Glaucoma and anterior uvietus
Reading File
Finding Sources
Finding Sources
Searching PubMed
"uveitic glaucoma" AND "anterior uveitis"
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content. Let me compile a thorough, well-organized answer.
Glaucoma and Anterior Uveitis
Anterior Uveitis — Overview
Anterior uveitis is inflammation of the iris and anterior ciliary body (pars plicata) and is the most common form of uveitis. It is subdivided into:
- Acute anterior uveitis (AAU) — rapid onset, usually unilateral; HLA-B27-related and idiopathic forms predominate
- Chronic anterior uveitis (CAU) — more likely bilateral, associated with systemic disease, often granulomatous
Interleukin-6 (released by monocytes/macrophages in response to inflammatory cytokines) plays a central role in the aberrant immune response.
Systemic Associations (Table 12.1)
| Category | Key Conditions |
|---|---|
| Idiopathic | ~50% of AAU |
| Infectious | VZV (ophthalmic zoster), TB, syphilis, Lyme disease |
| Non-infectious | HLA-B27 (~20% of AAU), JIA, sarcoidosis, Behçet, SLE, MS, IBD-associated |
| Masquerade | Lymphoma, anterior segment melanoma, juvenile xanthogranuloma |
Clinical Features
Symptoms of AAU: rapid-onset unilateral pain, photophobia, visual loss, redness, watery discharge. Recurrences are common, especially in HLA-B27 and idiopathic disease.
Key slit-lamp signs:
- Miosis — pupillary sphincter spasm; predisposes to posterior synechiae
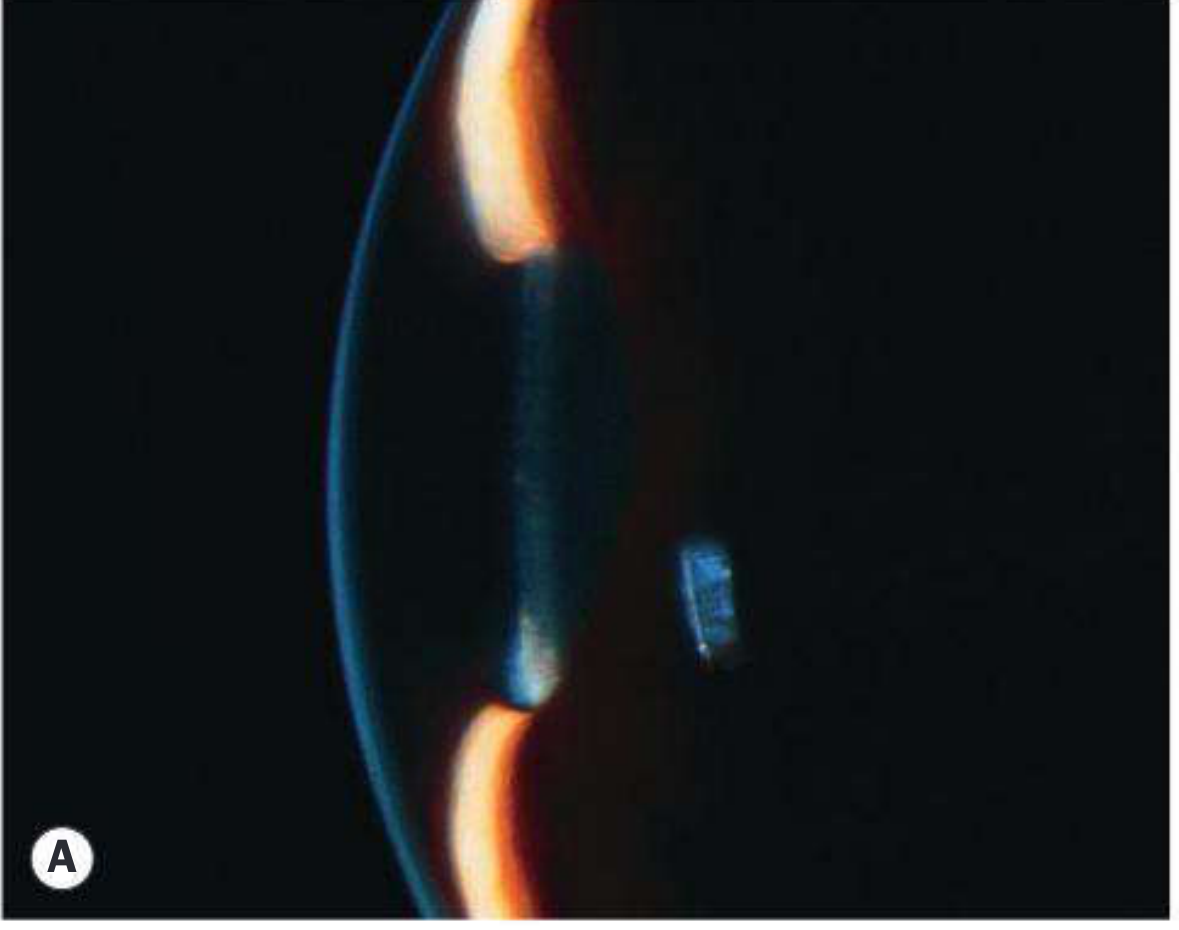
- Anterior chamber cells — graded per SUN Working Group (1×1 mm slit beam)
- Aqueous flare — protein leakage through breakdown of blood-aqueous barrier; even without cells, persistent flare indicates active inflammation and higher complication risk
- Hypopyon — horizontal layering of cells; immobile/fibrin-rich in HLA-B27; shifts with head position in Behçet disease
