pujo
"Pujo" — did you mean:
- Durga Puja — the Bengali Hindu festival?
- A specific topic (e.g., puja rituals, preparation, history)?
- Something else entirely?
What would you like to know?
PUJO in surgery
Reading File
Finding Sources
Searching the Web
PUJO surgery medical term meaning
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Here is a comprehensive overview of PUJO (Pelvi-Ureteric Junction Obstruction) in surgery:
PUJO — Pelvi-Ureteric Junction Obstruction
PUJO stands for Pelvi-Ureteric Junction Obstruction (also written PUJ Obstruction). It is an obstruction to urine flow from the renal pelvis into the ureter at the pelvi-ureteric junction.
Incidence
- Most common cause of unilateral hydronephrosis
- Incidence: 1 in 500 live births
- More common in males and on the left side
- Bilateral in 10% of cases
Etiology / Causes
- Intrinsic obstruction — aperistaltic segment at the PUJ due to muscular hypoplasia (most common)
- High insertion of the ureter into the renal pelvis
- Crossing aberrant (polar) vessels at the PUJ
Clinical Presentation
| Age Group | Presentation |
|---|---|
| Antenatal / Neonates | Detected on antenatal USS; palpable flank mass |
| Children | Intermittent flank pain, UTI, flank mass |
| Adults | Back/flank pain, recurrent pyelonephritis |
| Any age | Dietl's crisis — severe flank pain after large fluid intake, relieved by passing large amounts of urine |
Investigations
| Investigation | Findings |
|---|---|
