Right hemicolectemy
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
I now have all the information needed for a comprehensive answer. Here is the full write-up:
Right Hemicolectomy
Definition and Extent of Resection
A right hemicolectomy is surgical removal of the terminal ileum (typically the distal 10 cm), cecum, appendix, ascending colon, hepatic flexure, and the proximal one-third of the transverse colon, along with the associated mesentery and lymphovascular pedicles. The bowel continuity is restored with an ileocolic (ileo-transverse) anastomosis.
The diagram below shows the difference between a standard right colectomy (cecum/ascending colon lesion) and an extended right colectomy (hepatic flexure/proximal transverse colon lesion):
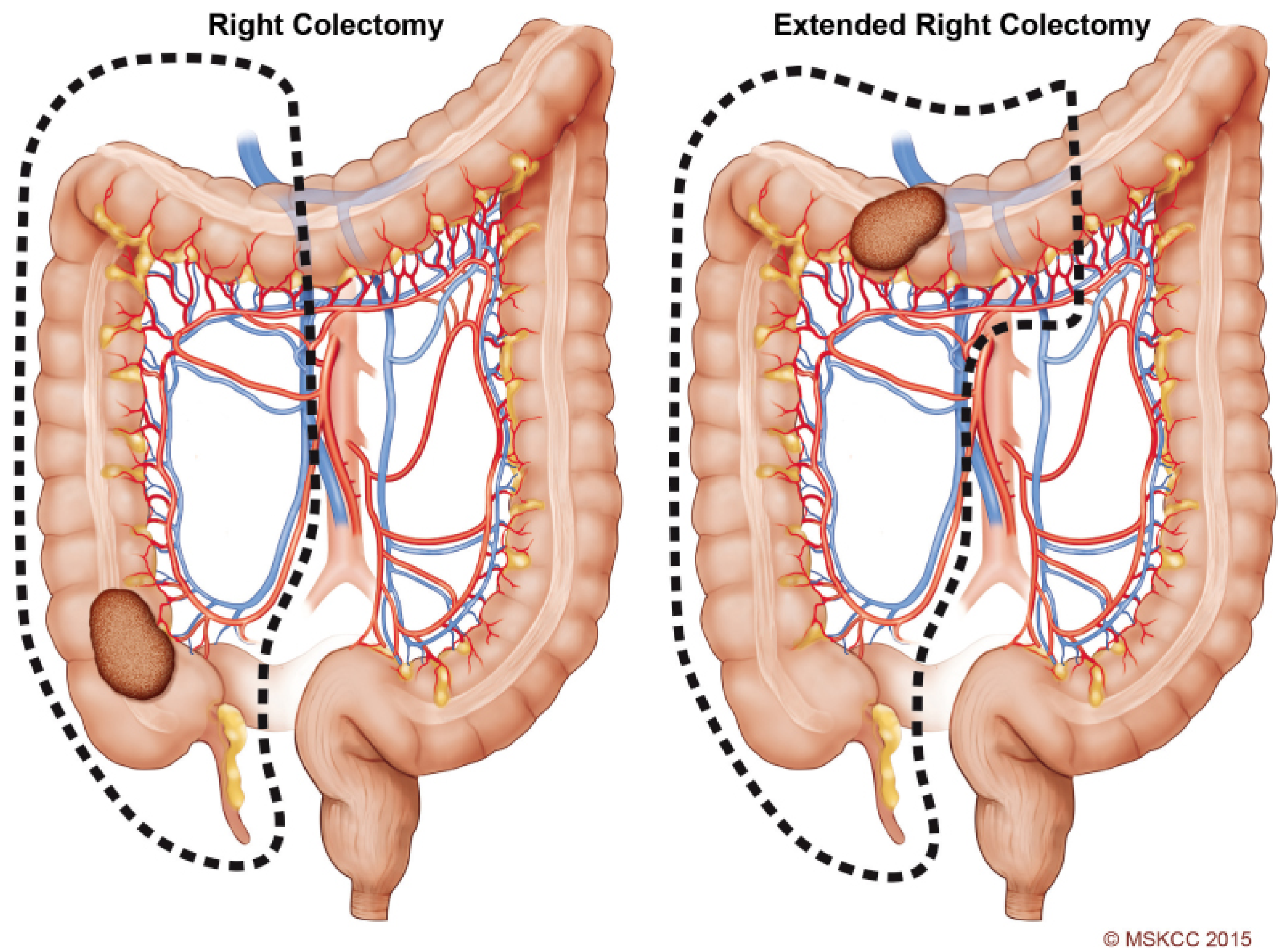
Figure 144.3 from Fischer's Mastery of Surgery, 8th ed.
