Describe anatomy of airway and tracheobronchial tree, emphasize on the structures relevant to airway management and endotracheal intubation.
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Finding Sources
I have all the key content and images needed. Now I have comprehensive material from Miller's Anesthesia (10th ed) and Morgan & Mikhail's Clinical Anesthesiology (7th ed) to compose a thorough, well-illustrated answer. Let me now write the full response.
Anatomy of the Airway and Tracheobronchial Tree
Sources: Miller's Anesthesia 10th ed; Morgan & Mikhail's Clinical Anesthesiology 7th ed; Barash Clinical Anesthesia 9th ed; Roberts & Hedges' Clinical Procedures in Emergency Medicine
The airway is divided into the upper airway (nasal cavity, oral cavity, pharynx, and larynx) and the lower airway (tracheobronchial tree). A detailed command of this anatomy underpins every aspect of airway management - from mask ventilation and laryngoscopy to surgical rescue airways.
1. Nasal Cavity
The airway begins functionally at the naris. The nasal cavity is divided into right and left fossae by the nasal septum (septal cartilage anteriorly; ethmoid superiorly and vomer inferiorly posteriorly). The lateral walls bear three turbinates (conchae) - inferior, middle, and superior - that divide the passage into corresponding meatuses.
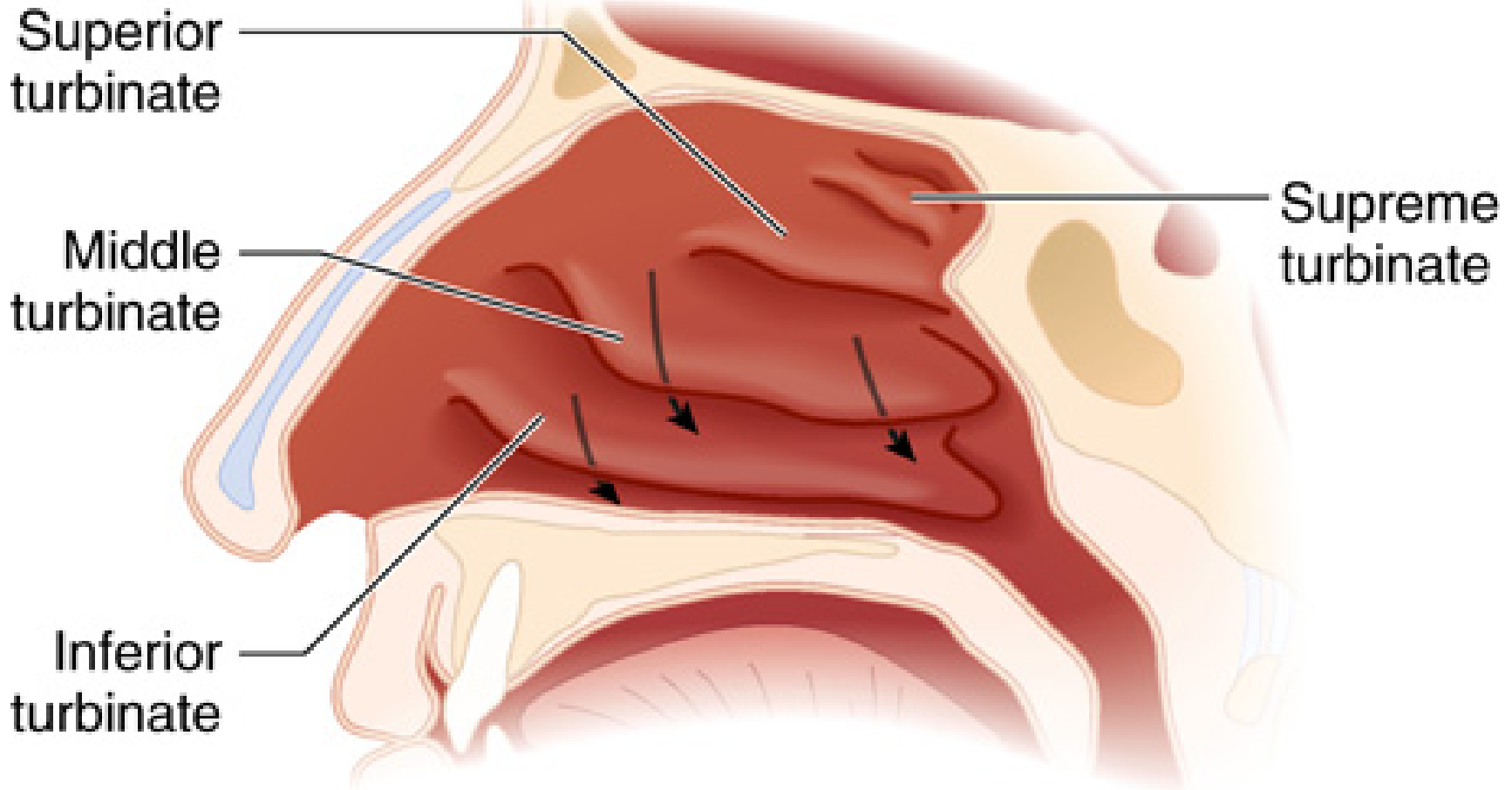
Clinically relevant points:
- The inferior meatus (between inferior turbinate and floor) is the preferred pathway for nasopharyngeal airways and nasotracheal tubes. Instruments placed elsewhere risk avulsing a turbinate.
