Everything about orchidectomy in detail surgery steps with reference to standard textbooks
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Searching Images
orchidectomy orchiectomy surgical steps inguinal incision spermatic cord
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive material from Hinman's Atlas of Urologic Surgery and Campbell-Walsh Wein Urology. Let me compose the complete, detailed answer.
Orchidectomy (Orchiectomy) — Complete Surgical Reference
Sources: Hinman's Atlas of Urologic Surgery, 4th Edition (Elmajian / Tanrikut & Goldstein, Chapters 109, 116, 117) • Campbell-Walsh-Wein Urology, 12th Edition (Chapters 77, 43) • Smith & Tanagho's General Urology, 19th Edition
1. Overview and Terminology
Orchidectomy (British) / Orchiectomy (American) refers to surgical removal of one or both testes. The procedure falls into four main categories depending on indication, approach, and extent of resection:
| Type | Approach | Extent |
|---|---|---|
| Radical (inguinal) orchiectomy | Inguinal | Testis + epididymis + spermatic cord to internal ring |
| Simple orchiectomy | Scrotal / subinguinal | Testis ± epididymis |
| Subcapsular orchiectomy | Scrotal | Testicular parenchyma only (tunica albuginea preserved) |
| Partial (testis-sparing) orchiectomy | Inguinal | Excision of mass + margin, testis preserved |
2. Indications
Radical (Inguinal) Orchiectomy
- Suspected or confirmed testicular malignancy (germ cell tumor — seminoma, NSGCT)
- Provides histological diagnosis, T-staging, tumor markers, local control
- Curative in 80–85% of clinical stage I seminoma and 70–80% of CS I NSGCT
- Contraindicated scrotal approach — alters lymphatic drainage, risks inguinal/pelvic nodal seeding
Simple Orchiectomy
- Bilateral: Androgen deprivation for prostate cancer; gender-affirming surgery (transgender women)
- Unilateral: Infected testis (abscess) refractory to antibiotics; non-viable testis (torsion, trauma); chronic orchialgia (last resort)
Subcapsular Orchiectomy
- Alternative to simple orchiectomy for castration; preserves scrotal contour and body image
Epididymis-Sparing Orchiectomy
- Castration while preserving epididymis for palpable scrotal bulk
Partial (Testis-Sparing) Orchiectomy
- Polar tumor ≤2 cm with compromised/absent contralateral testis
- Synchronous bilateral tumors
- Suspected benign lesion (up to 80% of lesions <3 cm with >6 months symptoms are benign)
Delayed Orchiectomy
- Diffuse metastatic GCT requiring urgent chemotherapy first; orchiectomy recommended after regardless of systemic response
3. Preoperative Assessment
History and examination: Testicular ultrasound is the primary imaging modality.
Serum tumor markers (before and after surgery):
- α-Fetoprotein (AFP)
- β-Human chorionic gonadotropin (β-hCG)
- Lactate dehydrogenase (LDH)
Staging imaging: CT chest/abdomen/pelvis with IV contrast (preferred preoperatively before radical orchiectomy to avoid confusion with postoperative retroperitoneal hematoma)
Anesthesia options:
- General anesthesia (most common for radical)
- Spinal/regional anesthesia
- Spermatic cord block ± conscious sedation (for simple orchiectomy)
Sperm banking: Should be offered before radical orchiectomy; intraoperative cryopreservation possible during testis-sparing procedures.
4. Radical Inguinal Orchiectomy — Step-by-Step
The gold standard for testicular malignancy.
