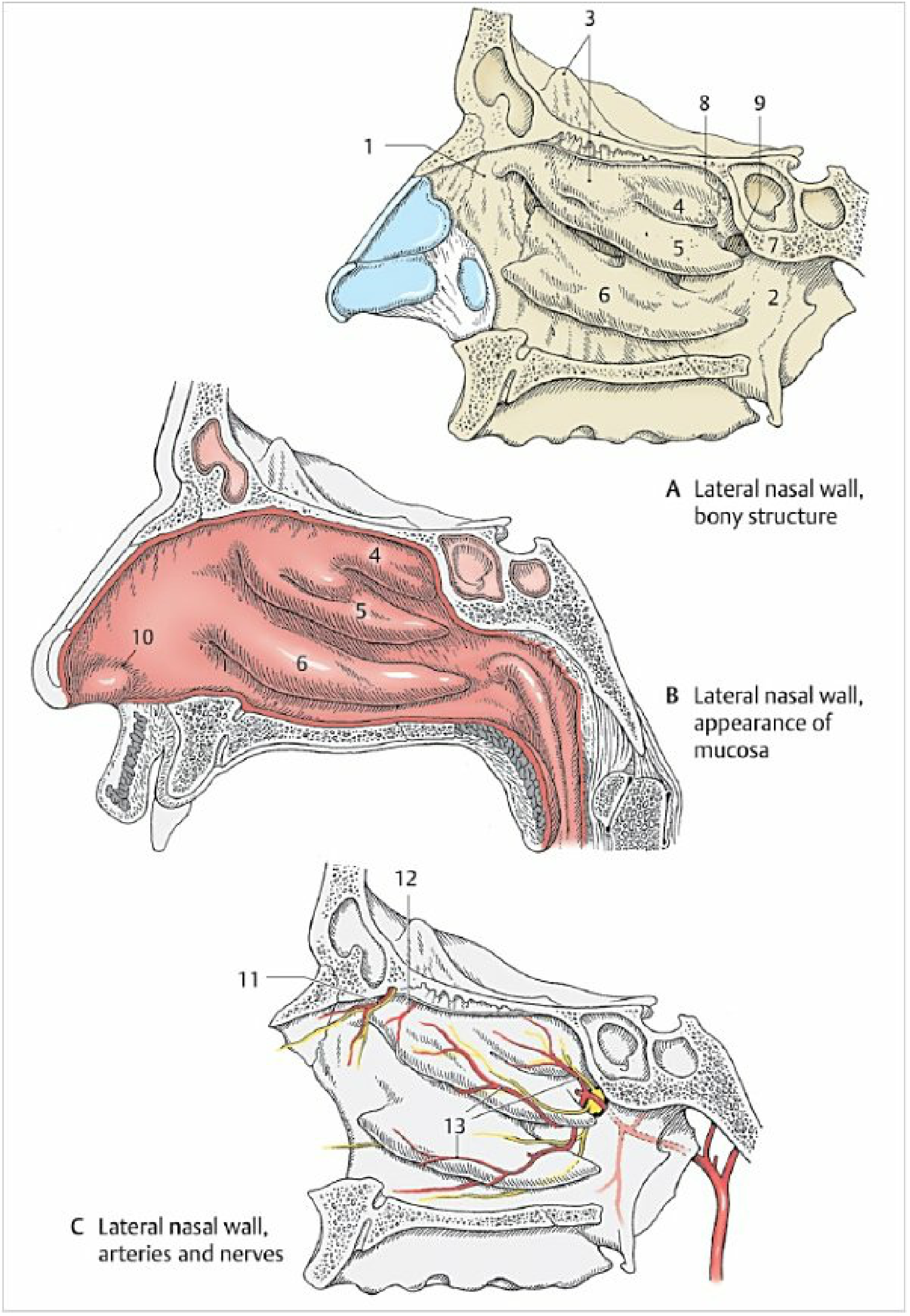
Figure: Lateral nasal wall anatomy (A) bony structure, (B) mucosal appearance, (C) arteries and nerves (Color Atlas of Human Anatomy, p. 176)
8. Clinical Relevance Summary
| Topic | Key Point |
|---|---|
| Epistaxis | Little's area (Kiesselbach's plexus) is the most common site; treated with silver nitrate cautery, nasal packing, or vessel ligation |
| Deviated nasal septum (DNS) | Can arise from trauma or developmental causes; leads to nasal obstruction, recurrent sinusitis, sleep disturbance; corrected by septoplasty |
| Septoplasty | Preserves an "L-strut" (1 cm dorsal + 1 cm caudal cartilage) to maintain support; ~20-30% of patients have incomplete symptom relief with suboptimal technique |
| Nasoseptal flap | Based on the posterior septal artery (branch of SPA); workhorse flap for endoscopic skull base reconstruction |
| Septal perforation | Can result from trauma, cocaine use, granulomatous disease (GPA, sarcoidosis), or surgical complication |
| Cavernous sinus thrombosis risk | The valveless venous drainage from the nasal septum (via ethmoidal veins) can allow retrograde spread of infection intracranially |
Sources:
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery (Vol 1 & 2), pp. 1014-1015, 285
- Cummings Otolaryngology Head and Neck Surgery, pp. 565-566
- KJ Lee's Essential Otolaryngology, pp. 517-518, 584
- Color Atlas of Human Anatomy Vol. 2, pp. 175-176
Tell me in detail about the constrictor of pharynx and Killianhs dehiscence [zenkers diverticulum]
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive, richly illustrated information from multiple authoritative sources. Let me compile the full detailed answer.
Constrictors of the Pharynx and Killian's Dehiscence (Zenker's Diverticulum)
PART 1: CONSTRICTORS OF THE PHARYNX
Overview
The pharynx has two layers of muscle:
- Outer circular layer: three constrictor muscles (superior, middle, inferior) - they overlap like stacked flower pots, with each lower muscle overlapping the upper border of the one below
- Inner longitudinal layer: palatopharyngeus, stylopharyngeus, salpingopharyngeus
The constrictors narrow the pharyngeal cavity sequentially from top to bottom during swallowing to propel the food bolus into the esophagus. All three are innervated by the vagus nerve (CN X) via the pharyngeal plexus.