- Nasal septal deviation is common in adults; always determine the more patent side before instrumentation.
- The cribriform plate (roof of the nasal cavity) is fragile; fracture creates a nasal-intracranial communication. Nasotracheal tubes are contraindicated with suspected basilar skull fractures.
- The mucosa is richly vascular. Topical vasoconstrictors (e.g., oxymetazoline or cocaine) must be applied before any nasal instrumentation to prevent epistaxis.
- The posterior openings, the choanae, lead into the nasopharynx.
- Miller's Anesthesia 10th ed, p. 5836
2. Oral Cavity
The mouth is the primary conduit for airway devices because nasal passage size and trauma risk limit nasal use.
- Mouth opening requires rotation within the temporomandibular joint (TMJ) followed by anterior sliding (subluxation) of the mandibular condyles. Restricted TMJ mobility (trismus, ankylosis, masseter hypertrophy) limits laryngoscopy blade insertion depth.
- The tongue is anchored by the genioglossus to the mandible. The jaw-thrust maneuver exploits this attachment - pulling the mandible forward pulls the tongue off the posterior pharyngeal wall, relieving obstruction.
- The mylohyoid muscle separates the sublingual space (superior) from the submental space (inferior). Infection or hematoma in these spaces (Ludwig's angina) displaces the tongue posteriorly, causing severe airway obstruction.
- The oral cavity leads into the oropharynx, bounded inferiorly by the tongue and superiorly by the hard and soft palates.
- Miller's Anesthesia 10th ed, p. 5837
3. Pharynx
