pleural tap clinical anatomy
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive content from multiple authoritative textbooks. Let me compile the full, well-structured answer.
Pleural Tap (Thoracocentesis/Thoracentesis) - Clinical Anatomy
Definition and Purpose
A pleural tap (thoracocentesis, thoracocentesis) is a procedure in which a needle or catheter is introduced through the chest wall into the pleural space to aspirate fluid (or occasionally air). It is one of the most commonly performed interventional procedures in hospital practice.
- Diagnostic tap: 50 mL of fluid obtained for laboratory analysis (protein, LDH, cytology, microbiology)
- Therapeutic tap: typically up to 1.5 L removed to relieve dyspnea from a large effusion
- Roberts and Hedges' Clinical Procedures in Emergency Medicine, p. 250
Relevant Anatomy
1. The Pleural Space
The pleural cavity is a potential space between the visceral pleura (tightly adherent to the lung surface) and the parietal pleura (lining the chest wall, diaphragm, and mediastinum). In health it contains only a thin film of fluid (~10-20 mL) for lubrication.
The parietal pleura is divided into:
- Costal part - lines the bony thoracic wall
- Diaphragmatic part - overlies the diaphragm
- Mediastinal part - adjacent to mediastinal connective tissue
- Pleural cupula - extends above the superior thoracic aperture (clinically important - risk of pneumothorax from subclavian/jugular line insertion)
- Color Atlas of Human Anatomy Vol. 2 Internal Organs, p. 224
2. Pleural Recesses
The costodiaphragmatic recess is the most dependent part of the pleural cavity - the gutter between the chest wall and diaphragm where fluid accumulates by gravity. This is the target for pleural aspiration in the upright patient.
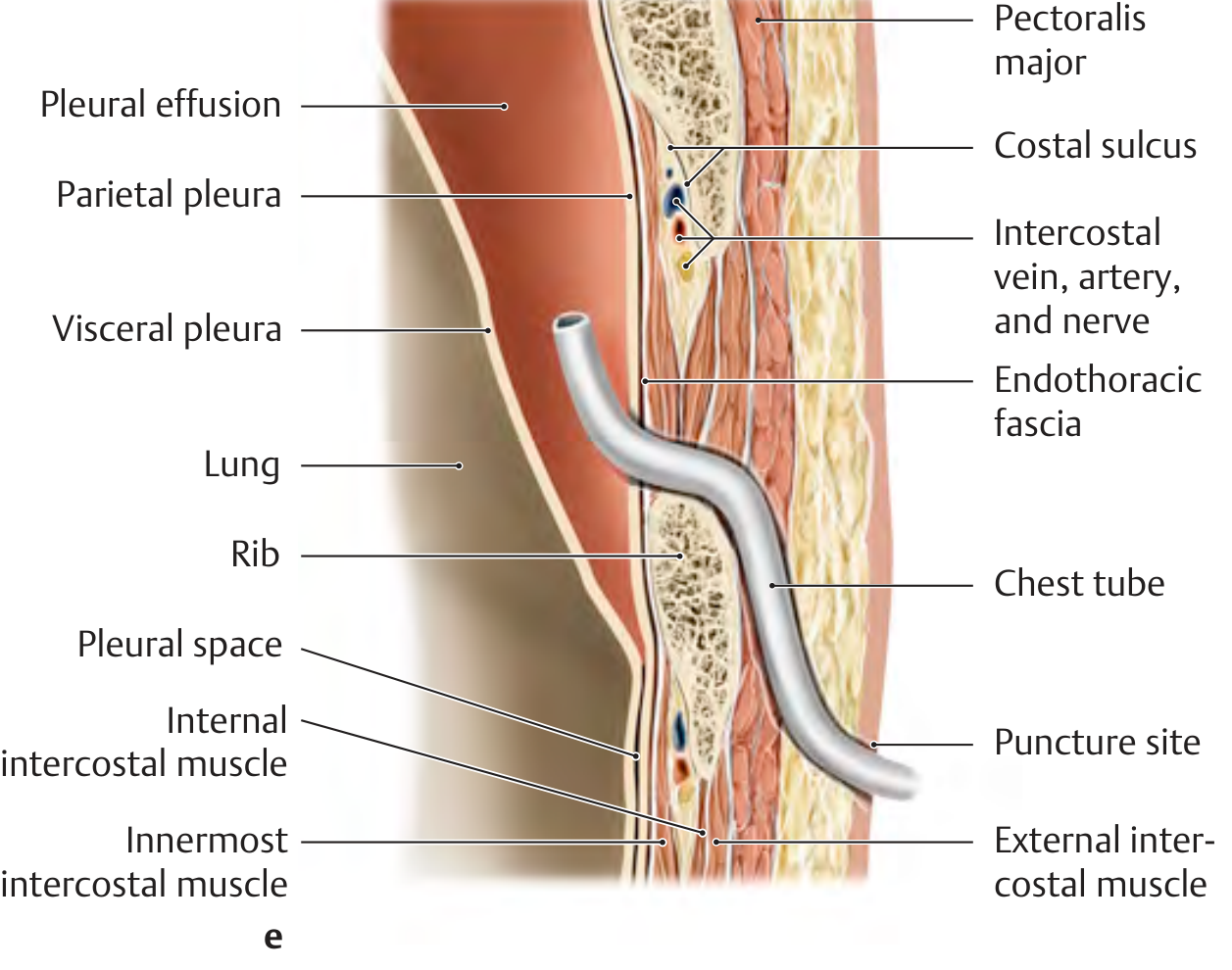
THIEME Atlas of General Anatomy - cross-section at the posterior axillary line showing all relevant layers
3. The Intercostal Neurovascular Bundle - Most Important Anatomical Point
Each intercostal space contains a neurovascular bundle running in the costal groove (costal sulcus) on the undersurface (inferior border) of each rib in the order (from above downward): Vein - Artery - Nerve (VAN).
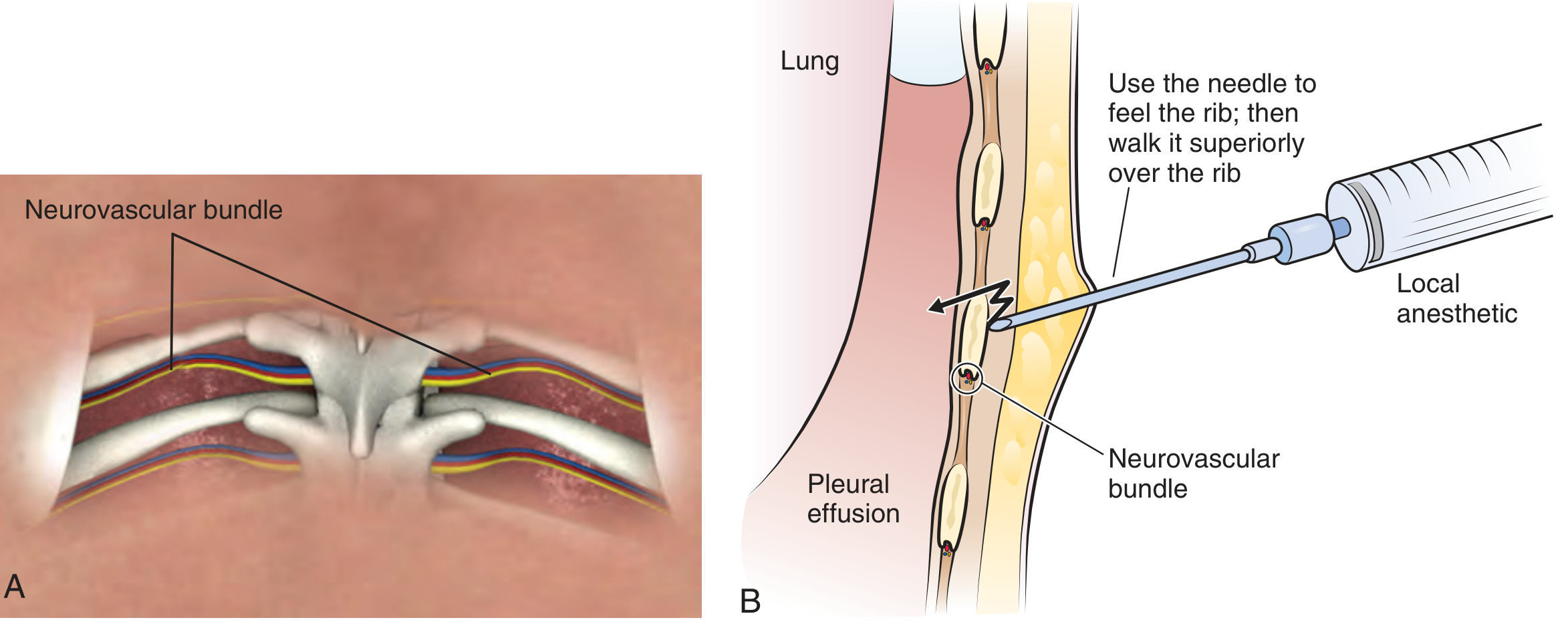
The needle MUST be inserted over the superior border (upper edge) of the lower rib of the chosen intercostal space - never along the inferior border of the upper rib, which risks lacerating the intercostal vessels and nerve, causing haemorrhage, haematoma, or neuralgia.
- Roberts and Hedges' Clinical Procedures in Emergency Medicine, p. 255