| Ultrasound | Symmetrical hydronephrosis, dilated renal pelvis, parenchymal thickness, cortical echogenicity |
| Isotope diuretic renography (DTPA/MAG3) | Investigation of choice — renogram curve; T½max >20 min after furosemide = obstruction |
| CTU / MRU | Used for further anatomical evaluation |
Renogram — Obstructive Pattern:
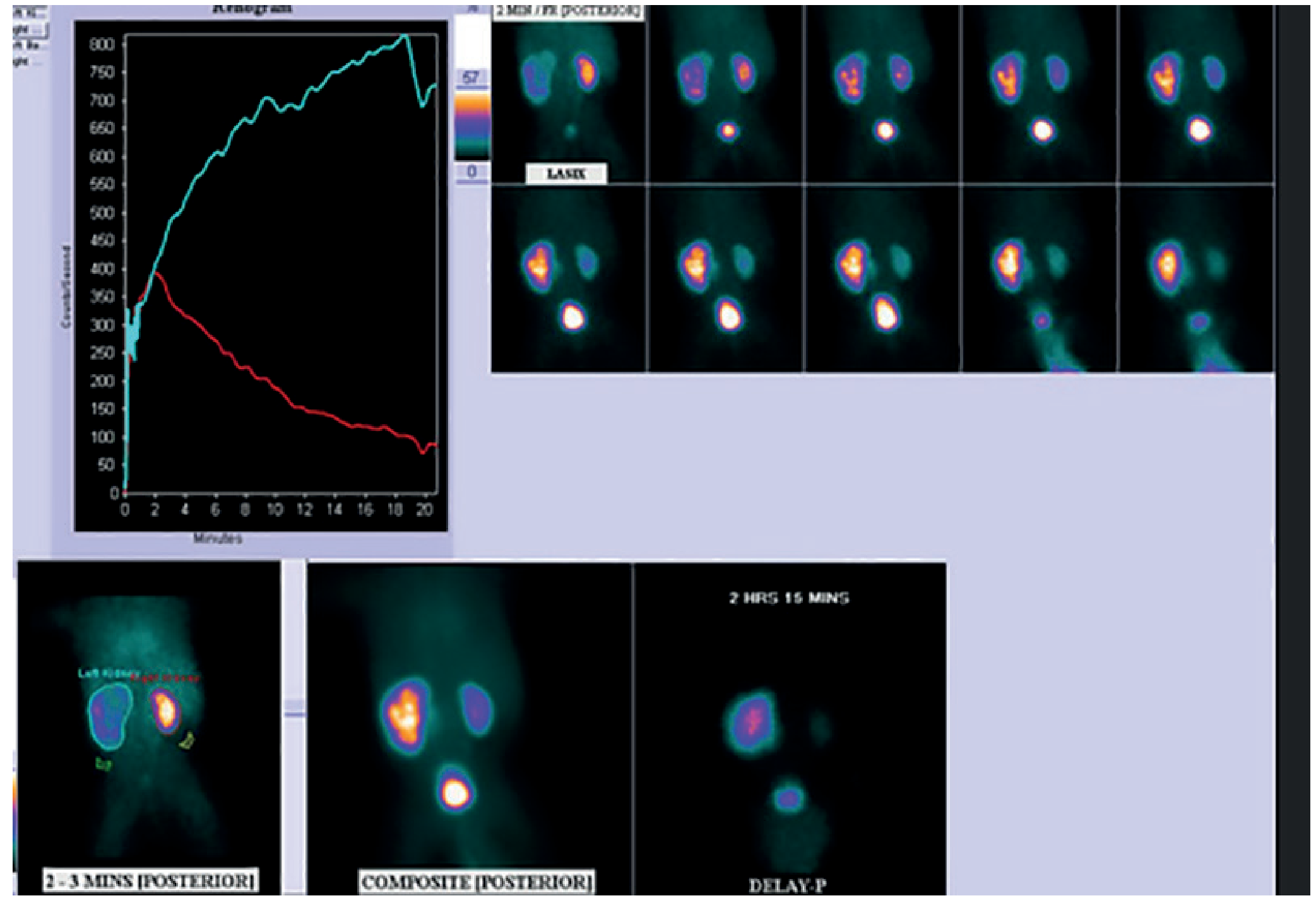
Criteria for significant obstruction (indication for surgery):
- Rising renogram curve after furosemide
- T½max > 20 minutes
- Differential function < 40% on the affected side
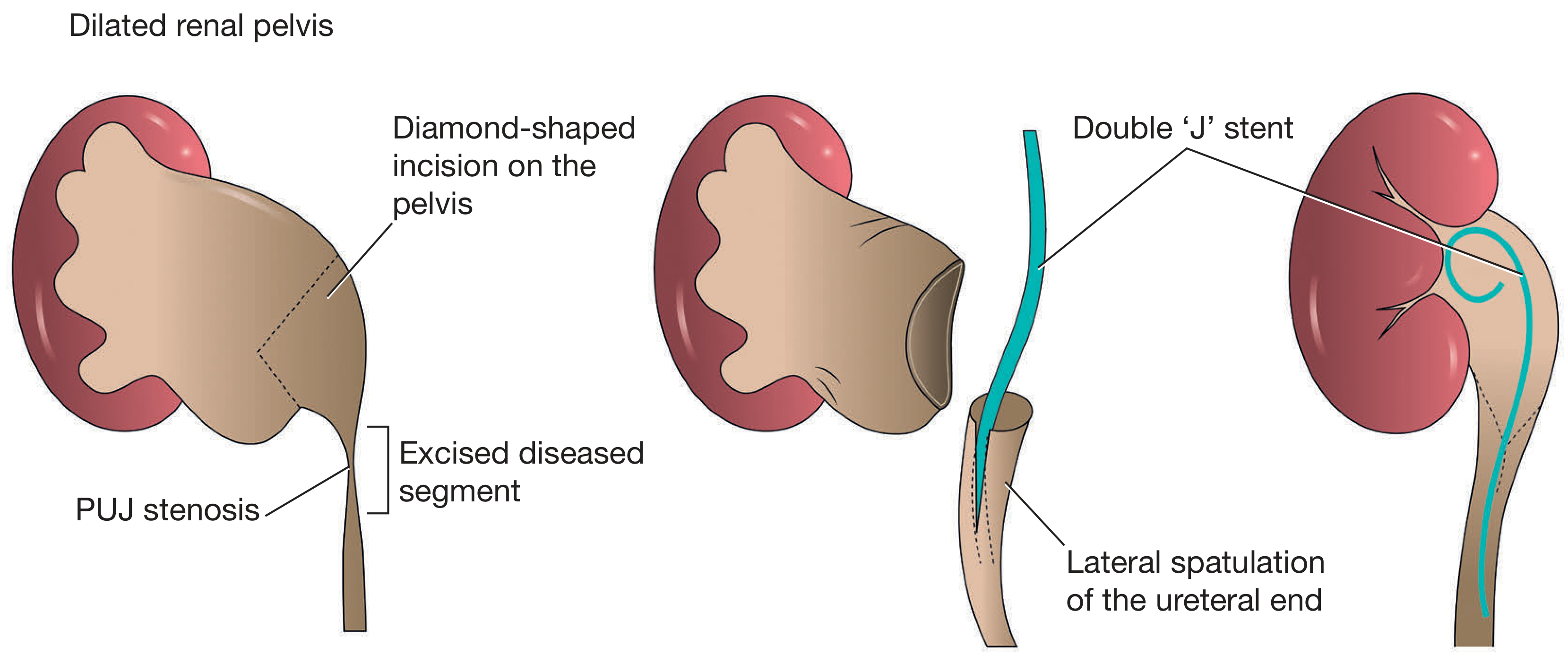
Surgical Treatment
Anderson–Hynes Dismembered Pyeloplasty
The procedure of choice.
Prerequisites of a good pelvi-ureteric anastomosis:
- Dependent
- Wide
- Funnel-shaped
- Good vascularity maintained
- Without tension
- Redundant pelvis excised
Indications for pyeloplasty:
- Persistent pain
- Hypertension
- Haematuria
- Secondary renal calculi
- Recurrent UTIs
Steps of Open Dismembered Pyeloplasty:
Endoscopic Management
- Endopyelotomy is reserved for post-pyeloplasty strictures (not the primary treatment)
Associations
PUJO is associated with:
- Horseshoe kidney (increased incidence of PUJO + stone formation)
- Ureteral duplication
- Multicystic dysplastic kidney (MCDK) — MCDK is the 2nd most common cause of abdominal mass in newborns after hydronephrosis due to PUJO
— Bailey and Love's Short Practice of Surgery, 28th Edition, Ch. 82
This is a shared conversation. Sign in to Orris to start your own chat.