The pharynx is a muscular tube extending from the base of skull to the level of the cricoid cartilage, connecting the nasal and oral cavities to the larynx and esophagus.
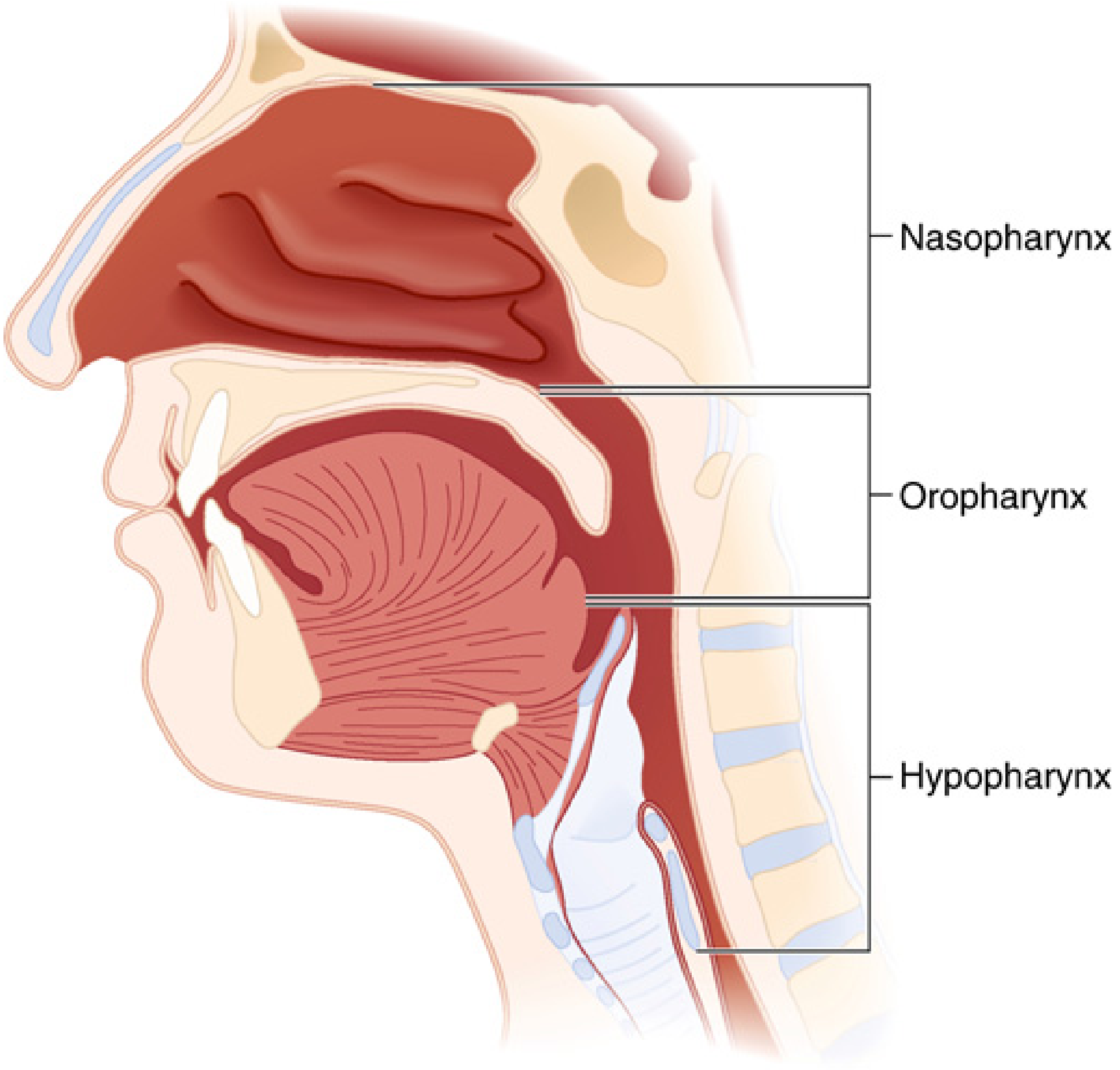
It has three regions:
| Region | Boundaries | Clinical Notes |
|---|---|---|
| Nasopharynx | Base of skull → soft palate | Contains adenoid tonsils (can obstruct nasal airway devices when enlarged); velopharynx (soft palate level) = common site of obstruction in anesthetized patients |
| Oropharynx | Soft palate → tip of epiglottis | Contains palatine tonsils in anterior/posterior tonsillar pillars; base of tongue lies anteriorly; vallecula = space between tongue base and epiglottis (tip of curved laryngoscope blade seats here) |
| Hypopharynx | Tip of epiglottis → inferior cricoid border | Contains the laryngeal inlet anteriorly and piriform sinuses (fossae) laterally |
Pharyngeal muscle tone in the awake patient maintains airway patency. Loss of tone under anesthesia is the primary mechanism of upper airway obstruction. A chin lift with mouth closure increases longitudinal tension in pharyngeal muscles, counteracting collapse.
The posterior pharyngeal wall is covered by the buccopharyngeal fascia, separating it from the retropharyngeal space. Inadvertent force during tube passage can lacerate this fascia and cause retropharyngeal dissection.
- Miller's Anesthesia 10th ed, p. 5838-5839
4. Larynx - The Critical Gateway
The larynx is the most anatomically complex structure relevant to intubation. It extends from the tip of the epiglottis to the inferior border of the cricoid cartilage (C3-C6 in adults, C4-C6; higher in infants at C3-C5).