Indications
- Invasive carcinoma of the cecum, ascending colon, hepatic flexure, or proximal transverse colon (most common)
- Malignant polyp with positive/unclear margins after polypectomy, or features predicting nodal metastasis (poor differentiation, vascular/lymphatic invasion, high tumor budding, deep submucosal invasion)
- Extended right hemicolectomy for proximal-to-mid transverse colon tumors, synchronous tumors, or multiple adenomas - the middle colic pedicle is ligated at its origin and the anastomosis is between terminal ileum and descending colon
- Crohn's disease involving the terminal ileum/cecum with ileocecal disease
- Cecal volvulus
- Appendiceal carcinoid >2 cm or with positive margins after appendectomy
- Right-sided colitis (ileocolic Crohn's disease)
Contraindications are relative. Laparoscopic/robotic approaches are more challenging with intestinal obstruction, large fistulizing tumors, or extensive adhesions from prior surgery. - Fischer's Mastery of Surgery, 8th ed.
Key Vascular Anatomy
The resection encompasses the lymphovascular territory of:
- Ileocolic artery - always ligated at its origin from the SMA ("high tie")
- Right colic artery - ligated at its origin (variable anatomy; absent in ~15%)
- Right branch of the middle colic artery - included in standard right hemicolectomy; the entire middle colic pedicle is taken in extended right hemicolectomy
Minimum 12 lymph nodes must be retrieved for accurate staging per oncologic guidelines. Complete mesocolic excision (CME) - dissecting along embryological planes with flush ligation of vessels at their SMA origin - is associated with improved outcomes in node-positive disease. - Bailey and Love's Short Practice of Surgery, 28th ed.
Preoperative Preparation
- Full colonoscopy and CT chest/abdomen/pelvis with IV contrast for staging
- Mechanical bowel preparation (polyethylene glycol) + oral antibiotics the day prior - reduces SSI, anastomotic leak, and postoperative ileus
- VTE prophylaxis: subcutaneous heparin, sequential compression devices, LMWH postoperatively, early ambulation
- IV antibiotics before incision, redosed during the case, discontinued postoperatively
- Enhanced recovery pathway (ERAS): carbohydrate loading 4 h preop, alvimopan preoperatively, transverse abdominis plane (TAP) blocks for MIS
- Goal-directed fluid therapy intraoperatively - Fischer's Mastery of Surgery, 8th ed.
Surgical Technique
Open Right Hemicolectomy
- Position: Supine, arms out. Midline incision with wound protector. Surgeon on the right, assistant on the left.
- Lateral mobilization: Assistant retracts the right colon medially; surgeon incises the lateral peritoneal reflection (white line of Toldt) with cautery along the right paracolic gutter.