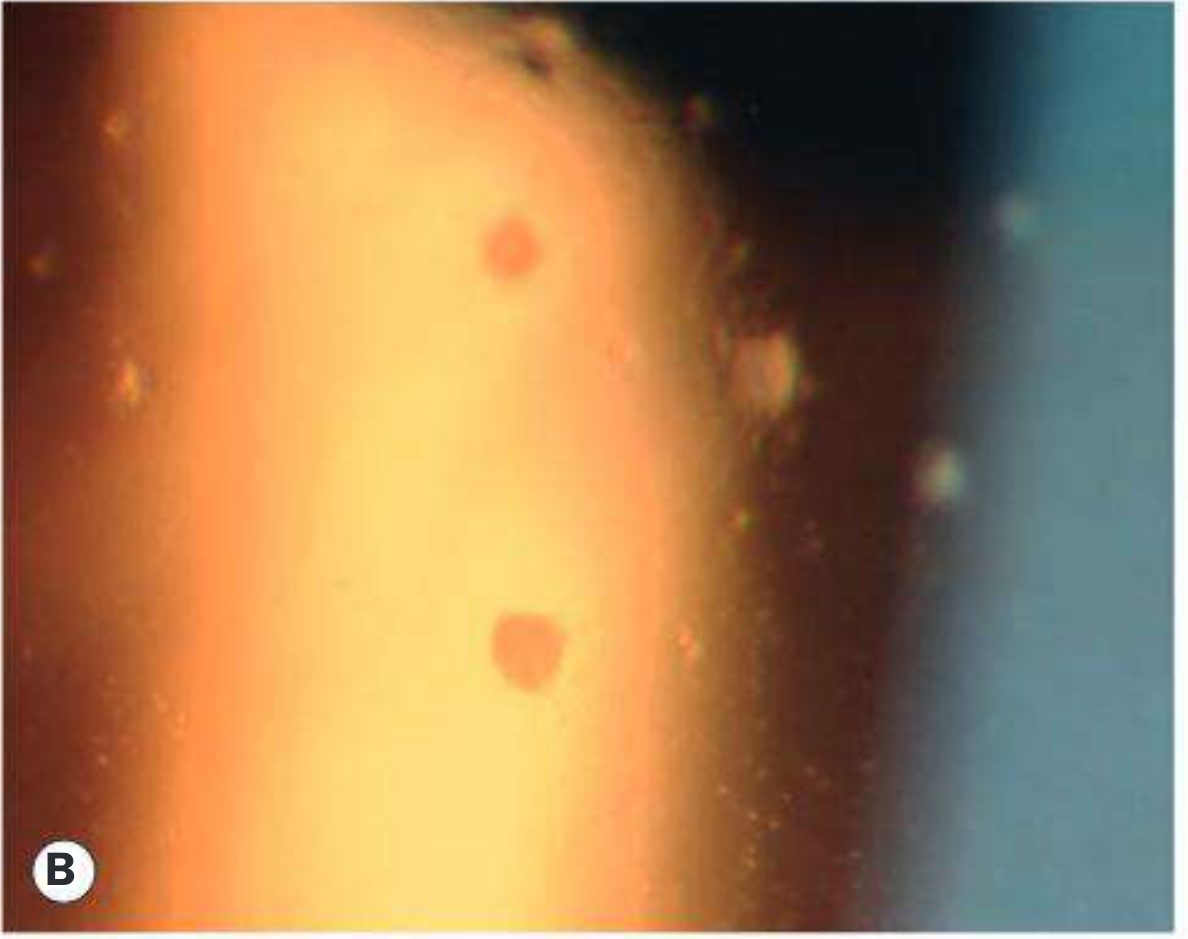
- Keratic precipitates (KP) — inferior Arlt triangle distribution
- Small KP — non-granulomatous (AAU)
- Mutton-fat KP — large, greasy; granulomatous (sarcoid, TB)
- Stellate KP — Fuchs uveitis syndrome
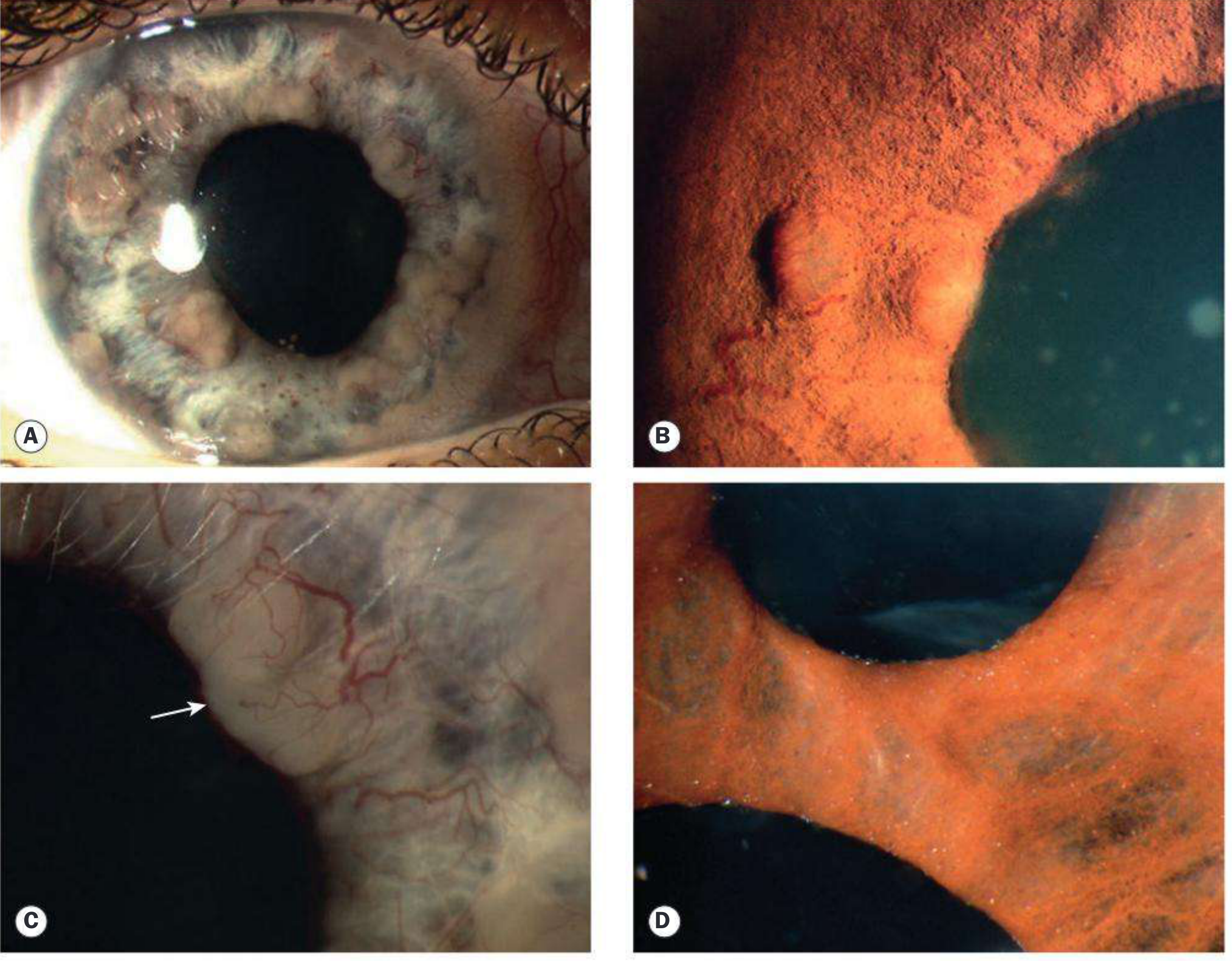
- Iris nodules: Busacca (stromal, granulomatous) and Koeppe (pupillary margin, site of posterior synechiae)
- Fibrinous exudate — severe AAU, especially HLA-B27
- Posterior synechiae (PS) — adhesions between iris and anterior lens capsule; may progress to seclusio pupillae (360° PS)
Treatment of Anterior Uveitis
- Topical corticosteroids — mainstay (e.g., prednisolone acetate 1%), tapered as inflammation resolves
- Cycloplegics (e.g., cyclopentolate, atropine) — relieve ciliary spasm, prevent posterior synechiae, reduce pain
- Periocular depot steroids — rule out infectious aetiology before use
- Systemic steroids — for severe/refractory cases or bilateral disease
- Systemic management per underlying condition (see below)
- Treat secondary glaucoma — see next section; avoid pilocarpine
Etiology-specific additions:
- Ankylosing spondylitis/HLA-B27: systemic NSAIDs (naproxen), rheumatology referral
- JIA: minimize topical steroids long-term (↑ risk of cataract and glaucoma in children); systemic steroids risk growth suppression
- Herpetic uveitis (HSV/VZV): oral antivirals (acyclovir, valacyclovir, famciclovir) + topical steroids; topical antivirals are insufficient for uveitis due to poor intraocular penetration
- IBD: systemic steroids, sulfadiazine, or other immunosuppressives
Secondary Glaucoma in Anterior Uveitis
This is the most important complication. Prevalence increases with chronicity and severity of uveitis. It is particularly common in Fuchs uveitis syndrome and CAU associated with JIA.