4.1 Cartilaginous Framework
The laryngeal skeleton has nine cartilages (three unpaired, three paired):
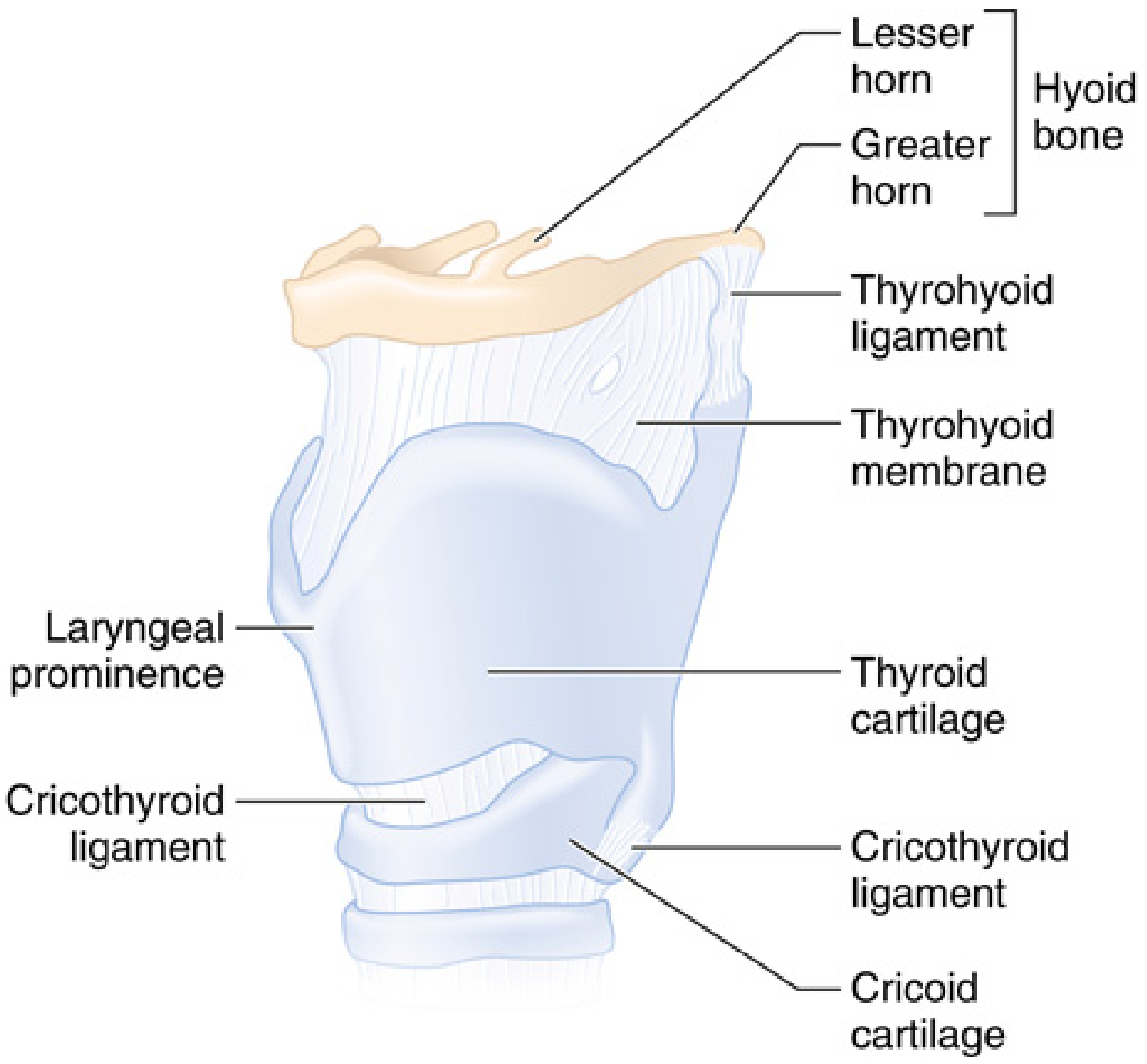
Unpaired:
- Thyroid cartilage - the largest cartilage; shield-shaped; forms the anterior "protective housing" of the vocal mechanism. The superior thyroid notch (Adam's apple/laryngeal prominence) is the key anterior neck landmark - palpated to identify midline and locate the cricothyroid membrane. Lies at approximately the level of C4-C5.
- Cricoid cartilage - the only complete cartilaginous ring in the airway. Lies at C6. Forms the inferior limit of the larynx. Anteriorly connected to thyroid cartilage by the cricothyroid membrane. Its signet-ring shape (narrow anteriorly, wider posteriorly) provides circumferential support. It is the narrowest point of the pediatric airway (making uncuffed ETTs appropriate in children); in adults, the glottic opening is the narrowest.
- Epiglottis - a leaf-shaped cartilaginous flap forming the anterior border of the laryngeal inlet. Its anterior surface connects to the hyoid bone via the hyoepiglottic ligament and to the base of tongue by the glossoepiglottic folds, creating the paired valleculae. The tip of the curved Macintosh blade seats in the vallecula; indirect pressure on the hyoepiglottic ligament lifts the epiglottis anteriorly to expose the glottis.
Paired:
- Arytenoid cartilages - articulate with the posterior surface of the cricoid; serve as the posterior attachments of the vocal cords. Their movement (abduction/adduction) controls glottic aperture.