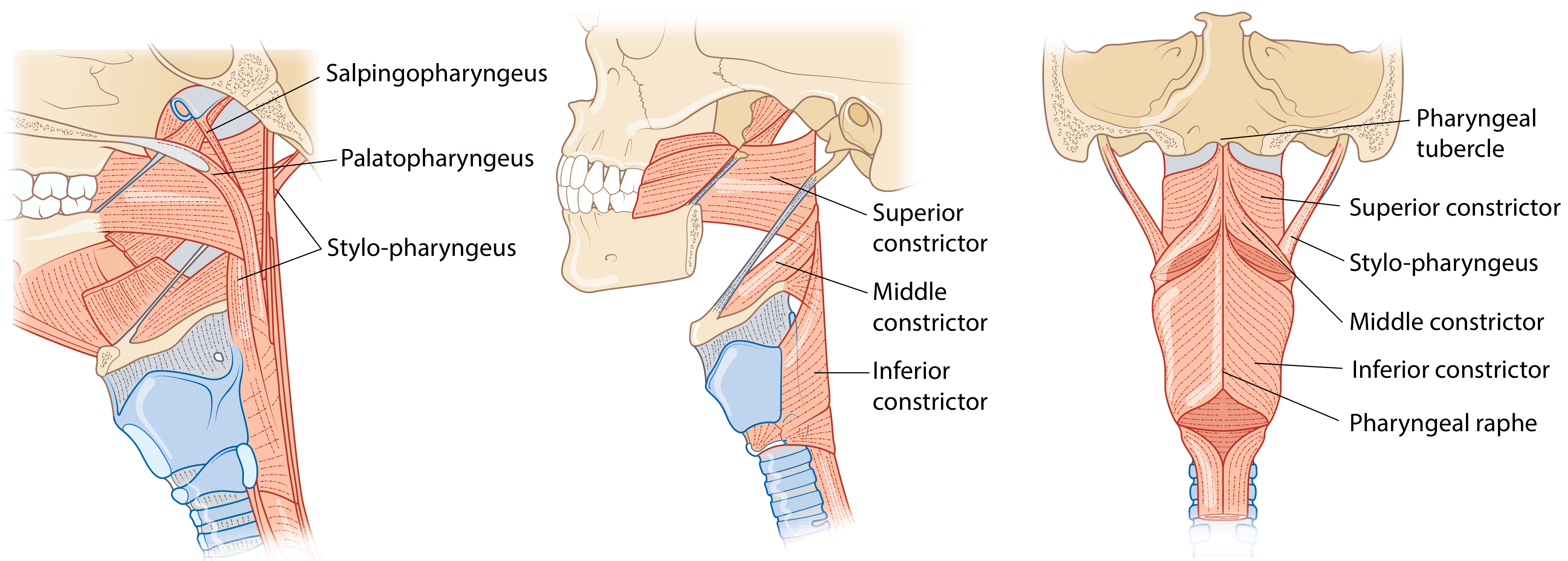
Figure: Pharyngeal muscles - (left) sagittal with longitudinal muscles, (centre) lateral view, (right) posterior view showing the three constrictors and pharyngeal raphe (Scott-Brown's Otorhinolaryngology)
1. Superior Constrictor
| Feature | Detail |
|---|---|
| Origin (anterior) | Pterygomandibular raphe and adjacent bone on the mandible; pterygoid hamulus (medial pterygoid plate) |
| Insertion (posterior) | Median pharyngeal raphe and pharyngeal tubercle of occipital bone |
| Innervation | Vagus nerve (CN X) via pharyngeal plexus |
| Function | Constricts the upper pharynx during swallowing |
Key clinical/anatomical notes:
- Passavant's ridge: a visible soft-tissue projection formed by contraction of the superior end of the superior constrictor during swallowing; it can be seen endoscopically and plays a role in velopharyngeal closure
- The glossopharyngeal nerve (CN IX) passes under the free edge of the superior constrictor, lying just deep to the palatine tonsil
- The palatopharyngeal sphincter lies on the deep surface of the superior constrictor
- The superior constrictor does not reach the skull base - the gap above it is filled by the pharyngobasilar fascia
2. Middle Constrictor
| Feature | Detail |
|---|---|
| Origin (anterior) | Greater horn of hyoid bone (upper margin), lesser horn of hyoid, and stylohyoid ligament |
| Insertion (posterior) | Median pharyngeal raphe |
| Innervation | Vagus nerve (CN X) via pharyngeal plexus |
| Function | Constricts the middle pharynx during swallowing |
Key anatomical note:
- The muscular anterior wall is incomplete between the middle and inferior constrictors - this gap is covered by the thyrohyoid membrane. The internal laryngeal nerve and superior laryngeal artery and vein pass through this membrane on its superolateral aspect. - Scott-Brown's, p. 788
3. Inferior Constrictor
The thickest of the three constrictors. Classically described as two separate muscular components:
| Component | Origin | Character |
|---|---|---|
| Thyropharyngeus (upper part) | Oblique line of thyroid cartilage; small part of inferior thyroid horn; tendinous fascia crossing the cricothyroid muscle | Oblique fibers, passes posteromedially to pharyngeal raphe; some fibers cross the raphe to fuse with the contralateral muscle |
| Cricopharyngeus (lower part) | Lateral aspect of cricoid cartilage (between cricothyroid attachment and inferior thyroid horn) | Horizontal fibers; encircles the cricoid arch without fusing at the pharyngeal raphe |
Cricopharyngeus - the sphincter:
- Distinctively different from all other constrictors - it is thicker, rounder, and its horizontal fibers create a true sphincter
- Acts as the upper esophageal sphincter (UES)
- Is in tonic contraction at rest (keeps the esophageal inlet closed, prevents air from entering during respiration)
- Actively dilates (relaxes) during swallowing - triggered by laryngeal elevation
- Is continuous below with the circular muscular coat of the upper esophagus