- THIEME Atlas of General Anatomy and Musculoskeletal System, p. 228
4. Layers the Needle Traverses
From outside to inside:
- Skin and subcutaneous fat
- Trapezius / serratus anterior / rhomboid muscles (depending on site)
- External intercostal muscle
- Internal intercostal muscle
- Innermost intercostal muscle
- Endothoracic fascia
- Parietal pleura - parietal pleura is highly pain-sensitive (innervated by intercostal nerves and phrenic nerve) - adequate local anaesthetic infiltration here is essential
- Pleural space - target
- Color Atlas of Human Anatomy Vol. 2, p. 224
5. Pleural Borders - Surface Anatomy
The pleural reflection levels are key to choosing a safe insertion site and avoiding subdiaphragmatic organ puncture:
| Line | Lung border | Pleural border |
|---|---|---|
| Midclavicular | 6th rib | 7th rib |
| Axillary | 8th rib | 9th rib |
| Scapular | 10th rib | 11th rib |
| Paravertebral | T10 spinous process | T11 spinous process |
The pleura extends 1-2 intercostal spaces below the lung border - this is the costodiaphragmatic recess.
Safe Site for Needle Entry
Classic Landmark Approach (Upright, Sitting Patient)
The patient sits upright leaning forward with arms resting on a table. Fluid sinks posteriorly and laterally.