Patient Positioning and Preparation
- Position: Supine on the operating table
- Skin prep: Abdomen to above the umbilicus, mid-thigh bilaterally, genitalia posteriorly to perineum
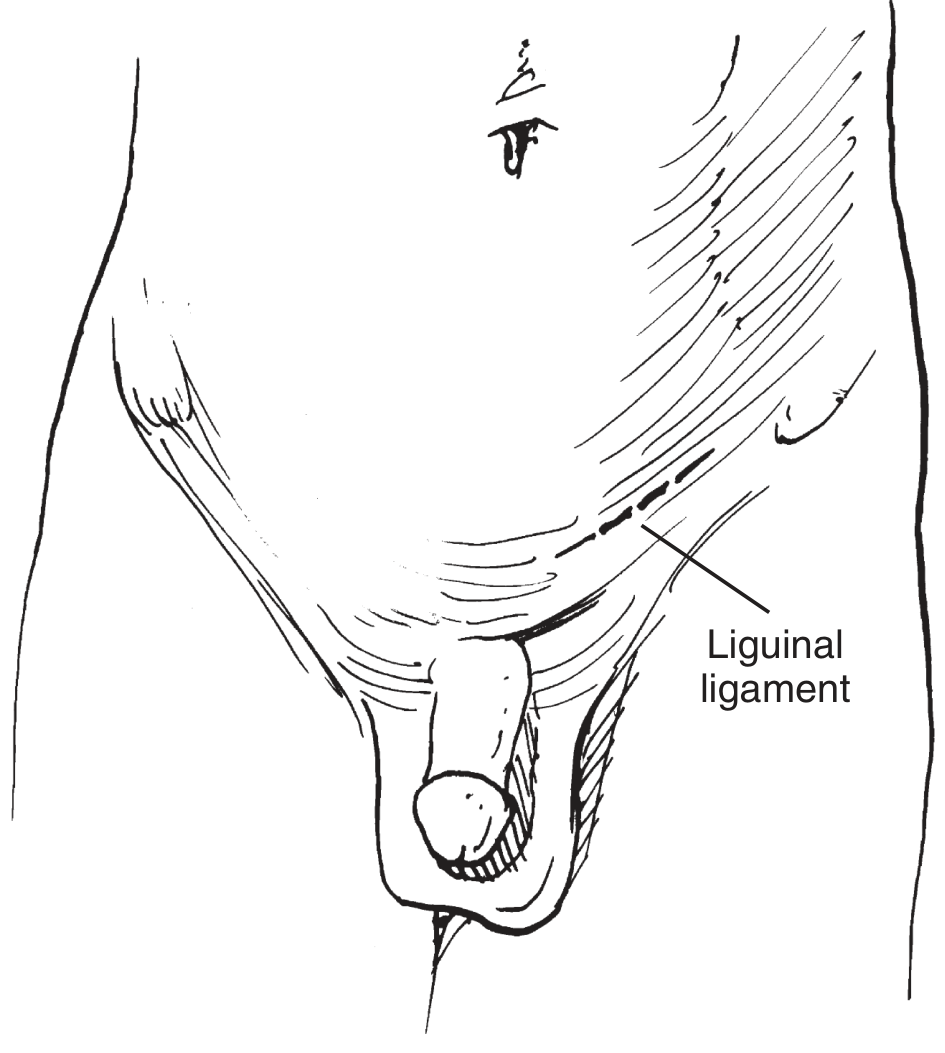
- Draping: Expose scrotum, ipsilateral ASIS, and pubic tubercle
- Examination under anaesthesia to locate the external inguinal ring
Step 1 — Skin Incision
- A 3–5 cm curvilinear/transverse incision is made 2 cm cephalad and lateral to the pubic tubercle, extending laterally along a Langer line for 5–7 cm
- The incision follows the inguinal crease overlying the inguinal canal
- For large tumours: extend obliquely toward the scrotum (hockey-stick or rotated orientation)
Step 2 — Superficial Dissection
- Incise through subcutaneous tissue (Camper and Scarpa fasciae are visible) using electrocautery
- Superficial inferior epigastric veins may be encountered laterally — carefully manage
- Expose the external abdominal oblique aponeurosis
Step 3 — Opening the External Oblique Aponeurosis
- Sharply incise the external oblique aponeurosis along the course of the inguinal canal, from the external inguinal ring medially to a point overlying the internal inguinal ring laterally (~4 cm)
- Weitlaner or Gelpi self-retaining retractors placed for exposure
Step 4 — Identify and Protect the Ilioinguinal Nerve
- The ilioinguinal nerve runs over the anterior aspect of the spermatic cord within the canal
- Identify it prospectively, dissect it free from its investing external spermatic fascia and cremasteric musculature, and retract it out of harm's way
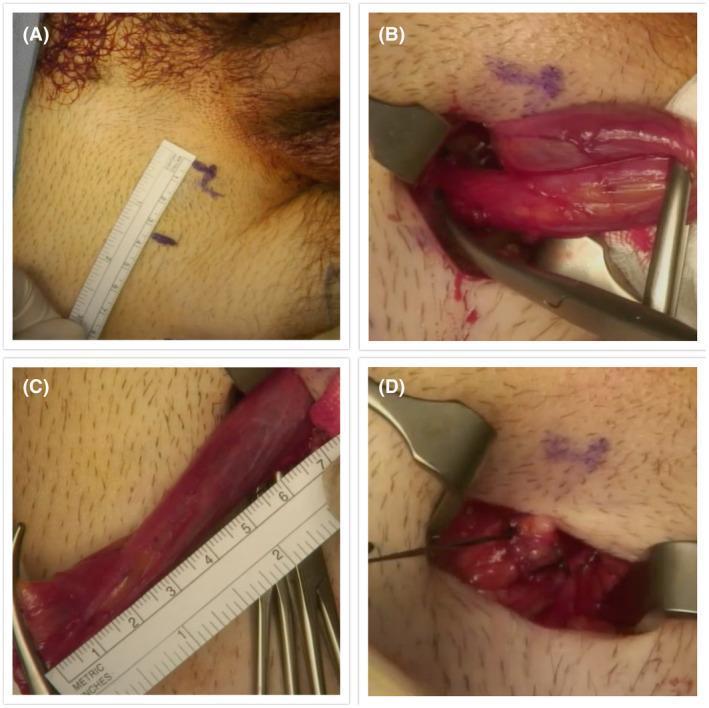
Step 5 — Mobilise and Encircle the Spermatic Cord (Early Vascular Control)
- Blunt dissection at the pubic tubercle to circumscribe the spermatic cord and cremasteric musculature
- The surgeon's finger passes posterior to the cord along the floor of the inguinal canal
- Caution: Avoid dissecting through the floor of the canal (risk of postoperative direct inguinal hernia)
- Encircle the cord with a ½-inch Penrose drain passed twice around and clamped with a haemostat — this provides early vascular control before any tumour manipulation
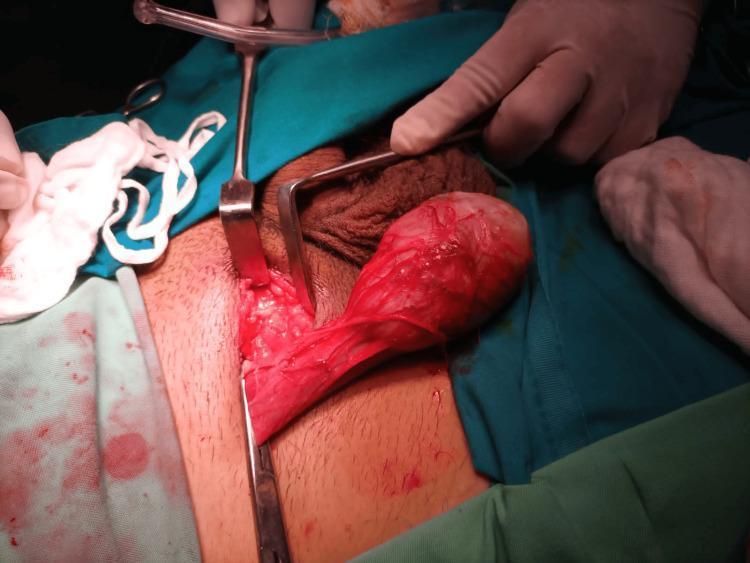
Step 6 — Testis Delivery
- The assistant gently pushes the testis from the base of the prepped hemiscrotum toward the incision
- The surgeon applies gentle traction on the spermatic cord to aid delivery
- The external spermatic fascia and cremasteric fibres are divided