Mechanisms
1. Open-Angle Mechanisms
| Condition | Mechanism |
|---|---|
| Acute anterior uveitis | Trabecular obstruction by inflammatory cells/debris; aqueous viscosity ↑ from protein leakage |
| Acute trabeculitis | Oedema/inflammation of trabecular meshwork → reduced outflow; particularly with HSV, VZV, toxoplasma |
| Chronic anterior uveitis | Trabecular scarring/sclerosis from chronic trabeculitis |
| Steroid response | Topical corticosteroids elevate IOP (steroid-response glaucoma) |
2. Angle-Closure Mechanisms
| Type | Mechanism |
|---|---|
| With pupillary block | 360° posterior synechiae (seclusio pupillae) → aqueous trapped in posterior chamber → iris bombé → peripheral iris occludes trabeculum + PAS formation |
| Without pupillary block | Inflammatory cells/debris deposited in angle → organisation and contraction pulls peripheral iris over trabeculum → progressive synechial (PAS) angle closure |
| Neovascular glaucoma | Iris neovascularization → secondary angle closure |
Diagnostic Dilemmas
- IOP fluctuation can be dramatic — phasing is helpful in borderline cases
- Ciliary body shutdown during acute uveitis flares lowers IOP, masking underlying glaucoma; as inflammation subsides and ciliary body function returns, IOP may spike
- Even eyes with IOP of 30–35 mmHg may become hypotonous during acute exacerbations
- Intermittent topical steroids cause fluctuating IOP
- Iris vessels can mimic neovascular glaucoma
- Glaucomatous damage may be hard to assess with small pupils or media opacities
Medical Treatment of Uveitic Glaucoma
| Drug Class | Notes |
|---|---|
| Beta-blocker | Drug of first choice |
| Alpha-adrenergic agonist / topical CAI | Second-line for moderate IOP elevation (<35 mmHg without significant disc damage) |
| Oral acetazolamide | If IOP very high |
| Prostaglandin analogues | Avoid if possible — may promote inflammation; try if other agents fail before resorting to surgery (Wills Eye) |
| Miotics (pilocarpine) | Contraindicated — increase vascular permeability; miosis promotes posterior synechiae formation |
Key clinical pearl: If the patient is on topical steroids and IOP rises from multiple possible causes, stop the steroid for 2 days and remeasure. Long-acting depot preparations are contraindicated in known steroid-responders.
Surgical Treatment
Laser iridotomy — for pupillary-block angle closure; re-establishes posterior-to-anterior chamber communication. Iridotomy may occlude in active uveitis — use intensive topical steroids post-laser. Surgical iridectomy if laser fails.
Trabeculectomy with mitomycin C — used for medically uncontrolled IOP; requires:
- Control of uveitis for minimum 3 months before surgery
- Pre-operative topical (and possibly oral prednisolone 0.5 mg/kg/day for labile disease) steroids
- Post-operative steroids tapered more slowly than in non-inflammatory glaucoma
Glaucoma drainage devices (tube shunts) — often the preferred surgical option for uveitic glaucoma; better long-term IOP control than trabeculectomy alone in many series.
Cyclodestructive procedures — used with caution; risk of exacerbating inflammation and profound hypotony → phthisis bulbi.
Special Syndromes
Posner–Schlossman Syndrome (Glaucomatocyclitic Crisis)
- Rare condition; recurrent attacks of acute secondary open-angle glaucoma with mild anterior uveitis
- IOP markedly elevated during attacks (50–70 mmHg) but normalizes between episodes
Fuchs Uveitis Syndrome
- Chronic, low-grade, unilateral anterior uveitis; stellate KP diffusely distributed
- High risk of secondary glaucoma; medical control often inadequate; drainage devices offer best IOP control
Summary: Glaucoma Mechanisms in Anterior Uveitis at a Glance
Anterior Uveitis
│
├── Trabecular obstruction (cells, debris, trabeculitis)
│ └── Open-angle glaucoma
│
├── Posterior synechiae → Seclusio pupillae
│ └── Iris bombé → Angle-closure glaucoma (with pupillary block)
│
├── PAS from inflammatory angle deposits
│ └── Angle-closure glaucoma (without pupillary block)
│
├── Steroid response
│ └── Open-angle glaucoma
│
└── Neovascularization of iris/angle
└── Neovascular glaucoma
Sources: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed. (sections on Uveitic Glaucoma, pp. 399–406, and Anterior Uveitis, pp. 445–450); The Wills Eye Manual, 8th ed. (§12.1 Anterior Uveitis/Iritis/Iridocyclitis)
Treatment of episcleritis sceleritis conjunctivitis anterior uvietus glaucoma
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.