Optimal insertion site for a free pleural effusion:
- 7th or 8th intercostal space on the posterior axillary line (or just medial to the scapular angle)
- The needle enters over the upper border of the lower rib
- Minimum 10 mm depth of fluid on ultrasound before attempting aspiration
Safe Triangle for Chest Drain (BTS guideline)
- Lateral border of pectoralis major
- Lateral border of latissimus dorsi
- Inferior boundary: horizontal line from the nipple (approximately 4th or 5th intercostal space)
- This is the axillary approach, used especially for chest drains
- Grainger & Allison's Diagnostic Radiology, p. 77
Critical Lower Limit
Do not insert below the 5th intercostal space anteriorly or below the 7th/8th intercostal space posteriorly. Lower than this risks crossing the pleural recess and penetrating:
- Liver (on the right)
- Spleen (on the left)
- Diaphragm
- Gray's Anatomy for Students, p. 283
Procedure Summary
- Confirm with ultrasound - all pleural aspirations should be US-guided; must confirm ≥10 mm fluid depth with no intervening lung at maximal inspiration
- Position - upright sitting, leaning forward
- Identify the rib - count from 2nd rib at the sternal angle downwards
- Local anaesthetic - infiltrate skin, subcutaneous tissue, intercostal muscles, and generously anaesthetize the periosteum of the rib and parietal pleura (extremely pain-sensitive)
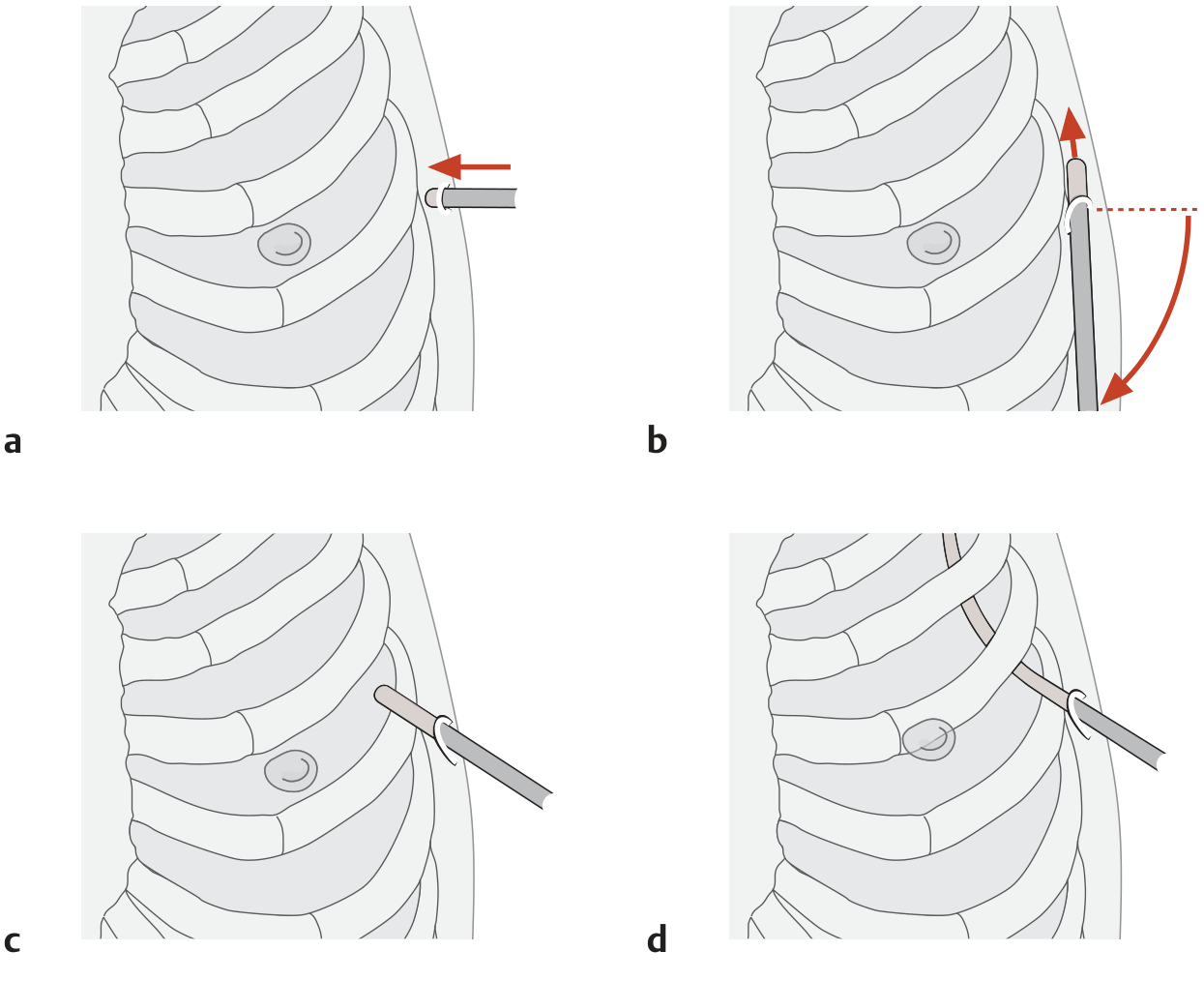
- Insert needle over the upper edge of the lower rib - "walk" the needle superiorly off the top of the rib to clear the neurovascular bundle
- Advance until a "pop" is felt on entering the pleural space; aspirate to confirm fluid
- Withdraw 50 mL (diagnostic) or up to 1.5 L (therapeutic) - do not exceed 1.5 L in a single session (risk of re-expansion pulmonary oedema)
Complications and Their Anatomical Basis
| Complication | Anatomical Basis |
|---|---|
| Pneumothorax (~5%) | Inadvertent lung puncture; highest risk in COPD |
| Haemorrhage / haematoma | Intercostal vessel (VAN bundle) laceration - needle too close to inferior rib border |
| Intercostal neuralgia | Nerve injury from the same bundle |
| Liver / spleen puncture | Needle inserted too inferiorly below the costodiaphragmatic recess |
| Diaphragmatic injury | Below safe lower limit |
| Re-expansion pulmonary oedema | Rapid removal of >1.5 L |
| Vasovagal reaction | Parietal pleura stimulation - keep atropine available |
| Infection / empyema | Breach of sterile technique |
- Grainger & Allison's Diagnostic Radiology, p. 77-78
- Roberts and Hedges' Clinical Procedures in Emergency Medicine, p. 256
Key Anatomical Rules to Remember