- The gubernaculum is divided
- The testis is delivered intact within the tunica vaginalis into the operative field
- Isolated from the wound with sterile towels
Step 7 — Intraoperative Frozen Section (If Indicated)
- If the diagnosis is uncertain, a frozen section biopsy may be performed at this point before definitive ligation
- For testis-sparing: tumour is excised with 2–5 mm margin and sent for frozen section
Step 8 — High Ligation of the Spermatic Cord
- The cord is dissected proximal to the internal inguinal ring
- Cremasteric muscle fibres and external spermatic fascia are incised with electrocautery at this level, skeletonising the cord
- A hand-held retractor elevates the internal abdominal oblique musculature forming the lateral edge of the internal ring, revealing retroperitoneal fat
- The cord is further dissected proximally to visualise:
- Divergence of vas deferens from spermatic vessels
- Reflection of peritoneum overlying the cord anteromedially
Step 9 — Separate Ligation and Division
- Vas deferens is ligated and divided separately with 2-0 permanent (non-absorbable) suture
- Gonadal vessels (spermatic cord proper) are doubly ligated and divided with 0 permanent suture
- Preferred ligation with non-absorbable sutures with 1–2 cm suture tails — these act as markers for identification during subsequent retroperitoneal lymph node dissection (RPLND)
- Some surgeons drop the ligated stump into the preperitoneal space deep to the internal ring to facilitate future RPLND
Step 10 — Wound Irrigation and Haemostasis
- Irrigate the surgical field
- Achieve meticulous haemostasis
- Ilioinguinal nerve repositioned safely in the bed of the inguinal canal
Step 11 — Closure
| Layer | Suture |
|---|---|
| External oblique aponeurosis | Running 2-0 absorbable suture (care not to include ilioinguinal nerve) |
| Scarpa fascia | Interrupted 3-0 absorbable suture |
| Camper fascia | Interrupted 3-0 absorbable suture (bury knots) |
| Subcutaneous tissue | Horizontal mattress 4-0 absorbable suture |
| Skin | Running subcuticular 5-0 absorbable suture |
- Long-acting local anaesthetic (bupivacaine) injected before skin closure for postoperative analgesia
- Sterile dressings applied
- Scrotal support with fluff dressings added to reduce scrotal swelling and haematoma (especially useful for first 2–3 days)
5. Simple Orchiectomy — Step-by-Step
Used for castration (prostate cancer, gender-affirming), non-viable testis, or refractory orchitis.