- The narrowest point of the pharyngeal cavity is the inferior constrictor's attachment to the cricoid cartilage
Important neurovascular relations at the inferior constrictor:
- The recurrent laryngeal nerve + inferior laryngeal artery and vein pass upward deep to the lower margin of the inferior constrictor - Scott-Brown's, p. 788
| Space | Location | Clinical Importance |
|---|---|---|
| Killian's dehiscence | Posterior triangular gap between thyropharyngeus (above) and cricopharyngeus (below) | Site of Zenker's diverticulum formation |
| Laimer-Hackerman space | Between posterior cricopharyngeus and esophageal musculature | Anatomical landmark |
| Killian-Jamieson space | Lateral dehiscence inferior to cricopharyngeus | Transmits branches of the inferior thyroid artery; site of Killian-Jamieson diverticulum (lateral, smaller, rarer) |
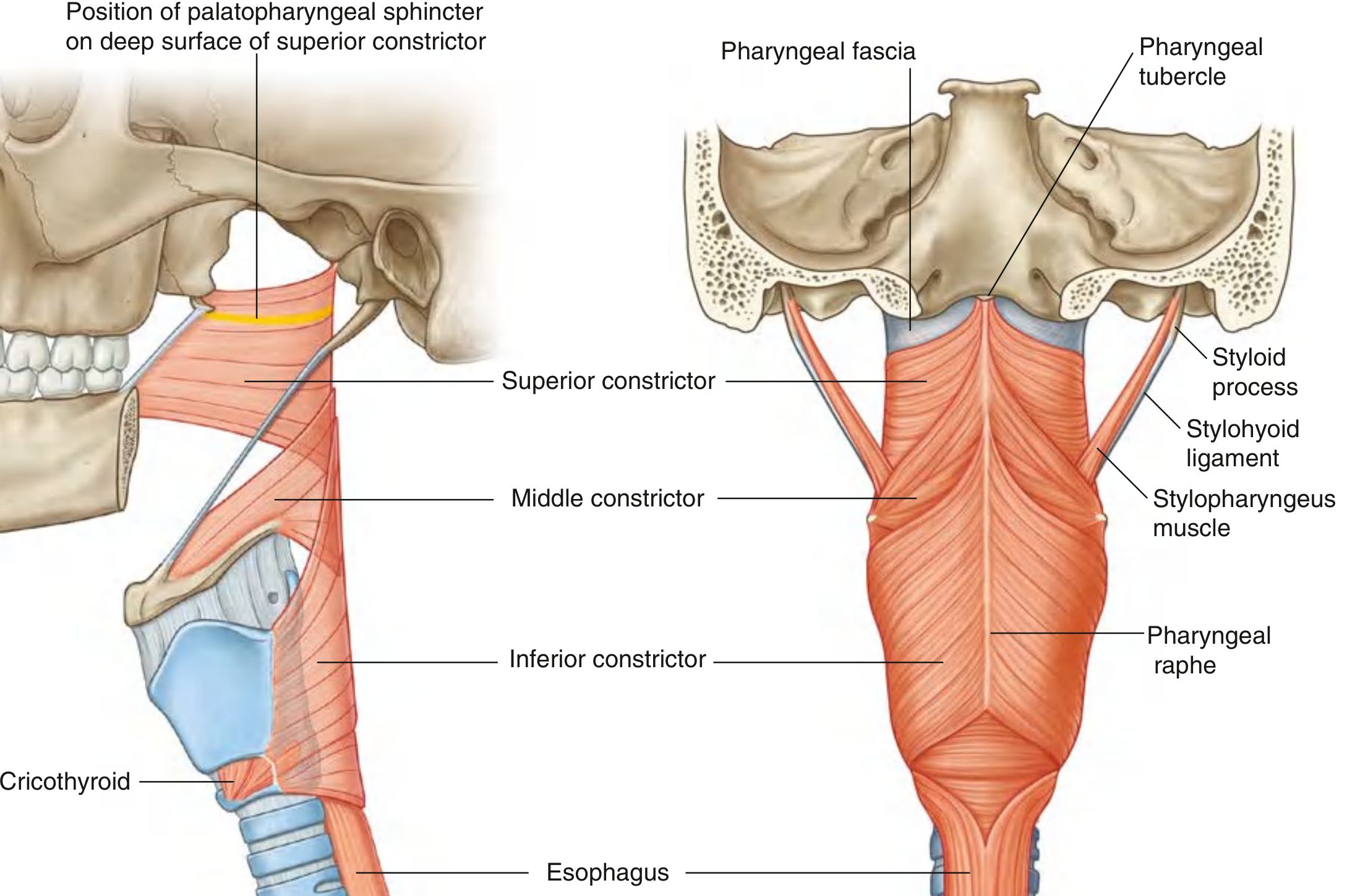
Figure: Constrictor muscles - lateral and posterior views showing three constrictors, pharyngeal raphe, and styloid process (Gray's Anatomy for Students)
Constrictor Overlap Arrangement
The constrictors overlap like stacked flower pots:
- Inferior constrictors overlap the lower margins of the middle constrictors
- Middle constrictors overlap the lower margins of the superior constrictors
This arrangement ensures continuous muscular coverage of the pharyngeal wall while allowing sequential peristaltic constriction during swallowing. - Gray's Anatomy for Students, p. 1182
PART 2: KILLIAN'S DEHISCENCE AND ZENKER'S DIVERTICULUM
Killian's Dehiscence - Anatomy
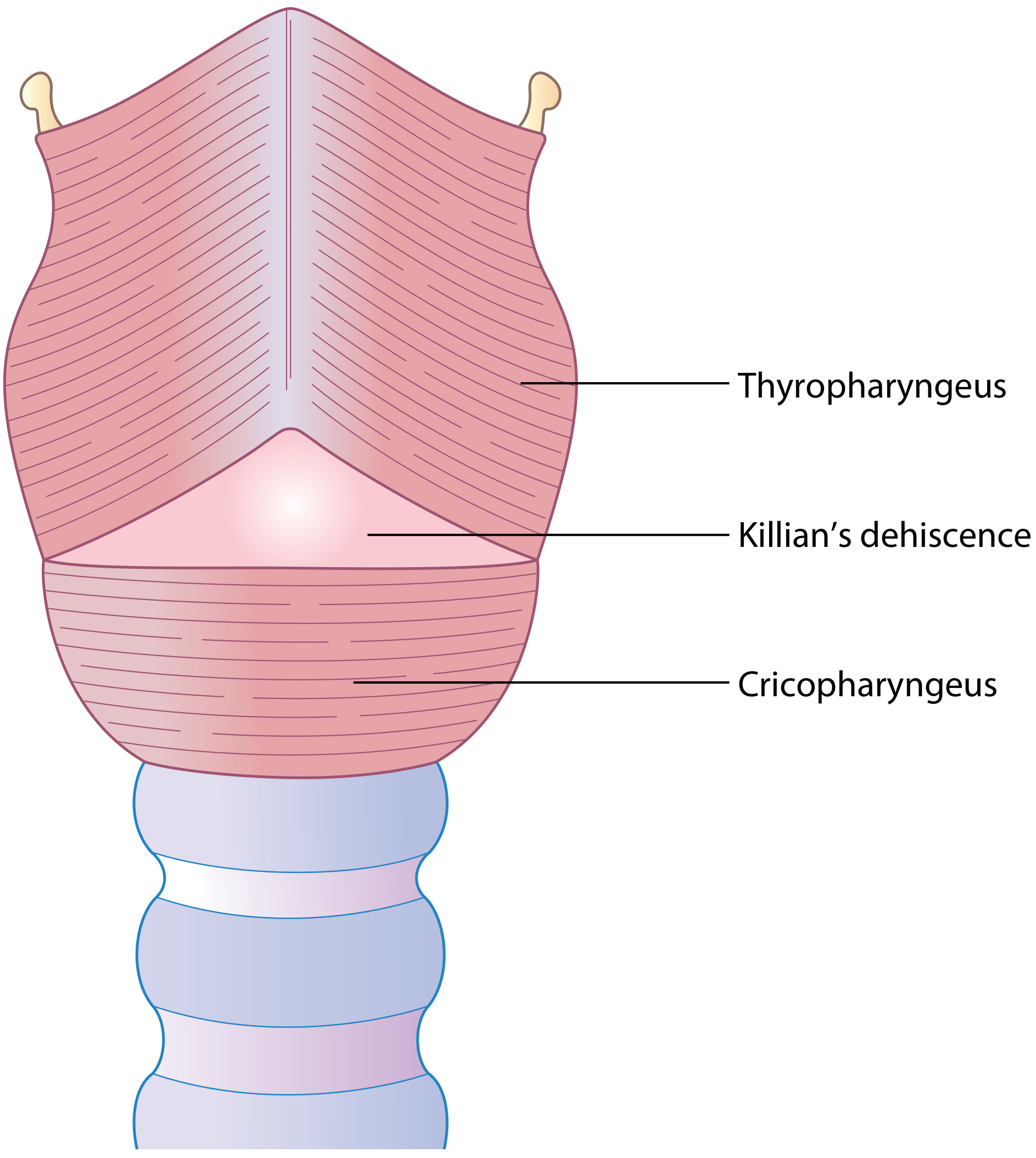
Figure: Killian's dehiscence - the triangular area of weakness between thyropharyngeus and cricopharyngeus (Scott-Brown's Otorhinolaryngology)
Killian's dehiscence is the triangular area of muscular weakness on the posterior wall of the most caudal part of the hypopharynx, bounded by:
- Superiorly: oblique fibers of thyropharyngeus (upper part of inferior constrictor)
- Inferiorly: horizontal fibers of cricopharyngeus (lower part of inferior constrictor)
The triangular zone contains very few muscle fibers and is supported only by mucosa and submucosa. First described by Gustav Killian in 1908. - Scott-Brown's, p. 855
Why does this gap exist? The descent of the human larynx during evolution (which enabled speech) creates this natural gap. Pharyngeal pouches are rare in other animals, supporting this evolutionary explanation. - Scott-Brown's, p. 857
Zenker's Diverticulum (Pharyngeal Pouch)
Definition: A pulsion diverticulum - herniation of pharyngeal mucosa and submucosa through Killian's dehiscence, above the cricopharyngeal muscle, at the level of the 6th cervical vertebra. Terms used interchangeably: pharyngeal pouch, hypopharyngeal diverticulum, Zenker's diverticulum.
Historical note: First described by Ludlow of Bristol in 1769. Clinically characterized by Zenker in 1878. First successful excision by Wheeler in 1885.
Epidemiology
- Incidence: 0.47-1 per 100,000 per year
- Predominantly affects Caucasians (rare in Asian and Afro-Caribbean races)
- Male:female ratio ~2:1