- Always over the top of the lower rib - to avoid the VAN bundle in the costal groove
- Never below the 5th space anteriorly / 8th space posteriorly - diaphragm, liver, spleen risk
- Parietal pleura = pain - anaesthetize it well; visceral pleura has no pain fibres
- Costodiaphragmatic recess = where fluid collects - aspirate here in the upright patient
- Pleural cupula projects into the neck - vulnerable in subclavian access
- US guidance is now standard - reduces complication rates significantly and accounts for fluid shifting between marking and aspiration
Sources: Roberts and Hedges' Clinical Procedures in Emergency Medicine; Grainger & Allison's Diagnostic Radiology; THIEME Atlas of General Anatomy and Musculoskeletal System; Gray's Anatomy for Students; Color Atlas of Human Anatomy Vol. 2 Internal Organs
this are performed posterior to the median glunaric line at one or more intercostal spaces below the fluid level with the patient in the sitting position but not below the ninth intercostal space, lest it may injure the diaphragm, the spleen on the left side and the liver on the right side. make it easy
Here's that point broken down simply:
Where to Insert the Needle (Posterior Approach)
Position
- Patient sits upright, leaning slightly forward
- Fluid sinks posteriorly by gravity - perfect for access
The Rule in Simple Terms
Behind the midscapular line + one or two spaces below the fluid level + never below the 9th intercostal space
Why Each Part Matters
| Rule | Why |
|---|---|
| Posterior to the midscapular line | Fluid collects here in the sitting patient - it's the most dependent (lowest) region posteriorly |
| One or more spaces below the fluid level | You need to be IN the fluid, not above it - going one space below the top of the fluid ensures you hit the collection, not the lung |
| NOT below the 9th intercostal space | Below this you risk hitting: diaphragm, spleen (left side), liver (right side) |
Visual Memory Aid
Fluid level (top of effusion)
↓
---- rib ---- ← skip this (too close to lung)
---- rib ---- ← INSERT HERE (1-2 spaces below fluid)
---- rib ----
---- 9th rib ---- ← STOP. Do not go below this
↓
Diaphragm / Liver / Spleen ← danger zone
The "Over the Top of the Rib" Rule
Once you've chosen the right space, the needle goes over the upper edge of the lower rib - because the intercostal vein, artery, and nerve (VAN) run under the rib above.
One-Line Summary
Sit the patient up, go behind the scapular line, one space below the fluid, over the top of the rib, and stop before the 9th space.
This is a shared conversation. Sign in to Orris to start your own chat.