Incision Options
- Transverse hemiscrotal incision within scrotal rugae (avoiding prominent vessels) — preferred for unilateral
- Longitudinal midline incision along the median raphe — for bilateral procedure (accesses both sides through one incision)
Steps
- Shave and sterile prep the scrotum
- Incise through dartos fibres and tunica vaginalis
- Deliver the testis into the wound; apply gentle traction to expose the spermatic cord
- Identify, ligate, and divide the vas deferens with 2-0 silk ligature
- Separate cremasteric muscle from the internal spermatic vessels
- Ligate each bundle separately with 2-0 silk sutures (vas deferens and remaining cord)
- Testicular prosthesis (if desired): leave gubernaculum and tunica vaginalis intact; place prosthesis inside the tunica vaginalis for natural position
- Meticulous haemostasis
- Dartos reapproximation: interrupted 3-0 or 4-0 absorbable suture
- Skin closure: inject with bupivacaine; running subcuticular 5-0 absorbable suture with skin hooks at apices
- Wound dressing: antibiotic ointment, fluffed gauze, athletic supporter
For bilateral procedure: repeat identical operation on contralateral side (separate incision or through the same median raphe incision).
6. Subcapsular Orchiectomy
Achieves castration while preserving scrotal volume and body image by retaining the tunica albuginea.
Steps
- Approach via scrotal incision as described for simple orchiectomy; deliver testis
- Incise the tunica albuginea
- Remove all testicular parenchyma (seminiferous tubules, Leydig cells) using blunt and sharp dissection
- Leave the tunica albuginea and epididymis intact — the tunica serves as a natural prosthesis
- Achieve haemostasis
- Close the tunica albuginea with absorbable suture
- Return within the tunica vaginalis; close the wound as for simple orchiectomy
7. Epididymis-Sparing Orchiectomy
Preserves the epididymis to maintain palpable scrotal bulk; uses operating microscope.
- Deliver testis as for simple orchiectomy
- Bring operating microscope into the field
- Sharply dissect epididymis off the testis
- Clamp and ligate the three major groups of epididymal vessels — superior, middle, caudal — with 2-0 silk
- Approximate caput and cauda of the epididymis with 3-0 absorbable suture → creates ellipsoid structure
- Insert a drain through a dependent stab wound (this is a bloodier operation than simple orchiectomy)
- Return epididymis to tunica vaginalis; close tunica vaginalis with 5-0 Vicryl
- Complete dartos and skin closure as for simple orchiectomy
Note: This procedure may increase the likelihood of epididymitis and leaves a palpable mass in the scrotum.