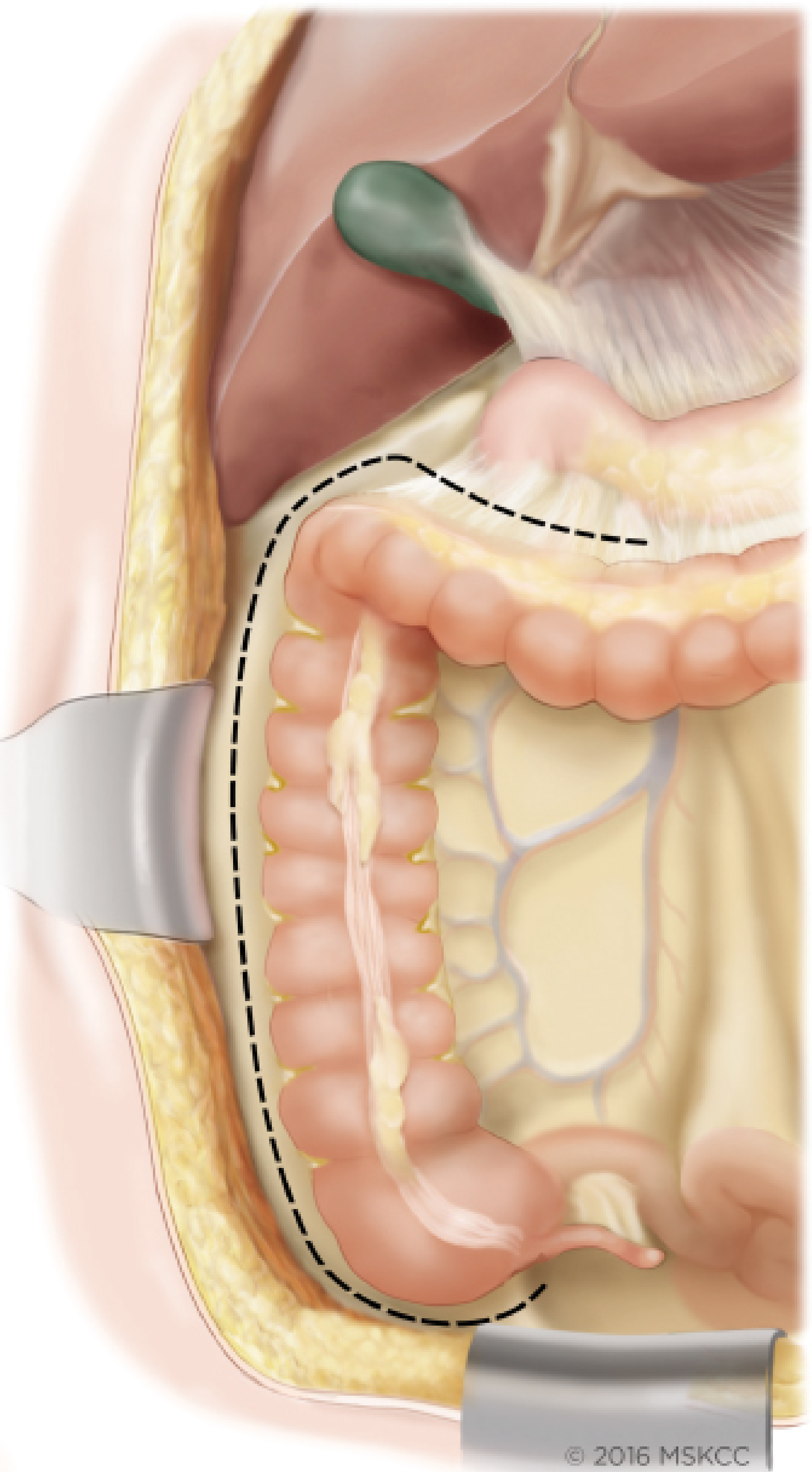
Figure 144.1 - Fischer's Mastery of Surgery, 8th ed.
- Retroperitoneal mobilization: The right colon is swept off Gerota's fascia, the duodenum, and the head of the pancreas. Care is taken around the small veins of the pancreatic head (suture ligation may be needed). The cecum and terminal ileum are dissected anteromedially, identifying and protecting the right gonadal vessels and right ureter (which stay in the retroperitoneum). Dissection extends to the third part of the duodenum.
- Hepatic flexure takedown: Cautery dissection continuing superiorly.
- Vascular ligation: The ileocolic artery (and right colic artery if present) are ligated at their origins from the SMA.
- Bowel division: Mesentery of the distal 10 cm of ileum and the mesocolon to the proximal transverse colon are divided. The greater omentum is divided to the transverse colon transection point.
- Anastomosis: An ileocolic anastomosis (side-to-side, functional end-to-end stapled, or hand-sewn) is performed once adequate blood supply at both margins is confirmed.
Laparoscopic Right Hemicolectomy
- Patient supine, both arms tucked, padded, strapped with anti-slip pad. Both surgeons stand on the patient's left side.
- Access via Veress needle at Palmer's point (3 cm below left subcostal border, midclavicular line) or Hasson cut-down.
- Port placement: 5-mm supraumbilical port (planned extraction site), three additional 5-mm ports in suprapubic, left upper, and left lower quadrants lateral to rectus.
- Table tilted: Trendelenburg, right side up - to expose ileocolic pedicle.
- A medial-to-lateral approach is standard: ileocolic pedicle identified first, peritoneum incised below it, retroperitoneal dissection plane developed before lateral mobilization.