- Corniculate cartilages - sit atop the arytenoids; visible during laryngoscopy as the posterior cartilaginous prominences at the laryngeal inlet.
- Cuneiform cartilages - embedded in the aryepiglottic folds; create the lateral prominences seen during laryngoscopy.
4.2 Membranes and Ligaments
- Thyrohyoid membrane - connects the thyroid cartilage to the hyoid bone superiorly; the internal branch of the superior laryngeal nerve (SLN) pierces it to provide sensory supply to the supraglottic mucosa.
- Cricothyroid membrane (CTM) - connects the inferior edge of thyroid cartilage to the superior surface of the cricoid cartilage. This is the emergency surgical airway access point.
- Dimensions: ~8-12 mm wide, 10.4-13.7 mm in height (Barash)
- Located 1-1.5 fingerbreadths below the laryngeal prominence
- Composed of yellow elastic tissue lying directly beneath the skin and a fascial layer - minimal subcutaneous fat in most patients, making it relatively accessible
- Any incision or needle puncture should be made in the inferior third and directed posteriorly to avoid the vocal folds (0.9 cm above the upper border of the membrane) and the cricothyroid arteries (running along the superior border)
- Ultrasound guidance improves identification, especially in obese patients; only ~one-third of trainees correctly identify the CTM by palpation alone
- Barash Clinical Anesthesia 9th ed, p. 2295
4.3 Laryngeal Inlet and Interior
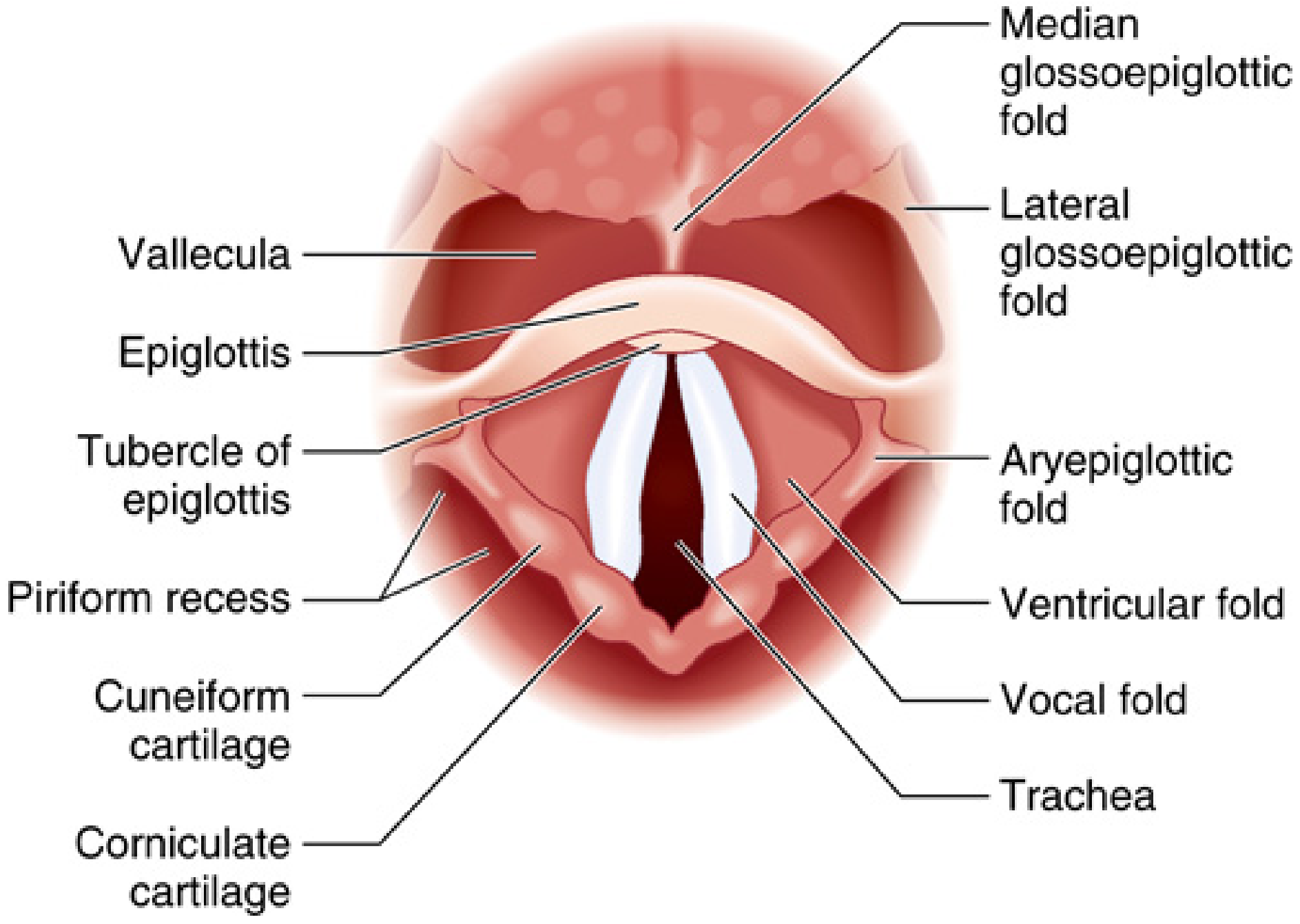
The laryngeal inlet is bounded:
- Anterosuperiorly: epiglottis
- Laterally: aryepiglottic folds (containing cuneiform and corniculate cartilages)
- Posteriorly: arytenoid cartilages and interarytenoid notch
The piriform sinuses (fossae) lie on either side of the laryngeal inlet, between the aryepiglottic folds and the thyroid cartilage. During laryngoscopy they appear as dark recesses on each side of the laryngeal opening; passage of an ETT into a piriform sinus is a recognized error.
From superior to inferior, the laryngeal cavity contains:
- Vestibule - from the laryngeal inlet down to the false vocal cords
- Ventricular folds (false vocal cords) - superior folds, not involved in phonation; they have no active function in normal respiration
- Ventricles - lateral recesses between the false and true cords
- True vocal cords (vocal folds) - pearlescent white bands extending from the thyroid cartilage anteriorly (anterior commissure) to the arytenoids posteriorly; they contain the vocalis muscle
- Glottis - the space between the true vocal cords; the anatomically narrowest point of the adult larynx
- Subglottis - below the vocal cords to the inferior border of the cricoid