- Almost exclusively patients over 50 years, most commonly 6th-9th decade
- A true false diverticulum - wall consists of mucosa and submucosa only (no muscle)
Pathogenesis / Aetiology
The aetiology is multifactorial with three main theories proposed:
Theory 1 - Anatomical weakness (Killian's dehiscence)
The inherent weakness of the posterior pharyngeal wall at the dehiscence means that normal swallowing pressures over time can cause mucosal prolapse - particularly in individuals with a large or weak dehiscence. The descent of the human larynx (unique to humans) is proposed to create the dehiscence. - Scott-Brown's, p. 857
Theory 2 - Failed relaxation of cricopharyngeus
The cricopharyngeus is normally in tonic contraction but relaxes during swallowing (at the end of stage 2 when the peristaltic wave descends). Failure of this relaxation - due to:
- Fibrosis (Cook's theory - laryngopharyngeal reflux as a cause)
- Muscle spasm (Negus, Sutherland, Belsey)
- Weakening of prevertebral fascia with age (Dohlman & Mattson) - the larynx falls forward, decreasing the circumference that cricopharyngeus is stretched across, creating functional obstruction
...creates elevated intrapharyngeal pressure above the cricopharyngeus, leading to herniation through Killian's dehiscence. Primary muscle disorders (e.g. inclusion body myositis) can also cause failed cricopharyngeal relaxation.
Theory 3 - Incoordination of pharyngeal muscles
Ardran, Kemp and Lund showed that in pouch patients:
- Oropharyngeal contraction is weak
- Pharyngeal peristaltic wave is weak
- Premature closure of cricopharyngeus occurs before the stripping wave reaches it
The descending wave meets the prematurely closed sphincter, pushing the posterior pharyngeal wall into a dimple that over years enlarges into a pouch.
Consensus conclusion: Incoordination between descending peristaltic wave AND failed cricopharyngeal relaxation → abnormally high intraluminal pressure → mucosal herniation through Killian's dehiscence. - Scott-Brown's, p. 858
Growth and Expansion of the Pouch
- Initially the pouch expands posteriorly, but prevertebral fascia limits this direction
- Larger pouches project laterally and inferiorly, predominantly to the left side (the more exposed side)
- A very large pouch can push the esophagus to one side, sitting in line with the pharynx and causing severe dysphagia
- Contents can spill into the larynx, causing aspiration pneumonia
Clinical Features
| Symptom | Details |
|---|---|
| Dysphagia | Present in virtually all patients; early - solids sticking, need to swallow multiple times |
| Regurgitation | Undigested food regurgitated hours after eating (hallmark symptom) |
| Halitosis | Due to food retention and decomposition |
| Gurgling/noise | Especially after eating |
| Aspiration | Cough, recurrent chest infections, aspiration pneumonia |
| Hoarseness | Voice change due to laryngeal involvement |
| Weight loss / cachexia | In large pouches with severe dysphagia |
Note: Symptoms progress insidiously - patients often present late with a well-developed pouch.