8. Partial (Testis-Sparing) Orchiectomy
Indications (Highly Selective)
- Polar tumour ≤2 cm, contralateral testis compromised or absent
- Synchronous bilateral tumours
- Suspected benign lesion; infertility concerns
- Contraindicated when a normal contralateral testis is present
Steps
- Initial approach identical to radical orchiectomy (inguinal incision, early cord control with Penrose drain)
- Deliver testis; isolate from wound with sterile towels
- Intraoperative ultrasonography for non-palpable lesions — needle localisation before tunica incision
- Cool testis with ice slush for 10 minutes to reduce warm ischaemia (some centres omit if resection <30 min)
- Occlude spermatic cord with two rubber-shod vascular clamps (cord and gubernaculum)
- Incise tunica albuginea in an avascular region under 10× magnification using a 15-degree microknife
- Blunt dissection through seminiferous tubules with microneedle holder until mass visualised
- Excise the mass with 2–5 mm margin of normal parenchyma using bipolar microforceps
- Frozen-section analysis — expert pathology input required
- Benign → preserve remainder
- Malignant + normal contralateral testis → proceed to radical orchiectomy
- Malignant + indication for organ-sparing → multiple random biopsies; preserve if negative margins and no intratubular germ cell neoplasia (GCNIS)
- If preserved: clamps released; haemostasis with bipolar cautery; tunica albuginea closed with running 5-0 absorbable suture; testis returned to tunica vaginalis (closed 4-0/5-0 absorbable)
- Wound closure: external oblique with 3-0 absorbable (running); Scarpa fascia 3-0 absorbable (interrupted); Camper fascia 3-0 absorbable (interrupted); subcutaneous 4-0 horizontal mattress; skin 5-0 subcuticular
- Adjuvant radiation (18–20 Gy) to remnant testis historically recommended for confirmed GCT; select patients can now be observed
9. Delayed Orchiectomy
For patients who require systemic chemotherapy before orchiectomy (diffuse metastatic GCT):
- Diagnosis may be made via biopsy of a metastatic site or presumptively on clinical/serological grounds
- Radical orchiectomy is still recommended after chemotherapy regardless of systemic response — discordant response rates exist between the testis and other metastatic sites
- For presumed extragonadal primary: GCNIS found in up to 42% of ipsilateral testis biopsies; 5% develop metachronous testicular cancer on observation
10. Postoperative Management
Immediate
- Scrotal support/athletic supporter for 2–3 days (reduces swelling and haematoma)
- Antibiotic ointment and gauze dressing
- Bupivacaine wound infiltration for analgesia
- Scrotal elevation
Staging After Radical Orchiectomy
- Repeat serum tumor markers (AFP, β-hCG, LDH) — trend in values guides management
- CT chest/abdomen/pelvis with IV contrast
- Note: PET and lymphangiography do not play a major role in initial staging
Pathological Examination of Specimen
Report must include:
- Histological tumour type and subtypes with percentages (for mixed GCT)
- Tumour size and multifocality
- Local invasion: rete testis, tunica albuginea, tunica vaginalis, epididymis, spermatic cord, scrotum
- Primary T stage (AJCC/UICC TNM)
- Lymphovascular invasion (LVI)
- Germ cell neoplasia in situ (GCNIS)
- Surgical margin status
11. Complications
| Complication | Notes |
|---|---|
| Haematoma/haemorrhage | Most common; prevented by meticulous haemostasis and scrotal support |
| Wound infection | Uncommon; antibiotic ointment prophylaxis |
| Ilioinguinal nerve injury | Numbness/hypoaesthesia of ipsilateral scrotum, inner thigh, root of penis; prevented by nerve identification and protection |
| Direct inguinal hernia | Avoid dissecting through the floor of the inguinal canal |
| Inguinal hernia | Recurrence of defect if aponeurosis not properly repaired |
| Lymphatic seeding/local recurrence | Consequence of scrotal approach for malignancy |
| Infertility/hypogonadism | Contralateral testis function must be assessed |
| Phantom scrotal pain | Can occur after simple orchiectomy; managed by genitofemoral nerve neuroma resection |
| Epididymitis | Especially after epididymis-sparing procedure |
| Vascular injury | Rare; care at internal ring |
12. Special Considerations
Testicular Prosthesis
- Can be placed at the time of radical orchiectomy (audit of 904 men confirms safety)
- For simple orchiectomy: place inside the intact tunica vaginalis with gubernaculum preserved for natural positioning
Bilateral Simple Orchiectomy
- Used for medical castration in prostate cancer — achieves castrate testosterone levels (<50 ng/dL) reliably and permanently
- Alternative to LHRH agonists; avoids injection-site reactions and compliance issues
- Consider subcapsular technique or epididymis-sparing for improved body image
Scrotal Violation (Oncological Principle)
Transcrotal biopsy or scrotal orchiectomy for a suspected malignant tumour is contraindicated because it:
- Leaves the inguinal portion of spermatic cord intact
- Alters testicular lymphatic drainage
- Increases risk of local recurrence and pelvic/inguinal nodal metastasis
References (Standard Textbooks)
- Hinman's Atlas of Urologic Surgery, 4th Edition — Elmajian DA (Ch. 117: Radical Orchiectomy); Tanrikut C, Goldstein M (Ch. 116: Simple Orchiectomy, Epididymis-Sparing Orchiectomy, Testis-Sparing Surgery); Ch. 109
- Campbell-Walsh-Wein Urology, 12th Edition — Chs. 77 (Testicular Cancer Management, Radical/Partial/Delayed Orchiectomy), 43, 28 (Orchiectomy for Chronic Scrotal Pain)
- Smith & Tanagho's General Urology, 19th Edition — Bilateral Orchiectomy
This is a shared conversation. Sign in to Orris to start your own chat.