- Miller's Anesthesia 10th ed, p. 5844
4.4 Laryngeal Innervation - Critical for Airway Blocks
Both sensory and motor supply derive from the vagus nerve (CN X) via two branches:
| Nerve | Course | Sensory supply | Motor supply |
|---|---|---|---|
| Superior laryngeal nerve (SLN) | Divides into internal and external branches at the hyoid | Internal branch: supraglottic mucosa (epiglottis, vallecula, aryepiglottic folds, above vocal cords); enters via thyrohyoid membrane | External branch: cricothyroid muscle only |
| Recurrent laryngeal nerve (RLN) | Loops under subclavian artery (right) or aortic arch (left) | Subglottic and tracheal mucosa (below vocal cords) | All intrinsic laryngeal muscles except cricothyroid |
Clinical significance:
- For awake intubation, the SLN internal branch is blocked with injection at the greater cornu of the hyoid, and the RLN is blocked via transtracheal injection of local anesthetic, or topical spray below the cords.
- Unilateral RLN injury causes hoarseness (paralyzed cord remains adducted at midline/paramedian position); the protective role against aspiration may also be compromised.
- Bilateral RLN injury causes complete airway obstruction by unopposed adduction of both cords; requires emergency airway.
- The cricothyroid muscle (innervated by the external SLN) is the tensor of the vocal cords - it is the only intrinsic laryngeal muscle not affected by RLN injury.
- Barash Clinical Anesthesia 9th ed, p. 2295
5. Trachea
The trachea begins at the inferior border of the cricoid cartilage (C6) and extends to the carina at the level of T4-T5 (sternal angle of Louis). Length: 10-15 cm in adults (Miller); 10-13 cm (Morgan & Mikhail).
Structure:
- 16-20 C-shaped cartilaginous rings, open posteriorly
- The anterior and lateral walls are supported by cartilage; the posterior wall is the trachealis muscle (smooth muscle connecting the ends of the C-rings)
- The cricoid cartilage is the narrowest part: average diameter 17 mm in men, 13 mm in women
Key intubation dimensions (Morgan & Mikhail):
- Average tracheal length: 10-13 cm
- Lumen narrows slightly toward the carina
- ETT tip should lie at least 2 cm above the carina to avoid endobronchial intubation but below the vocal cords
Relationships:
- The trachea is a midline structure in the neck, flanked by the thyroid gland
- Anterior surface of tracheal rings is subcutaneous in the neck, accessible for surgical or percutaneous tracheostomy
- The esophagus lies immediately posterior to the trachealis muscle
6. Tracheobronchial Tree
At the carina (T4-T5), the trachea bifurcates into the right and left mainstem bronchi.