Alarm features suggesting carcinoma within the pouch:
- Rapidly increasing dysphagia
- Pain
- Blood in regurgitated food
- Neck mass or nodes
Pathology (Histology)
The excised pouch wall shows:
- Stratified squamous epithelium lining
- Submucosa (no muscular layer = false diverticulum)
- Surrounding fibrous tissue
- Scanty muscle fibers near the neck of the pouch
- Evidence of myositis in some patients (isolated or part of systemic disease)
Carcinoma in pouch: Rare (~0.4%). Usually squamous cell carcinoma. Caused by chronic irritation from food retention. Risk factors: long-standing pouch, multiple interventions. - Scott-Brown's, p. 858-859
Diagnosis
| Investigation | Details |
|---|---|
| Barium swallow (lateral projection) | Gold standard - shows contrast filling the diverticulum during swallowing; dynamic video fluoroscopy preferred (assesses pharyngeal muscle function and gastric reflux simultaneously) |
| CT neck/chest | Useful for large pouches, assessing extent and relationships |
| Endoscopy | Required to exclude co-existing carcinoma - must inspect pouch lining; wash out food debris with saline for reliable view |
Important: A lower oesophageal carcinoma can coexist with a pharyngeal pouch - the barium study must include the lower oesophagus and stomach. - Scott-Brown's, p. 856
Management Options
1. Conservative
- Patients with minimal symptoms or unfit for surgery
- Dietary modification, positional manoeuvres
2. Endoscopic Surgery (preferred in elderly/frail - short anaesthetic, minimal intervention)
| Technique | Description |
|---|---|
| Rigid endoscopy + stapler diverticulotomy | Doyen-Dohlman procedure with stapler; divides the cricopharyngeal bar (common wall between pouch and oesophagus) using a linear stapler - most popular modern technique |
| Rigid endoscopy + laser (CO₂) | Laser division of the cricopharyngeal bar |
| Rigid endoscopy + diathermy | Division of bar with diathermy |
| Flexible endoscopy | Diathermy division via flexible scope |
All endoscopic techniques always include cricopharyngeal myotomy (since the cricopharyngeus muscle lies within the bar).
3. External (Open) Surgery
| Technique | Description |
|---|---|
| Open pouch excision + cricopharyngeal myotomy | Via left cervical approach; formal excision of the sac with separate myotomy |
| Pouch inversion + cricopharyngeal myotomy | Inverts and suspends the sac rather than excising |
| Cricopharyngeal myotomy alone | For early/small pouches; relieves the obstruction |
The rationale for always performing cricopharyngeal myotomy: Since failed cricopharyngeal relaxation is involved in pathogenesis, myotomy addresses the causative mechanism and prevents recurrence. - Scott-Brown's, p. 858
Summary Table: Key Spaces at the Inferior Constrictor
| Space | Boundaries | Clinical Significance |
|---|---|---|
| Killian's dehiscence | Between thyropharyngeus (above) and cricopharyngeus (below) - posterior midline | Site of Zenker's diverticulum (posterior pulsion diverticulum) |
| Laimer-Hackerman space | Between posterior cricopharyngeus and esophageal musculature | Anatomical landmark inferior to cricopharyngeus |
| Killian-Jamieson space | Lateral dehiscence below cricopharyngeus, anterolateral | Transmits inferior thyroid artery branches; site of Killian-Jamieson diverticulum (lateral, smaller, usually asymptomatic) |
Sources:
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery (Vol 3), pp. 788, 855-859
- KJ Lee's Essential Otolaryngology, pp. 669, 833
- Gray's Anatomy for Students, p. 1182
- Yamada's Textbook of Gastroenterology
Classify white matter of brain and describe internal capsule in detail
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive, well-illustrated content from multiple authoritative sources. Let me compile the detailed answer.
White Matter of the Brain: Classification and the Internal Capsule
PART 1: CLASSIFICATION OF WHITE MATTER OF THE BRAIN
The cerebral hemispheres contain billions of myelinated axons - their whitish appearance gives "white matter" its name. The gray matter (cell bodies) lies on the cortical surface and in deep nuclei, while white matter fills the interior. The opposite arrangement holds in the spinal cord. - Gray's Anatomy for Students, p. 1302
White matter tracts carry information to and from the cerebral cortex and are classified into three major groups based on their connections:
I. PROJECTION FIBERS
Fibers that connect the cerebral cortex with subcortical structures (brainstem, spinal cord, thalamus, basal ganglia). They run vertically and are of two types:
| Type | Direction | Examples |
|---|---|---|
| Corticofugal (efferent) | Cortex → subcortical targets | Corticospinal, corticobulbar, corticopontine, corticothalamic, corticoreticular tracts |
| Corticopetal (afferent) | Subcortical → cortex | Thalamocortical radiations (anterior, superior, posterior/optic, inferior/auditory) |
These fibers converge as they descend from the cortex, passing through the corona radiata (fan-shaped arrangement above the internal capsule) and compressing into the internal capsule, then continuing as the cerebral peduncles in the midbrain. - Kaplan & Sadock's Comprehensive Textbook of Psychiatry, p. 197
II. COMMISSURAL FIBERS
Fibers that cross the midline to interconnect corresponding (homotopic) or dissimilar (heterotopic) cortical areas in the two cerebral hemispheres.
| Structure | Content / Connections |
|---|---|
| Corpus callosum | Largest fiber bundle in the brain (~300 million axons). Divided into: rostrum, genu (frontal lobes), body (parietal/motor/sensory areas), and splenium (occipital/posterior parietal lobes). Almost all cortical regions are connected except the hand area of motor and somatosensory cortex |
| Anterior commissure | Connects the two temporal lobes (olfactory areas, amygdala, anterior temporal cortex) |
| Posterior commissure | Connects pretectal nuclei; involved in the pupillary light reflex |
| Hippocampal commissure (psalterium) | Connects hippocampal formations bilaterally |
| Habenular commissure | Connects habenular nuclei |
III. ASSOCIATION FIBERS
Fibers that connect cortical areas within the same hemisphere. They are further subdivided by length:
A. Short Association Fibers (U-fibers / arcuate fibers)
- Connect adjacent gyri within the same lobe
- Form a "U" shape dipping under the sulcus between gyri
- Located just beneath the cortical gray matter
- Most superficial of all white matter
B. Long Association Fibers (Named Fasciculi)
| Fasciculus | Course | Connections |
|---|---|---|
| Superior longitudinal fasciculus (SLF) | Runs laterally above the insula | Frontal ↔ parietal ↔ occipital cortices |
| Arcuate fasciculus | Arcs around the insula | Frontal lobe (Broca's area) ↔ temporal lobe (Wernicke's area); critical for language |
| Uncinate fasciculus | Curved, hooked bundle through the limen insulae | Orbital frontal lobe ↔ anterior temporal lobe |
| Inferior occipitofrontal fasciculus | Courses ventrally and laterally | Occipital lobe ↔ frontal lobe |
| Inferior longitudinal fasciculus (ILF) | Along the lateral temporal and occipital regions | Temporal ↔ occipital lobes |
| Cingulum | Within white matter deep to the cingulate gyrus | Cingulate gyrus ↔ parahippocampal gyrus; part of Papez circuit |
C. Sub-cortical Capsular Fibers (also association type)
-
External capsule: between claustrum and putamen
-
Extreme capsule: between claustrum and insular cortex
-
Kaplan & Sadock's, pp. 202-203
PART 2: THE INTERNAL CAPSULE
Definition
The internal capsule is a compact lamina of white matter representing the largest projection fiber tract in the brain. It contains afferent and efferent nerve fibers passing to and from the brainstem and the cerebral hemispheres. - Localization in Clinical Neurology, 8e, p. 31
Superiorly it continues as the corona radiata (fan-shaped, expanding toward the cortex).