- Specimen extracted via supraumbilical port site extension or Pfannenstiel incision.
- Anastomosis can be extracorporeal (most common) or intracorporeal.
Robotic Right Hemicolectomy
- Robot docked from patient's right side. Five-port approach (4 robotic + 1 accessory).
- Medial-to-lateral approach as with laparoscopic surgery.
- Advantages: enhanced 3D visualization, greater dexterity for CME dissection near SMA/SMV, particularly useful in obese patients and bulky lymphadenopathy. Trends toward lower conversion rate and higher rates of intracorporeal anastomosis.
- Limitation: Higher cost, longer OR time. In the only RCT comparing laparoscopic vs robotic right hemicolectomy, surgical and oncologic outcomes were equivalent.
Structures at Risk
| Structure | Risk |
|---|---|
| Right ureter | Division or thermal injury during retroperitoneal dissection |
| Right gonadal vessels | Traction/thermal injury |
| Duodenum (2nd/3rd part) | Direct injury during mobilization |
| Superior mesenteric vessels | Injury during high ligation |
| Small pancreatic head veins | Avulsion - suture ligation needed |
| Gerota's fascia / right kidney | Inadvertent entry |
Anastomosis
- Ileocolic anastomosis: Between terminal ileum and transverse colon
- Can be hand-sewn (single or two-layer) or stapled (side-to-side functional end-to-end)
- Both are oncologically equivalent; technique selected based on surgeon preference, tissue quality, and blood supply
- Extended right hemicolectomy: Anastomosis is between terminal ileum and distal transverse colon or descending colon, depending on vascular supply
- In elderly patients: note that loss of the ileocecal valve can increase daily bowel frequency significantly
Oncologic Principles (CME)
Complete Mesocolic Excision with Central Vascular Ligation (CME-CVL) mirrors the principles of TME for rectal cancer:
- Sharp dissection between parietal and visceral mesofascial layers (embryological planes)
- Flush ligation of vessels at SMA origin
- Retrieval of ≥12 lymph nodes mandatory for accurate staging
- CME may improve survival in node-positive disease (Hohenberger data) - Bailey and Love's, 28th ed.
Complications
With enhanced recovery protocols, the overall complication rate is 5-10%:
| Complication | Rate | Management |
|---|---|---|
| Anastomotic leak | <5% | Bowel rest, antibiotics, ± percutaneous drainage |
| Wound infection (SSI) | <5% | Local wound care |
| Postoperative ileus | Variable | ERAS protocols (alvimopan, early ambulation, limit opioids) reduce this |
| VTE | Low with prophylaxis | Heparin + SCD + early ambulation |
| Ureteral injury | Rare | Identification and protection during retroperitoneal dissection |
| Duodenal injury | Rare | Careful mobilization |
| Hemorrhage | Rare | Careful vascular ligation |
Outcomes Comparison: Open vs Laparoscopic vs Robotic
| Parameter | Open | Laparoscopic | Robotic |
|---|---|---|---|
| Hospital stay | Longer | Shorter | Similar to lap |
| Postoperative ileus | More | Less | Less |
| Pain | More | Less | Less |
| Conversion rate | N/A | ~5-15% | Lower than lap |
| Oncologic outcomes | Equivalent | Equivalent (COST trial) | Equivalent |
| Intracorporeal anastomosis | N/A | Less common | More common |
| Cost | Lowest | Moderate | Highest |
Prospective RCTs (including the COST trial) have proven laparoscopic colectomy is not inferior to open surgery with 5-year oncologic data. Minimally invasive approaches are preferred when expertise is available. - Fischer's Mastery of Surgery, 8th ed.
Sources:
- Fischer's Mastery of Surgery, 8th edition - Chapter 144 (Open Right Hemicolectomy, Laparoscopic Right Hemicolectomy, Robotic Right Hemicolectomy)
- Bailey and Love's Short Practice of Surgery, 28th edition - Chapter 77 (Operations: Right Hemicolectomy)
- Schwartz's Principles of Surgery, 11th edition - Figure 29-10 (Terminology of colorectal resections)
- Maingot's Abdominal Operations - Table 36-14 (Standard resections of the colon)
This is a shared conversation. Sign in to Orris to start your own chat.