Right vs. Left Mainstem Bronchus
| Feature | Right Mainstem Bronchus | Left Mainstem Bronchus |
|---|---|---|
| Angle from trachea | More vertical (~25°) - more in-line with trachea | More obtuse (~45°) |
| Length | Shorter (~2 cm before RUL take-off); ~2.0 cm in men, ~1.5 cm in women to RUL | Longer: ~5.0 cm in men, ~4.5 cm in women |
| Consequence | Foreign bodies and malpositioned ETTs preferentially enter here | ETT rarely passes here unless deeply advanced |
| Right upper lobe | Takes off just ~2 cm from carina (1 in 250 people has a "tracheal bronchus" emerging above carina) | - |
Intubation implication: After intubation, confirm bilateral breath sounds - diminished breath sounds on the left with dullness on the left suggest right mainstem intubation. The ETT cuff should ideally sit 2-3 cm below the cords and 2+ cm above the carina.
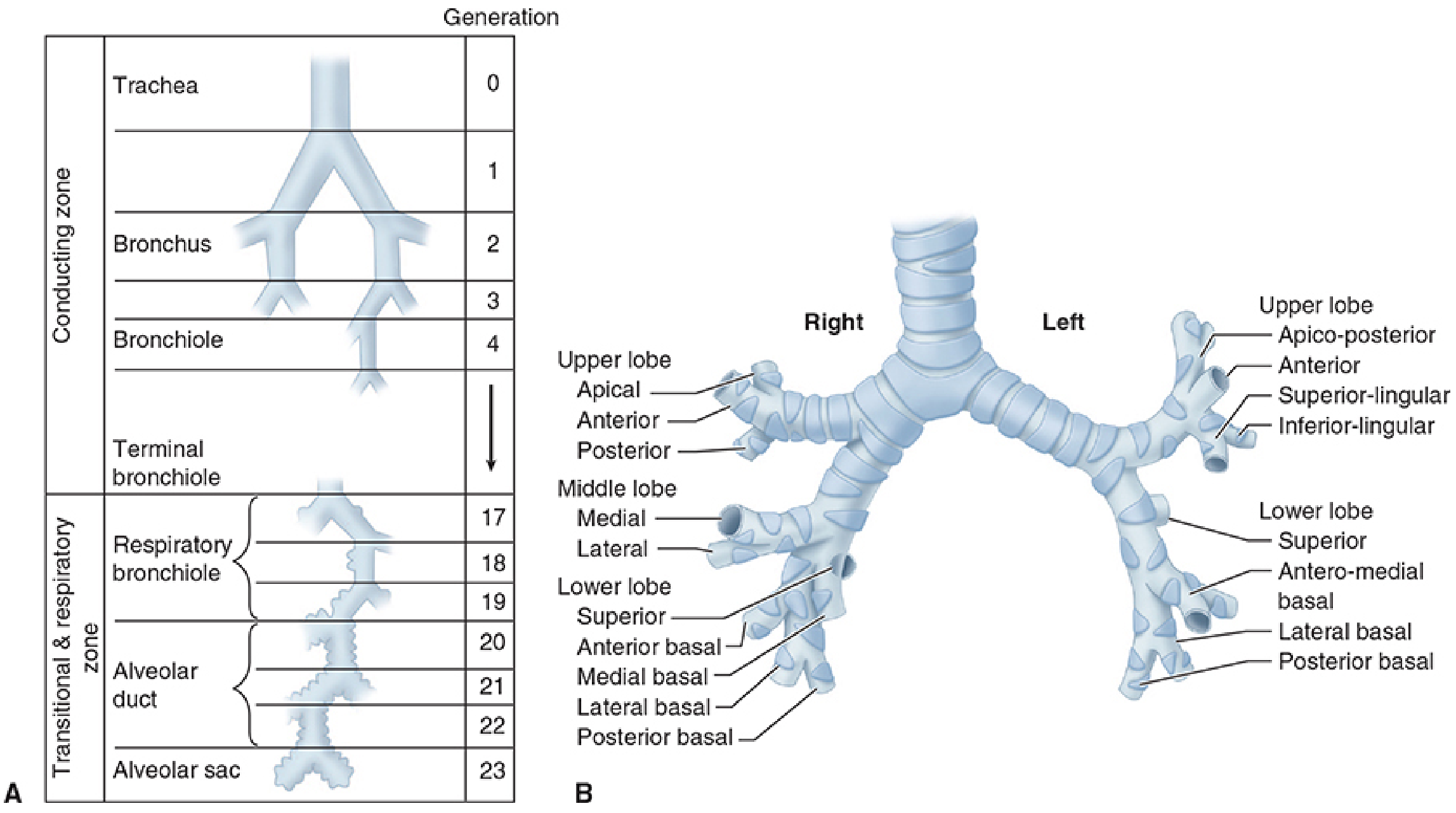
Airway Generations (Weibel Model)
Starting from the trachea (Generation 0) to alveolar sacs (Generation 23):
- Generations 0-16 = Conducting zone (no gas exchange): trachea → mainstem bronchi → lobar bronchi → segmental bronchi → bronchioles → terminal bronchioles
- Generations 17-19 = Respiratory bronchioles (first alveoli appear in walls; gas exchange begins)
- Generations 20-22 = Alveolar ducts
- Generation 23 = Alveolar sacs (~17 alveoli each)
Each generation approximately doubles the number of airways. Total: 300-500 million alveoli providing 50-100 m² of gas-exchange surface area.