Inferiorly it continues as the cerebral peduncles (basis pedunculi) in the midbrain.
Shape and Position (Horizontal/Flechsig Section)
On a horizontal (axial) section, the internal capsule appears as a V-shape (like two arrowheads pointing inward, or two letter Vs with points facing medially). The convexity faces inward (medially).
Relations (always remember these):
- Medial: Caudate nucleus (head) and Thalamus
- Lateral: Lenticular nucleus (Putamen + Globus pallidus)
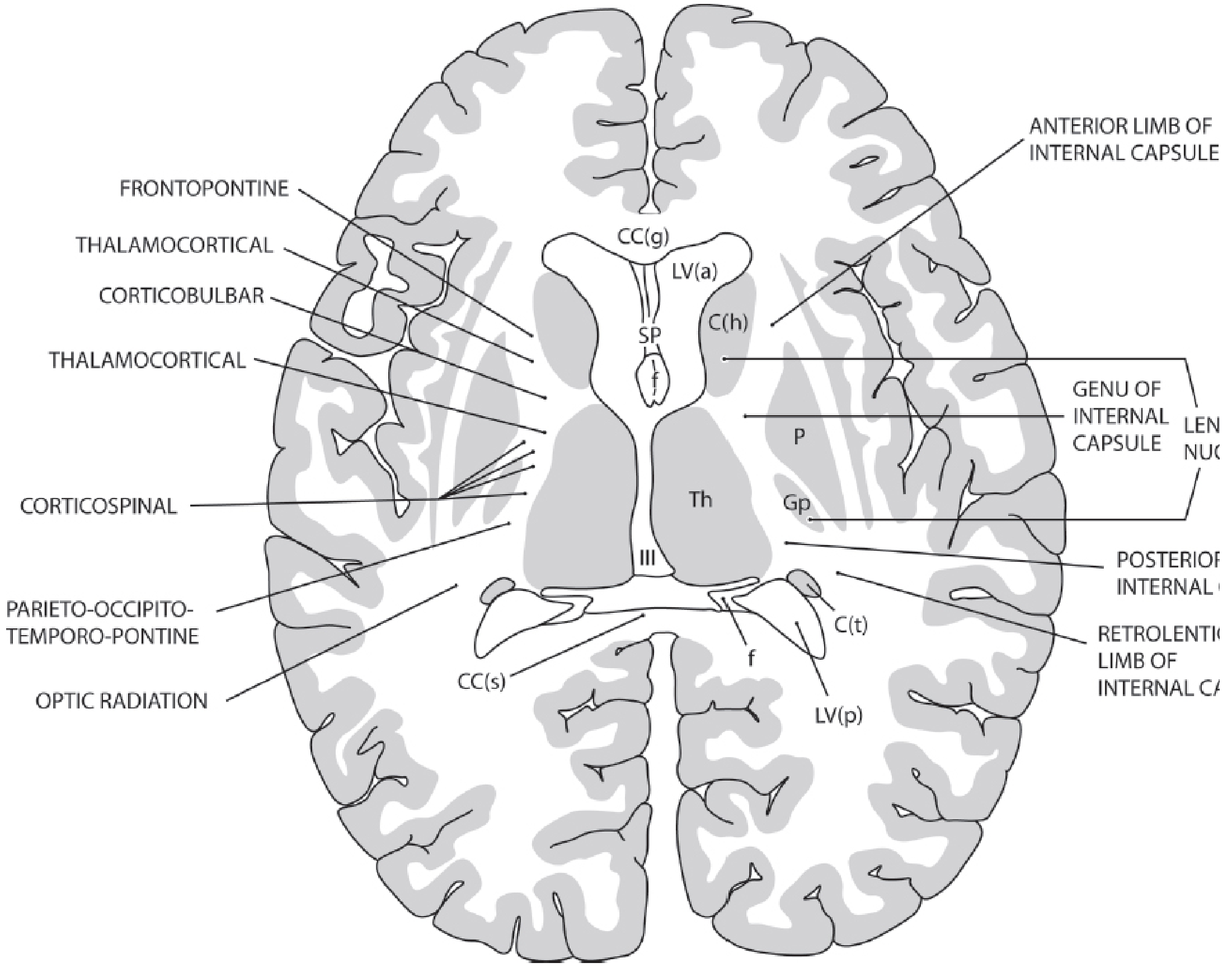
Figure: Horizontal (Flechsig) section of the brain showing all five segments of the internal capsule, with named fiber systems in each segment (Kaplan & Sadock's)
Five Segments and Their Contents
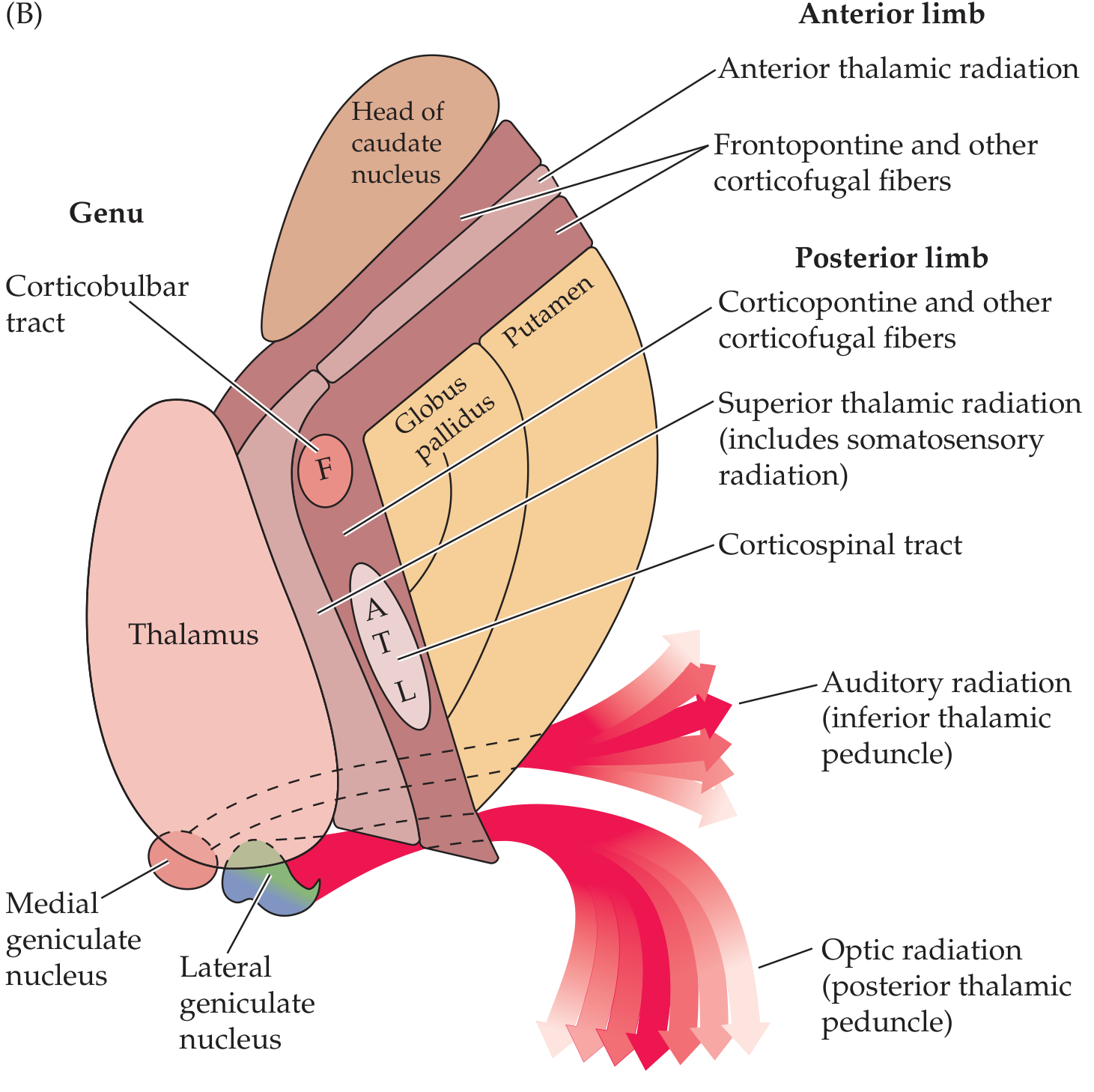
Figure: (A) 3D view of the internal capsule showing its V-shape and relation to thalamus, caudate, and lentiform nucleus. (B) Horizontal section showing all segments and fiber contents with somatotopic map (F=Face, A=Arm, T=Trunk, L=Leg) (Neuroanatomy through Clinical Cases)
1. Anterior Limb (Lenticulocaudate Segment)
- Boundaries: Between the lenticular nucleus (lateral) and the head of the caudate nucleus (medial)
- Length: ~2 cm
- Fibers:
- Frontopontine fibers (frontal lobe → pontine nuclei)
- Anterior thalamic radiation (thalamocortical and corticothalamic fibers connecting thalamus ↔ frontal cortex)
- Caudate-putaminal fibers
2. Genu ("Knee")
- At the bend between anterior and posterior limbs, at the level of the interventricular foramen of Monro
- Fibers:
- Corticobulbar (corticonuclear) tract - upper motor neuron fibers to cranial nerve nuclei in the brainstem
- Corticoreticular fibers (to bilateral brainstem reticular formation)
- Some motor corticopontine fibers
Clinical pearl: The genu syndrome (isolated genu infarct) produces facial and lingual hemiparesis with mild limb involvement because corticobulbar fibers predominantly serve the face and tongue. - Localization in Clinical Neurology, p. 31
3. Posterior Limb (Lenticulothalamic Segment)
- Boundaries: Between the lenticular nucleus (lateral) and the thalamus (medial)
- Length: ~3-4 cm (the largest segment)
- Fibers (anterior to posterior):
- Corticopontine fibers (anterior part)
- Corticospinal tract (caudal half) - somatotopically organized:
- Upper extremity fibers more anterior (shoulder → elbow → wrist → fingers)
- Followed by trunk fibers
- Lower extremity fibers more posterior (hip → knee → ankle → toes)
- Bladder and rectum fibers most posterior
- Superior thalamic radiation (includes somatosensory radiation - VPL/VPM thalamus → somatosensory cortex)
- Corticorubral fibers (to red nucleus)
- Corticothalamic fibers
4. Retrolenticular Segment
- Position: Behind (posterior to) the lenticular nucleus
- Fibers:
- Optic radiation (Gratiolet's radiation / geniculocalcarine tract): Lateral geniculate nucleus (LGN) → primary visual cortex (calcarine cortex)
- Corticotectal fibers (to superior colliculus)
- Corticonigral fibers (to substantia nigra)
- Corticopontine fibers (parieto-occipito-temporo-pontine)
5. Sublenticular Segment
- Position: Inferior to the lenticular nucleus
- Fibers:
- Auditory radiation (inferior thalamic peduncle): Medial geniculate nucleus (MGN) → primary auditory cortex (Heschl's gyri, superior temporal gyrus)
- Temporopontine fibers
- Some visual radiation fibers
| Segment | Key Fibers (Mnemonic) |
|---|---|
| Anterior limb | Anterior thalamic radiation + Frontopontine |
| Genu | CorticoBulbar (face/tongue UMN) |
| Posterior limb | CorticoSpinal (somatotopic: arm anterior, leg posterior) + Superior thalamic/sensory radiation |
| Retrolenticular | Optic radiation (visual) |
| Sublenticular | Auditory radiation |
Blood Supply
The internal capsule has a segmental blood supply - this is of immense clinical importance since different vessels' occlusions damage different parts.
| Segment | Arterial Supply |
|---|---|
| Anterior limb | Recurrent artery of Heubner (branch of anterior cerebral artery, ACA) |
| Genu | Anterior choroidal artery (branch of internal carotid or MCA) |
| Genu + middle and inferior posterior limb | Anterior choroidal artery |
| Superior part of anterior and posterior limbs | Lenticulostriate arteries (branches of middle cerebral artery, MCA) |
- Localization in Clinical Neurology, p. 31
The lenticulostriate arteries (also called Charcot's arteries of cerebral hemorrhage) are end-arteries with thin walls, making them especially vulnerable to hypertensive hemorrhage - the most common cause of internal capsule stroke.
3D Spatial Relationships
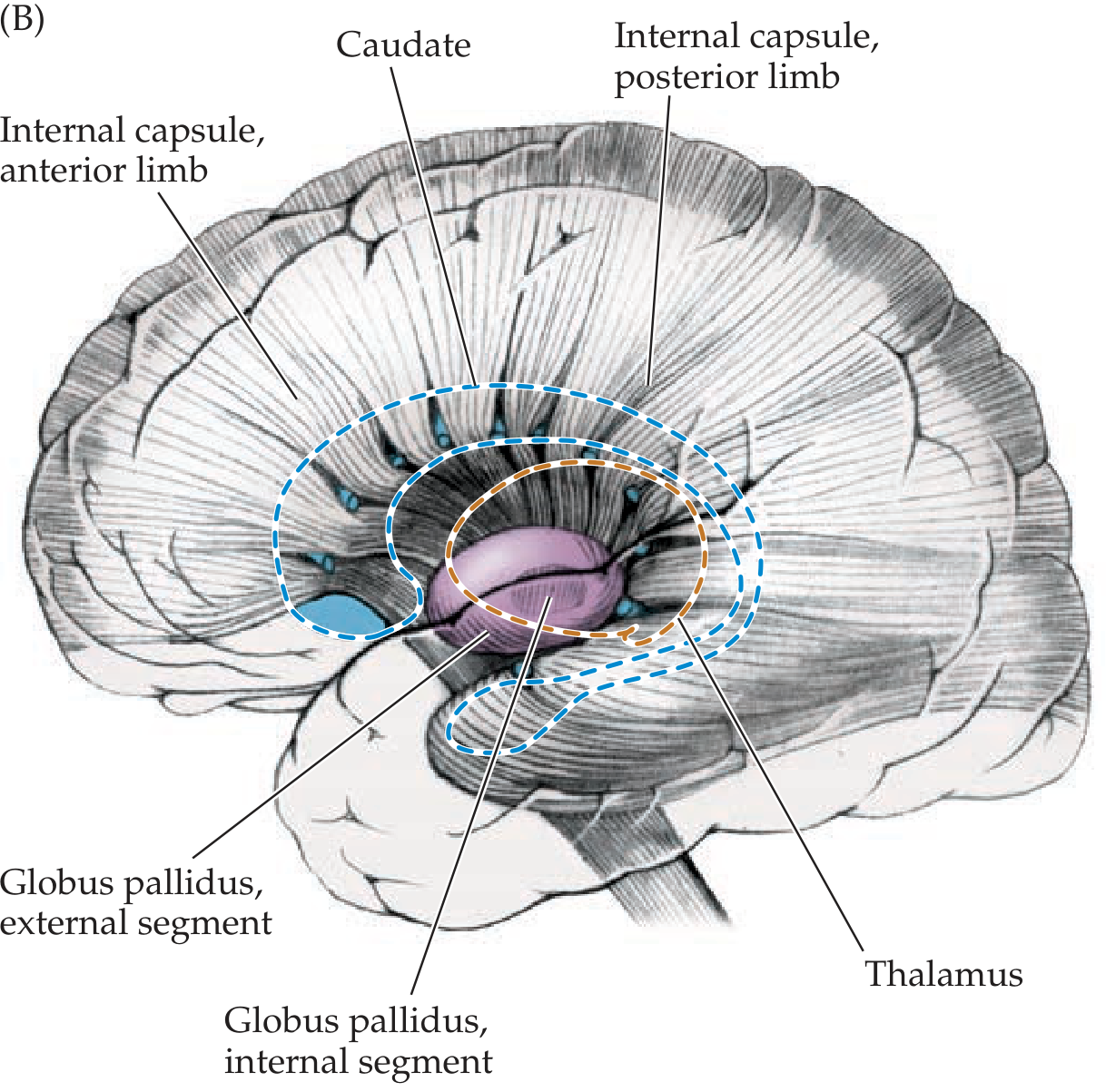
Figure: Lateral view of the internal capsule showing its anterior and posterior limbs, with the putamen (removed), globus pallidus, and thalamus (Neuroanatomy through Clinical Cases)
Moving lateral to medial through a horizontal section:
Insula → Extreme capsule → Claustrum → External capsule → Putamen → External medullary lamina → GPe → Internal medullary lamina → GPi → Internal capsule → Thalamus/Caudate
Clinical Significance
Because the internal capsule concentrates vast numbers of motor and sensory fibers into a small area, even a small lesion (lacunar infarct, hypertensive hemorrhage) causes profound deficits.
| Lesion Location | Clinical Syndrome |
|---|---|
| Posterior limb (corticospinal) | Contralateral hemiparesis (arm + leg), with face spared relatively |
| Genu (corticobulbar) | Contralateral facial/tongue paresis, dysarthria, dysphagia (capsular genu syndrome) |
| Posterior limb + genu | Pure motor hemiplegia (face + arm + leg) |
| Posterior limb + thalamic radiation | Sensorimotor stroke (hemiparesis + hemisensory loss) |
| Retrolenticular segment | Homonymous hemianopia (optic radiation) |
| Sublenticular segment | Auditory deficits / cortical deafness |
| Lateral and posterior capsule | Contralateral: hemiparesis, numbness, dysarthria, homonymous hemianopia with tongue of sparing along horizontal meridian, memory impairment |
Pure motor hemiplegia (contralateral face, arm, and leg weakness without sensory/visual/cognitive deficits) is the classic lacunar syndrome from a small deep infarct in the posterior limb. - Bradley and Daroff's Neurology, p. 3310
Summary Table: Internal Capsule
| Feature | Detail |
|---|---|
| Shape on axial section | V-shaped, convexity facing medially |
| Medial relations | Head of caudate + Thalamus |
| Lateral relation | Lenticular nucleus (putamen + globus pallidus) |
| Continues superiorly as | Corona radiata |
| Continues inferiorly as | Cerebral peduncles (basis pedunculi) |
| Most important clinical segment | Posterior limb (corticospinal tract) |
| Key blood supply | Lenticulostriates (MCA) - prone to hypertensive hemorrhage |
Sources:
- Localization in Clinical Neurology, 8th Edition, pp. 31-32
- Neuroanatomy through Clinical Cases, 3rd Edition, pp. 256-257, 771-772
- Kaplan & Sadock's Comprehensive Textbook of Psychiatry, pp. 197-203
- Gray's Anatomy for Students, pp. 1302-1303
- Bradley and Daroff's Neurology in Clinical Practice, pp. 3297-3316
This is a shared conversation. Sign in to Orris to start your own chat.