Wall structure changes progressively:
- Ciliated columnar epithelium in trachea → cuboidal in bronchioles → flat alveolar epithelium
- Cartilaginous support disappears at the bronchiolar level (generation ~11)
- Smooth muscle remains throughout, providing the substrate for bronchoconstriction
- Morgan & Mikhail Clinical Anesthesiology 7th ed, p. 911-912
7. Summary Table: Structures and Their Intubation Relevance
| Structure | Intubation Relevance |
|---|---|
| Inferior turbinate | Nasal airway/nasotracheal tube pathway; vasoconstriction required |
| Nasal septum | Deviated septum → identify more patent nostril |
| Temporomandibular joint | Restricted opening limits laryngoscope insertion |
| Genioglossus/mandible | Target of jaw thrust; forward mandible displacement relieves obstruction |
| Vallecula | Tip of Macintosh blade seats here to lift epiglottis |
| Epiglottis | Lifted by direct contact (Miller blade) or vallecula pressure (Macintosh) |
| Hyoepiglottic ligament | Mechanism of indirect epiglottis elevation by curved blade |
| Aryepiglottic folds / Piriform sinus | Piriform fossae must not receive the ETT tip |
| True vocal cords (glottis) | Visual target for ETT passage; narrowest adult airway point |
| Anterior commissure | ETT tip directed slightly posteriorly to pass without catching |
| Subglottis / Cricoid | Narrowest pediatric airway point; ETT leak pressure guides sizing |
| Cricothyroid membrane | Emergency surgical/needle airway access |
| Carina (T4-T5) | ETT tip must stay ≥2 cm above; carina stimulation causes cough/bronchospasm |
| Right mainstem bronchus | Site of inadvertent endobronchial intubation |
| Recurrent laryngeal nerve | At-risk during thyroid/cervical surgery; injury causes cord paralysis |
| Superior laryngeal nerve (internal branch) | Blocked for awake intubation (supraglottic anesthesia) |
8. Infant vs. Adult Airway - Key Differences
Per Barash Clinical Anesthesia (Table 28-1):
| Feature | Infant | Adult |
|---|---|---|
| Larynx level | C3-C5 | C4-C6 |
| Laryngeal shape | Funnel-shaped (narrowest at subglottis/cricoid) | Cylindrical (narrowest at glottis) |
| Epiglottis | Longer, omega-shaped, angled at 45° | Flatter, horizontal |
| Narrowest point | Cricoid (subglottic) | Glottis |
| Cartilages | More pliable | Calcified with age |
| Implications | Uncuffed ETTs acceptable; straight blade preferred | Cuffed ETTs required; curved blade often preferred |
All content sourced from:
- Miller's Anesthesia 10th ed - Chapter 40, Functional Airway Anatomy (pp. 5835-5845)
- Morgan & Mikhail's Clinical Anesthesiology 7th ed - Chapter 23, Tracheobronchial Tree (pp. 911-912)
- Barash Clinical Anesthesia 9th ed - Chapter 28, Review of Airway Anatomy (p. 2295)
- Roberts & Hedges' Clinical Procedures in Emergency - Chapter 4, Airway Anatomy
This is a shared conversation. Sign in to Orris to start your own chat.